
Abstract
Background:
Carcinoma ovary is very rarely associated with paraneoplastic cerebellar degeneration (PCD). The first clinical manifestations of primary malignancy could be associated with paraneoplastic symptoms. The presence of specific serum onconeural antibodies (Abs) in cerebellar ataxia patients may guide clinicians to search for the primary tumor by different investigation modalities.
Case:
A 71-year female presented with symptoms of gait ataxia and urinary incontinence. There were high levels of serum anti-Yo Ab and rapid progression of symptoms with no known etiology, which led to confirmation of PCD. The whole-body positron emission tomography-computed tomography scan showed multiple peritoneal and retroperitoneal metastases with normal adnexa. The histopathology of omental nodule showed high-grade serous carcinoma suggesting an occult primary ovarian cancer with PCD as a paraneoplastic syndrome.
Results:
The patient was treated with plasmapheresis and chemotherapy. Symptoms improved transiently after plasmapheresis. But, the general condition of the patient deteriorated gradually due to catheter-induced deep venous thrombosis, paraneoplastic neurologic symptoms, and metastatic disease status.
Conclusion:
Clinicians should have knowledge of paraneoplastic symptoms for early diagnosis and appropriate treatment, which will improve the quality of life by stabilizing the neurologic symptoms.
Introduction
The paraneoplastic disorder is not an unknown clinical manifestation in varieties of cancers. The nonspecific symptomatology is the main culprit for a delayed and/or incorrect diagnosis. There are a couple of cases reported on paraneoplastic cerebellar degeneration (PCD) associated with gynecologic malignancy. 1 We are presenting an even rarer case of PCD with occult primary ovarian cancer, who presented with gradually progressive gait and limb ataxia with urinary incontinence without symptoms of parkinsonism, cognitive and behavioral changes, and sensorineural deficits.
Case Report
A 71-year old postmenopausal female presented with imbalance while walking, difficulty in speaking, and urinary incontinence for 4 months. These symptoms were subacute in onset and gradually progressing with time. The patient had a change in behavior in the form of reduced interaction, reduced speech, and low mood. There was no history of forgetfulness and cognitive–behavioral changes. She had urinary incontinence and frequency. There were no symptoms of sensorineural deficits and increase in intracranial pressure. There was no history of similar complaints in any other family member.
General systemic and gynecologic examination findings were essentially normal. The Eastern Co-operative Oncological Group Performance Status (ECOG PS) was 2, in view of neurologic deficits. The neurologic clinical features were suggestive of cerebellar dysarthria, nystagmus, slow saccades, absent left ankle jerk, bradykinesia, left eye ptosis, wasting of small hand muscles, mild proximal weakness of all four limbs, extensor plantar reflex, intension tremors, gait, and limb ataxia. Overall patient's symptoms and clinical examination findings were suggestive of gait and truncal ataxia with urinary incontinence and dysarthria, probably pancerebellar dysfunction syndrome with autonomic dysfunction. Cerebrospinal fluid studies were within normal limits.
Magnetic resonance imaging (MRI) of brain was suggestive of age-related cerebral atrophy with periventricular demyelination and a focal 5 × 4 mm lesion in the left temporal lobe consistent with chronic focal hemorrhage. MRI of spine revealed mild multilevel disk (C3–C4, L1–L2, L2–L3, L3–L4, L4–L5, and L5–S1) protrusions with thecal sac indentation and narrowing of bilateral neural foramina. Nerve conduction studies and electromyography showed moderate mixed sensory motor, axonal, and demyelinating neuropathy. The autonomic function test expressed moderate loss in the parasympathetic reactivity with severe loss in cardiac autonomic tone.
Serum anti-Yo or anti-Purkinje cell antibody (Ab) 1 was strongly positive (3+) by enzyme immunoassay technique. Anti-Hu, anti-Ri, and other onconeural Abs of paraneoplastic disorder profile were negative. Tumor marker cancer antigen (CA) 125 and lactic dehydrogenase (LDH) were 982.9 U/mL (normal: <35 U/mL) and 53 U/L (normal: 200–420 U/L). Serum alpha-fetoprotein, carcinoembryonic antigen, and CA 19-9 were normal. Screening mammogram revealed bilateral small involuting fibroadenoma (Breast Imaging-Reporting and Data System category 2).
Fluorodeoxyglucose-positron emission tomography (PET) scan showed multiple avid lesions in bilateral internal mammary, anterior diaphragmatic, peritoneal, pelvic, retroperitoneal, omental, subcapsular hepatic, and serosal deposits (Fig. 1). Histopathology of omental nodule biopsy was consistent with high-grade serous carcinoma. On further evaluation with immunohistochemistry, the tumor cells were immunopositive for P53 and WT1 (Fig. 2). So, the final diagnosis was made as paraneoplastic subacute cerebellar degeneration with occult primary ovarian carcinoma.
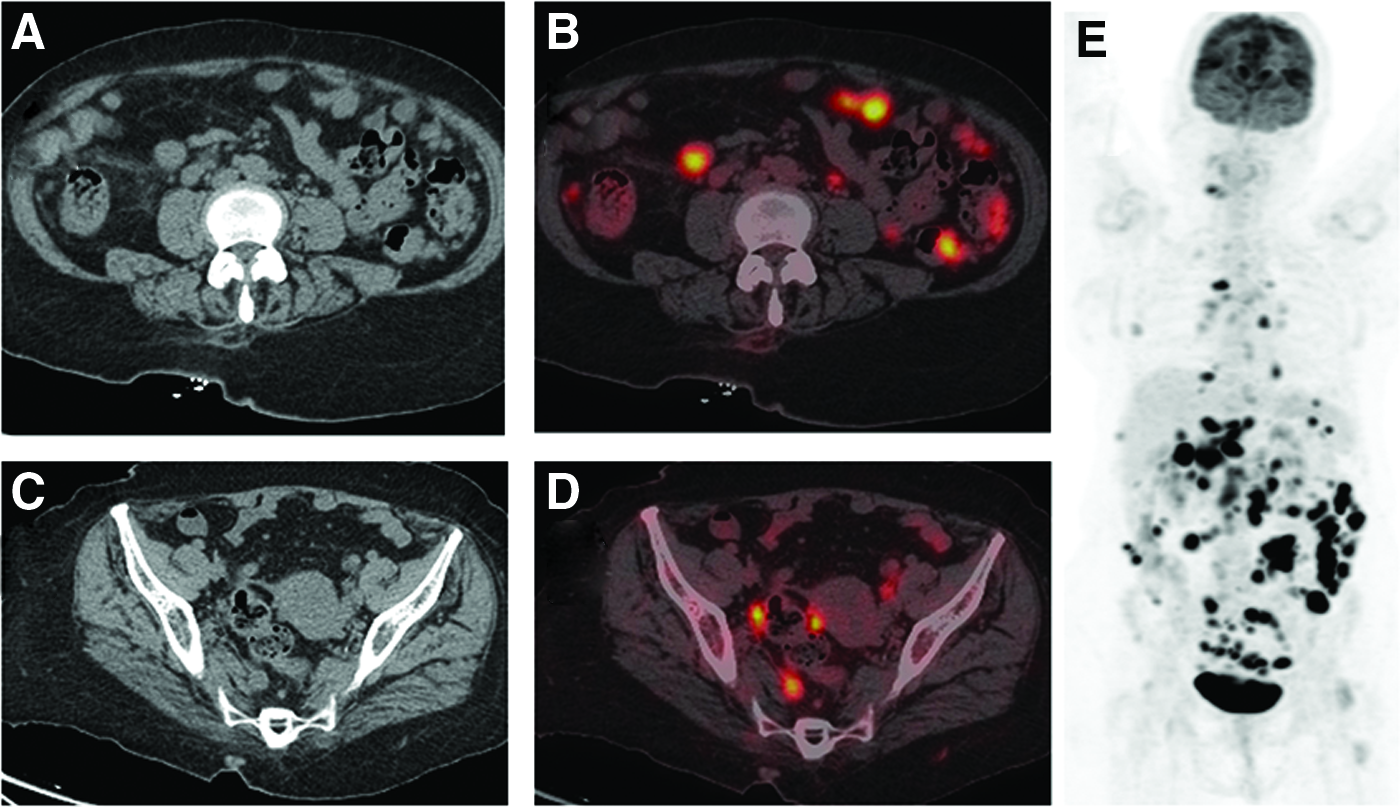
Transaxial CT

Microphotograph showing a high-grade serous carcinoma
The patient was treated with five cycles of plasmapheresis, after which the patient was symptomatically relieved. She received one cycle of chemotherapy (paclitaxel and carboplatin). She developed right lower limb deep vein thrombosis secondary to dialysis vascular catheter in situ. The patient's general conditions deteriorated gradually with time. Her ECOG PS became 3, limiting her to administer further cancer-directed treatment (surgery/chemotherapy/immunotherapy/targeted therapy). In a multidisciplinary tumor board meeting, the best supportive care with pain management and anticoagulant (rivaroxaban) was advised to the patient.
Discussion
We present a case of PCD with occult primary ovarian cancer, favored by raised serum anti-Yo Ab and CA 125 along with occult metastatic primary ovarian cancer. The latter was confirmed with histopathology and immunohistochemical studies. PCD is a heterogeneous group of neurologic disorders in a malignant tumor, caused by remote systemic effects of primary cancer or metastasis, 2 but not caused by direct involvement by tumor, metastasis, or antitumor treatment. The differential diagnoses of cerebellar and brain metastasis, toxic and metabolic causes, alcoholism, hypothyroidism, cerebrovascular disease, infectious cerebellitis, demyelination, or HIV should be specifically considered.
PCD is observed in <0.01% of all cancer patients. 3 The most commonly associated malignancies with PCD are small cell lung cancer, Hodgkin's lymphoma, and breast and gynecologic malignancies. 4 Both genders are affected with a preponderance to females, the reason being a more common association of PCD with gynecologic malignancies.
Pathogenesis of PCD is triggered with Ab-mediated humoral and cytotoxic T cell immune response. In the histologic examination, there is characteristically marked degeneration of Purkinje cells with minimal inflammatory infiltrates. 5 The immune system cross-reacts to tumor cells and neuronal antigens like the “Double Sword” mechanism. Any part of the brain may be affected in paraneoplastic syndromes, but cerebellum involvement is the commonest one. In 65%–80% of patients with PCD, isolated neurologic deficits may be the only presenting symptoms. 6 This may lead to diagnosing the underlying causative cancer in the early stage. However, the prognosis of disease may be masked by the severity of PCD-associated neurologic morbidities.
Diagnostic investigations begin with routine laboratory work-up and neuroimaging to rule out other possible causes. All onconeural Abs are associated with PCD. However, the most common Ab is an anti-Yo Ab and is associated with ovary, breast, and other gynecologic malignancies. Anti-Hu Ab is the second most common Ab. It is raised in small cell lung cancer and causes paraneoplastic encephalomyelopathy and Lambert–Eaton myasthenic syndrome. 7 In our patient, it is the strong positivity of the anti-Yo Ab that guided us for identification of underlying primary tumor by extensive diagnostic work-up, proving its diagnostic values in PCD. Since anti-Yo Ab is associated with a few specific cancers, it may be used as a biomarker in the PCD setting.
Paraneoplastic biomarkers should be quantified in both cerebrospinal fluid and serum. Nevertheless, the absence of these Abs does not exclude the possible diagnosis of PCD. The primary malignancy could be occult ovary or peritoneal serous carcinoma. The possible hypothesis is autolysis of the primary tumor by Abs. 5 The typical symptoms of our patient such as progressive gait instability, truncal, and both limbs ataxia with intention tremor match with those of PCD. The diagnosis of PCD is always a diagnosis of exclusion, which may be confirmed by the identification of paraneoplastic Abs and underlying malignancy. Rarely a patient may present with symptoms of primary malignancy before the onset of PCD clinical manifestations.
The neurologic outcome is dismal, despite low titer Abs by plasmapheresis and immunosuppressive strategies such as corticosteroids, immunoglobulins, plasmapheresis, and cyclophosphamide. 8 The modest clinical neurologic improvement with plasmapheresis and chemotherapy in this case might be due to irreversible neurologic damage by an onconeural Ab. Successful treatment of PCD is still limited with few reported significant clinical resolutions by the treatment of underlying cancer. 9
Conclusions
PCD is a disease of rare manifestations in common malignancy with poor oncologic, neurologic, and overall clinical outcomes. It has a poor prognosis to date regardless of the treatment. This report is certainly of value in that it increases awareness of this neurologic condition and earlier diagnosis reduces confusion, avoids further unnecessary interventions, and allows for potentially beneficial directed treatment.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose and no conflicts of interest.
Funding Information
No funding was received for this article.