
Abstract
Background:
With advancements in surgical techniques and equipment, successful laparoscopic management has been reported in selected cases of iatrogenic uterine perforation. However, management of iatrogenic uterine perforation by laparoendoscopic single-site surgery (LESS) has never been described in a case series.
Cases:
Case 1: In a 36-year-old woman, uterine perforation with omental injury was induced by placenta forceps during evacuation of a retained placenta and managed by LESS hemostatic suturing of the uterine wound, followed by extracorporeal ligation of the injured omental vessels. Case 2: In a 28-year-old woman, uterine perforation without visceral injury was induced by Pean's forceps during unsuccessful removal of an intrauterine device and was managed by hysteroscopic-assisted removal of the device, followed by LESS compression hemostasis of the uterine perforation. Case 3: In a 29-year-old woman, uterine perforation with a small-bowel injury was induced by placenta forceps during removal of a retained placenta and managed by LESS hemostatic suturing of the uterine wound, followed by extracorporeal resection and re-anastomosis of the injured ileum.
Results:
Three cases of iatrogenic uterine perforation during intrauterine manipulation were managed successfully, with no significant surgical complications, by LESS surgery.
Conclusions:
A minimally invasive approach with LESS surgery could be a feasible option for management of iatrogenic uterine perforation.
Introduction
Uterine perforation is a rare but recognized iatrogenic complication associated with various forms of intrauterine manipulation.1–3 When uterine perforation is assumed to be complicated by injury of nearby organs, such as the bowel,1–3 this is a potentially life-threatening condition that requires immediate intervention, followed by repair of injured organs when they are identified.1,2
With recent advances in surgical equipment and techniques, it has been shown that a minimally invasive approach utilizing laparoscopy is a feasible option for diagnosing1,2 and treating3,4 uterine perforation and its associated organ injuries in selected cases.
Transumbilical laparoendoscopic single-site (LESS) surgery is now being used increasingly in various forms of general5,6 and gynecologic7,8 surgeries. However, the feasibility of this form of minimally invasive approach for the diagnosis and management of iatrogenic uterine perforation has never been reported.
This article herein reports on 3 cases of iatrogenic uterine perforation that were managed successfully by LESS surgery7,8 without subsequent major complications.
Cases
Case 1
A 36-year-old (gravida 2 para 1) woman was referred 17 days after an uneventful vaginal delivery; she now had complaints of persistent febrile morbidity. With a diagnosis of an infectious retained placenta, uterine evacuation was performed. After removal of most of the placenta tissue by vacuum aspiration, attempts were made to remove the remnants with placenta forceps. Tissue thought to be placental remnants was grasped, twisted, and pulled, but the removed tissue had the appearance of omental fat tissue.
Now with a diagnosis of iatrogenic uterine perforation with potential visceral injury, emergency LESS surgery was performed. Under laparoscopic visualization, significant hemoperitoneum was confirmed (Fig. 1A). Continuous bleeding was observed from a myometrial perforated injury at the posterior uterine wall near the fundus (Fig. 1A, arrow). The injured portion was reapproximated by intracorporeal suturing and extracorporeal knot-tying (Fig. 1B).
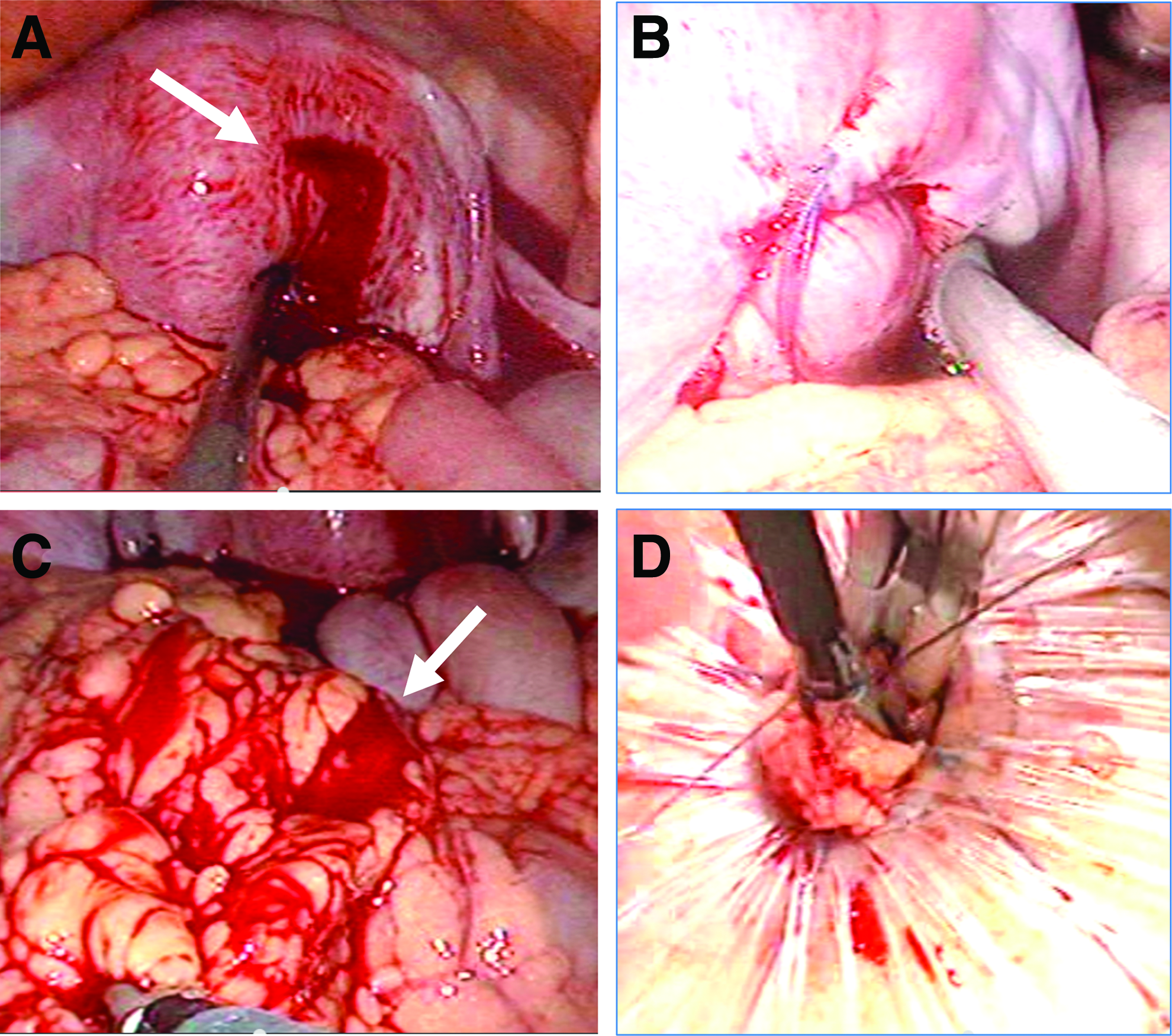
Subsequently, continuous bleeding from the injured omental tissue was identified (Fig 1C, arrow); however, no apparent bowel injury was evident. The injured portion of the omental tissue was carefully grasped and exteriorized through the umbilical incision, and hemostasis was achieved by extracorporeal ligation of the injured blood vessels (Fig. 1D).
Case 2
A 28-year-old (gravida 4 para 4) woman was transferred due to severe abdominal pain and vaginal bleeding after an attempt to retrieve a levonorgestrel-releasing intrauterine system (Mirena®; Bayer, Whippany, NJ) using Pean's forceps failed.
At triage, on contrast-enhanced computed tomography (CT), the retained Mirena device was identified in the uterine cavity (Fig. 2A, arrow). An oblique contrast-unenhanced structure across the myometrium at the lower portion of the posterior uterine wall suggested uterine perforation (Fig. 2A, arrowhead).
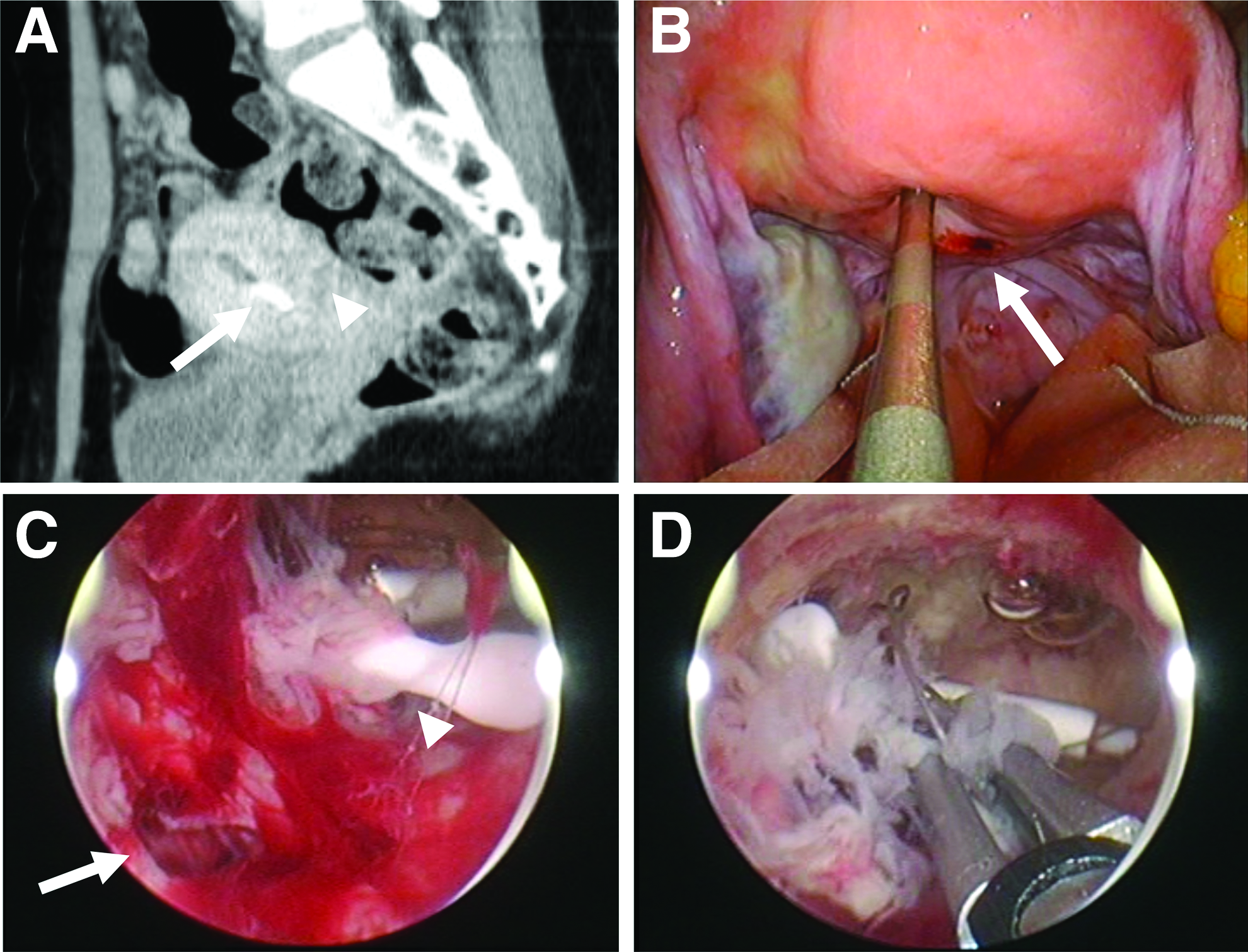
Emergency LESS surgery with hysteroscopic-assisted removal of the device was attempted. Under laparoscopic vision, uterine perforation with subtle but continuous oozing was identified at the right posterior wall of the lower uterine body near the cul-de-sac (Fig. 2B, arrow).
Under hysteroscopic observation, uterine perforation was detected at the right posterior wall of the lower uterine body (Fig. 2C, arrow). The displaced Mirena device identified in the uterine cavity (Fig. 2C, arrowhead) was grasped transcervically with laparoscopic forceps under hysteroscopic guidance (Fig. 2D) and removed from the uterine cavity through the cervical canal.
Thereafter, hemostasis of oozing from the perforated uterine wall was achieved by compression with oxidized, regenerated cellulose sheets.
Case 3
A 29-year-old (gravida 1 para 1) woman was transferred due to uterine perforation with prolapse of the small bowel through the cervical canal by placenta forceps when uterine evacuation was performed to manage a retained placenta that was diagnosed 1 month after an uneventful vaginal delivery.
Magnetic resonance imaging (MRI) showed an oblique hyperintense structure at the anterior myometrial wall with focal disruption of the junctional zone, indicating uterine perforation (Fig. 3A, long arrow). Peritoneal effusion suggesting hemoperitoneum (Fig. 3A, arrowhead) and presumed retained placental tissue in the cervical canal (Fig. 3A, short arrow) were also recognized. CT images revealed spotty free air in the mesentery of the small intestine (Fig. 3B, arrow), strongly suggesting small-bowel injury.
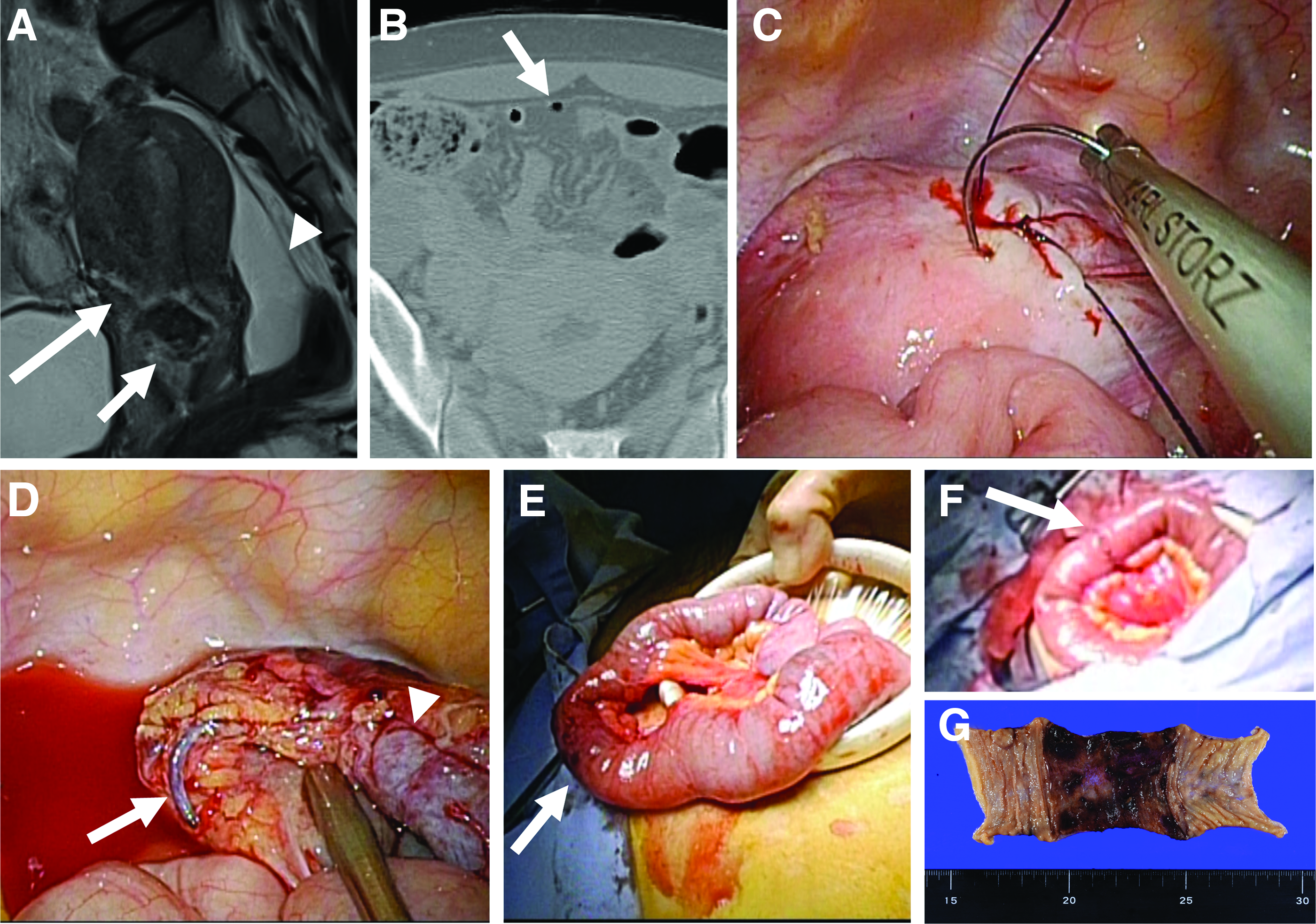
Emergency LESS surgery was performed. Under laparoscopic vision, continuous active bleeding was identified from the perforated wound over an area measuring 2 cm. This perforated wound was reapproximated intracorporeally by suturing using 0 monofilament Stratafixtm barbed sutures (Ethicon, Somerville, NJ; Fig. 3C).
Thereafter, although no apparent intestinal excretion was observed in the peritoneal cavity, severe ileal devascularization with laceration of the versa recta and mesentery (Fig. 3D, arrow) as well as exfoliation of the intestinal serosa (Fig. 3D, arrowhead) were identified.
With the assistance of gastrointestinal surgeons, the injured portion of the ileum was completely exteriorized through the umbilical working port (Fig. 3E, arrow). Under direct vision, the injured portion of the ileum (10 cm) was excised and end-to-end anastomosed by extracorporeal manual suturing (Fig. 3F, arrow).
Results
In Case 1, the duration of surgery was 60 minutes, and the intraoperative blood loss was 100 mL. The postoperative course was complicated by prolonged resolution of an inflammatory reaction, which was managed conservatively by extended administration of antibiotics. On postoperative day 13, the patient was discharged from the hospital, and thereafter, the postoperative course was uneventful.
In Case 2, the duration of surgery was 58 minutes, and the intraoperative blood loss was 50 mL. Four days after surgery, the patient was discharged from the hospital. The subsequent postoperative course was uneventful.
In Case 3, the duration of surgery was 97 minutes, and the intraoperative blood loss was 210 mL. The postoperative course was uneventful. The patient was discharged from the hospital 4 days postoperatively. A pathologic examination showed severe localized necrotic changes in the excised ileum (Fig. 3G).
Discussion
Intrauterine manipulations are procedures commonly performed worldwide with good safety records. 2 However, one of the most serious complications during this procedure is uterine perforation. 2 Perforation with blunt instruments, such as a Hegar dilator, will not generally cause any serious harm.1,2 In such occasions, expectant management may be sufficient, with no need for surgical closure of the perforated uterine wound in most cases.1,2 However, even in such cases, if the original procedure is not completed and associated injury of nearby organs is of concern, completion of the procedure along with management of the uterine perforation, preferably through laparoscopic guidance, may be a safe and feasible option, as was chosen for Case 2.
However, when perforation occurs with thermal, avulsion, or suction instruments, the immediate consequences are hemorrhaging and/or associated injury of nearby organs, such as the bowel,1–3,9 as was observed in Cases 1 and 3.
Uterine perforation is usually initially diagnosed as a result of operator suspicion. 2 In Case 1, because uterine perforation with omental exteriorization occurred in the operating room, an immediate laparoscopic examination was chosen.
In contrast, for women, such as in Cases 2 and 3, who are referred from other clinics, a further precise evaluation of uterine perforation and associated organ injuries, using CT 9 and/or MRI, 10 are likely to be more informative for determining the extent of the visceral damage and thereafter deciding on the treatment strategy, especially for laparoscopy versus laparotomy, at triage.
When emergency intervention is required due to a strong suspicion of uterine perforation, the choice of the initial surgical approach—laparotomy or laparoscopy—depends on the patient's hemodynamic stability, the likelihood of significant intra-abdominal hemorrhaging, and the suspicion of injury to the nearby visceral organs, such as the bowel. 4 Additional considerations include the surgeon's experience with laparoscopic surgery in emergency situations. 4
If uterine perforation can be managed laparoscopically by either hemostatic suturing or electrosurgical coagulation, a further laparoscopic examination of the entire peritoneal cavity can aid greatly in determining the need for laparotomy by evaluating the extent of the visceral damage. 3
If the injured portion is located in a mobile part of the small intestine, as in Case 3, laparoscopic-assisted complete exteriorization through a minimal umbilical incision followed by resection of the injured portion and end-to-end reanastomosis with manual suturing under direct vision may be another option that may achieve reliable outcomes. 5
However, in conventional multiport laparoscopic surgery, the small bowel cannot be exteriorized through 5–12 mm-ports without extending the incisions. This may be resolved thanks to recent advances in LESS surgery,5–8 wherein laparoscopic procedures are performed through a relatively long single incision measuring from 2 cm to 3 cm in length. As a result, umbilical incisions have been reported to allow the exteriorization of mobile tissue, such as the small bowel, 5 appendix, 6 and uterine adnexal tissue. 7
Although, LESS surgery is associated with surgical difficulties that need to be overcome, such as ergonomic constraints, 7 this approach enabled the current authors to reproduce safely all surgical steps usually performed during conventional laparoscopy or even laparotomy through intracorporeal as well as extracorporeal procedures.
Therefore, although further accumulation of cases is needed, LESS surgery for uterine perforation may become a useful surgical procedure in the era of minimally invasive surgery, offering advantages for patients without any specific complications, as demonstrated in these 3 cases.
Conclusions
Even in emergency cases experiencing iatrogenic uterine perforation, a minimally invasive approach with LESS surgery may be a feasible option for minimizing the abdominal scar, thereby reducing patient dissatisfaction regarding iatrogenic complications.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.