
Abstract
Background:
The surgical management of ovarian cancer is performed conventionally by laparotomy. The role of minimally invasive surgery has been highlighted in early stage disease, assessment of resectability and second-look surgery. However, laparoscopy in cytoreductive surgery for advanced ovarian cancer has not been established. The aim of this report is to demonstrate the role of the minimally invasive approach to primary cytoreductive surgical treatment of advanced ovarian cancer.
Case:
A 38-year-old multiparous woman presented with a gradually enlarging abdominal mass. A preoperative work-up showed that she actually had bilateral ovarian masses with extensive peritoneal carcinomatosis. The patient underwent laparoscopic cytoreductive surgery (hysterectomy, bilateral salpingo-oophorectomy, peritoneal fluid cytology, anterior and posterior pelvic peritonectomy, bilateral pelvic node dissection, low anterior resection with colo–anal reanastomosis, partial hepatectomy, right subdiaphragmatic peritonectomy, and ablation of liver and subdiaphragmatic peritoneal nodules) performed by a multidisciplinary team of gynecologic oncologists, as well as colorectal and hepatobiliary surgeons.
Results:
This patient's estimated blood loss was 350 mL. There were no intraoperative or postoperative complications. The histopathology result showed high-grade serous carcinoma of the bilateral ovaries with metastasis to the omentum, subdiaphragmatic peritoneum, and liver capsule. The final surgicopathologic stage was IIIC. The patient received her first course of adjuvant chemotherapy 11 days postsurgery with no adverse events and was discharged in an improved condition.
Conclusions:
Minimally invasive cytoreductive surgery for advanced ovarian cancer is a safe and feasible procedure. Laparoscopy enables better visualization of tumor involvement, ensuring complete removal of all visible disease. It allows for faster recovery, leading to a shorter interval to chemotherapy initiation.
Introduction
The conventional approach to the management of patients with ovarian cancer is through laparotomy. A midline vertical incision is performed in order to carry out hysterectomy, bilateral salpingo-oophorectomy, peritoneal biopsies, bilateral pelvic lymph-node dissection, para-aortic lymph-node dissection, omentectomy, and debulking. The goal of surgery is to remove all visible macroscopic disease because optimal cytoreductive surgery has been shown to confer a significant survival benefit in patients with advanced ovarian cancer. 1
The minimally invasive surgical approach in ovarian cancer has been shown to be applicable in the management of early stage disease, diagnostic laparoscopy to obtain a biopsy for cases with advanced disease recommended for neoadjuvant chemotherapy, assessment of resectability of advanced ovarian disease, and second-look surgery for patients who received neoadjuvant chemotherapy. The use of laparoscopy in complete cytoreductive surgery for advanced ovarian cancer has yet to be validated. This article presents the case of a patient with advanced ovarian disease with extensive peritoneal spread who underwent primary cytoreductive surgery with laparoscopy performed by a multidisciplinary team of oncologic surgeons.
Case
The patient was a 38 year old gravida 2, para 2, female, who had a palpable left lower abdominal mass enlarging over a course of 4 months. There was an associated weight loss of 5 kg in 2 weeks. A complete work-up was performed, including an abdominal computed tomography scan. The scan showed that she actually had bilateral ovarian masses with concerning potential presence of tumor rupture and peritoneal spread with the presence of multiple peritoneal nodules in the pelvic cavity, periappendiceal area, bilateral paracolic gutter, and perihepatic space. Her tumor markers, including cancer antigen (CA)–125 and CA 19-9, were elevated.
This patient underwent laparoscopic cytoreductive surgery under general anesthesia. Closed entry, using a Veress needle was performed, and the primary port was placed at the Lee-Huang point with 4 5-mm lateral ancillary ports in the mid-to-lower abdomen. Careful inspection of the abdomen and pelvis was performed. Ascitic fluid was aspirated and sent for cytology analysis. Intraoperatively, there was abdominopelvic carcinomatosis over the anterior pelvic peritoneum, uterine serosa, bilateral ovaries, fallopian tubes, bilateral paracolic gutters, and cul de sac with involvement of the rectosigmoid colon. The tumor involvement of the rectum was 8 cm proximal to the anal verge. The omentum was caked with tumor involvement close to the transverse colon, especially on the right side of the omentum. Tumor peritoneal seeding was spread over the liver surface and the right and left subdiaphragmatic surfaces.
The gynecologic oncologic service performed laparoscopic hysterectomy, bilateral salpingo-oophorectomy, peritoneal fluid cytology, anterior and posterior pelvic peritonectomy, bilateral pelvic lymph-node dissection, and omentectomy. The omentum was excised from the inferior margin of the transverse colon, using a LigaSuretm advanced bipolar device. The colorectal surgery service performed laparoscopic low anterior resection using a 60-mm GIAtm stapler and performed colo-anal reanastomosis. The descending colon was mobilized to the level of the splenic flexure, and the mobilized proximal sigmoid colon was brought out through the vagina. A 33-mm end-to-end anastomosis stapler was inserted into the rectum, and the spike was connected to the anvil and activated, resulting in the end-to-end anastomosis. The rectum was then insufflated with air to check for leakage, which was negative. The hepatobiliary surgery service performed laparoscopic partial hepatectomy of segment 8 and a right subdiaphragmatic peritonectomy. An additional upper abdominal port was placed. The tiny right liver nodules and left subdiaphragmatic peritoneal nodules were ablated. All specimen were placed in endoscopic bags and removed through the vaginal vault (Fig. 1). No specimen samples were extracted through any of the trocar ports. Copious washing of the abdominopelvic cavity, vaginal vault, and port sites was performed.
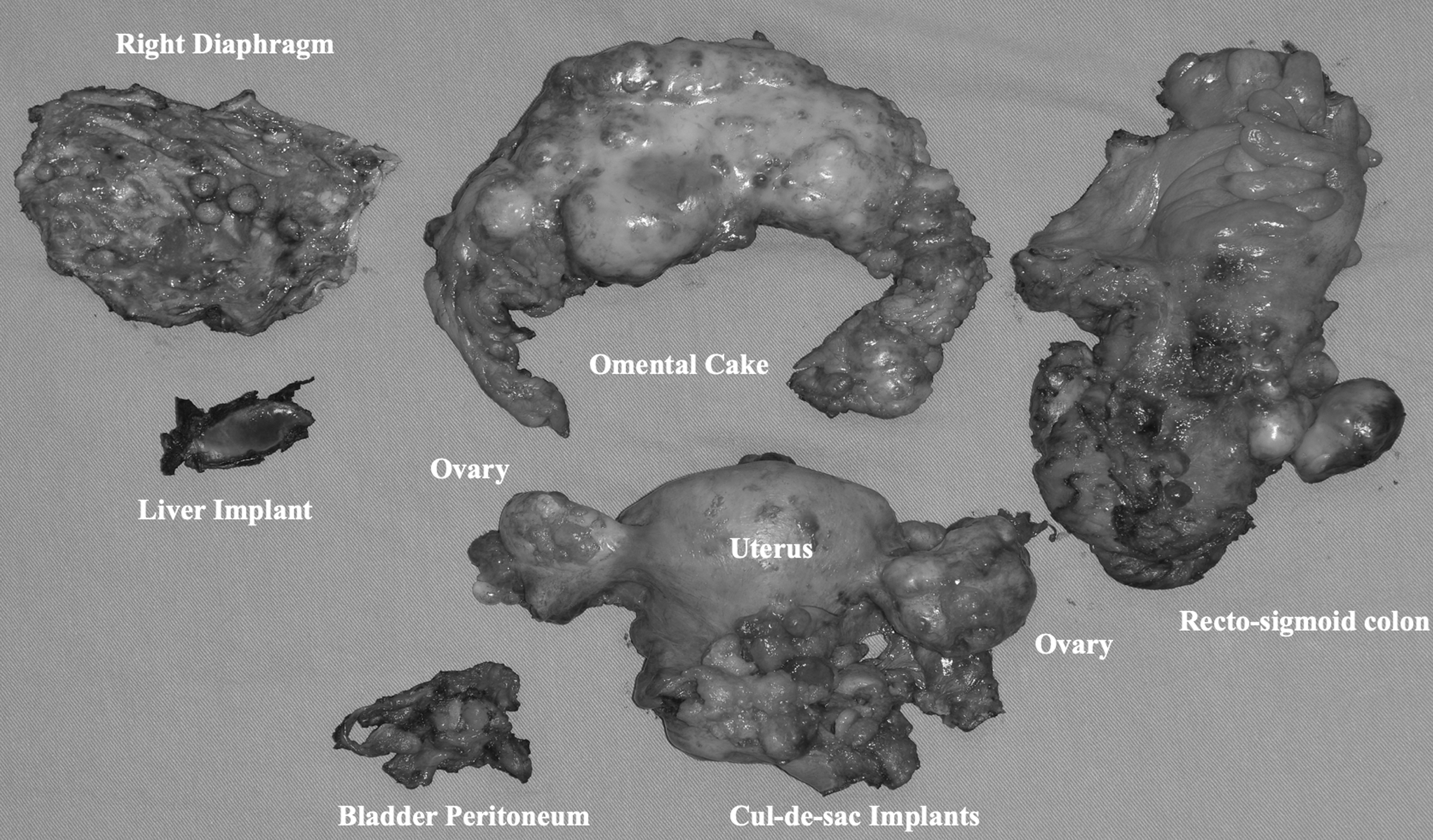
Specimens showing the uterus with bilateral ovaries, bladder peritoneum, liver implant, right subdiaphragmatic peritoneum, omentum, and rectosigmoid colon, etc.
Results
The patient's estimated blood loss (EBL) was 350 mL for the entire procedure. She was stable throughout the procedure with no episodes of hypotension or desaturation. She had an uneventful postoperative course and did not experience fever, severe abdominal pain, ileus, or bladder dysfunction. The final histopathology result showed high-grade serous carcinoma of the bilateral ovaries with metastasis to the right fallopian tube, right and left pelvic lymph nodes, omentum, bladder peritoneum, rectum, subdiaphragmatic peritoneum, and capsular surface of segment 8 of the liver. The ascitic fluid was positive for atypia. The surgicopathologic stage of the patient was IIIC. She received the first course of adjuvant chemotherapy with carboplatin–paclitaxel 11 days postsurgery. There were no adverse events.
The hospital's institutional review board ruled that approval was not required for this report. Written informed consent was obtained from the patient for publication of this case report and accompanying image.
Discussion
Comprehensive surgical staging and optimal cytoreduction are essential in the management of advanced ovarian cancer. Optimal cytoreduction is the most-significant prognostic factor that confers a survival benefit to these patients.1,2 Diagnostic laparoscopy use in advanced ovarian cancer has been described with respect to obtaining biopsy samples prior to neoadjuvant chemotherapy, assessment of resectability, and second-look surgery after laparotomy cytoreduction and chemotherapy. The authors of several retrospective studies have advocated that minimally invasive surgical approaches may be a tool in the evaluation of patients with advanced disease who can undergo maximum cytoreduction.3–5 With the use of open laparoscopy wherein laparoscopy is primarily used to determine where optimal debulking is possible, there is a significant improvement in the rate of optimal debulking from 61% to 96%, and the appropriate patients are determined to be suitable for cytoreductive surgery. 5 A randomized controlled trial demonstrated that diagnostic laparoscopy reduced the number of futile laparotomies in patients with suspected advanced-stage ovarian cancer. 6 However, these studies still limit the use of laparoscopy to only the diagnostic work-up of patients with suspected advanced ovarian cancer.
The application of minimally invasive surgical cytoreduction for advanced ovarian cancer was first described by Amara et al. 7 That case series included 5 patients who underwent primary staging or secondary cytoreductive surgery, and all of those patients had good postoperative courses. The safety and efficacy of laparoscopic surgical staging for advanced-stage ovarian cancer was demonstrated in a retrospective study including 32 patients who underwent laparoscopic evaluation (17 patients underwent primary cytoreduction, 11 patients underwent diagnostic laparoscopy converted to laparotomy for cytoreduction, and 4 patients underwent limited cytoreduction). 4 That study showed that EBL was lower and hospital stays were shorter for the study's laparoscopy group The operative time and complication rates were similar among the study groups. The absence of trocar complications was notable, particularly port-site metastasis. Furthermore, there was a longer recurrence-free interval in the laparoscopic-debulking group, compared with the open-surgery group. 4
Another small series showed that 9 of 11 patients with primary advanced ovarian cancer underwent successful laparoscopic cytoreductions. Two patients were converted to laparotomy because the first patient had extensive omental metastasis and the second patient had bulky metastasis involving the rectosigmoid. 8 Laparoscopy is not a deterrent to upper abdominal disease debulking or extensive gastrointestinal invasion. Omental disease, liver metastases, and subdiaphragmatic peritoneal tumor implants may be resected laparoscopically by skilled surgeons. Bowel resection as part of debulking surgery may also be performed. Despite the presence of widespread disease, performance of the comprehensive debulking surgery does not increase possible surgical complications dangerously. Operative time might be increased but the length of hospitalization is reduced and complication rates are comparable to open surgery. 9
Concerns about laparoscopic surgical staging include the possibility of cyst rupture and subsequent intraoperative tumor spill, tumor spread due to pneumoperitoneum, and port-site metastasis. Intraoperative tumor rupture will lead to upstaging of the disease and could lead to tumor spread. A meta-analysis concluded that intraoperative rupture does not reduce progression-free survival compared to no rupture in early stage ovarian cancer with complete surgical staging followed by chemotherapy. 10 The role of CO2 pneumoperitoneum in the spreading malignant cells is not understood fully. Some studies show that pneumoperitoneum contributes to implantation of the tumor in wound sites. Port-site metastasis can result from advanced malignancy, direct contamination of cancer cells following extensively unprotected manipulation or presence of ascites, gas leak at the port sites, and tissue acidosis caused by the use of carbon dioxide. 11
With the advances in the field of minimally invasive surgery and improvement in the instruments and proficiency of the surgeons, comprehensive surgical staging and cytoreduction can be performed for patients with advanced stage disease. Laparoscopy offers improved visualization of the abdominopelvic structures, reduction in postoperative pain, shorter hospital stay, faster recovery time, and shorter interval to the initiation of chemotherapy, which is important in patients with advanced ovarian cancer.
Conclusions
Laparoscopic cytoreductive surgery is a viable option for patients with advanced ovarian cancer. The widespread extent of disease does not hinder the performance of complete surgical staging and may include upper abdominal disease resection and bowel resection performed by a multidisciplinary team of proficient surgeons.
Footnotes
Acknowledgments
The authors thank the Asia-Pacific Association for Gynecologic Endoscopy and Minimally Invasive Therapy (APAGE) for providing the International Fellowship in Minimally Invasive Gynecologic Surgery at Chang Gung Memorial Hospital for Dr. Mendoza.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
The authors did not receive a specific grant for the preparation of this report from any funding agencies in the public, commercial or nonprofit sectors.