
Abstract
Background:
Early postoperative mechanical intestinal obstruction is rare, with the commonest cause being adhesions. The wide application of minimally invasive surgeries has increased the incidence of Richter's hernia.
Case:
A 63-year old, morbidly obese lady diagnosed with carcinoma of the uterine cervix underwent laparoscopic radical hysterectomy under general anesthesia. Two 10-mm ports were used—one in the umbilical area for a camera and the other in the right iliac fossa as a working port. Three 5-mm ports were also used. The procedure was completed without any intraoperative complications and a specimen was retrieved per her vagina. Postoperatively, this patient developed protracted bilious vomiting from day 2, which was managed conservatively for the first 8 days and was finally diagnosed to be Richter's hernia with contrast-enhanced computerized tomography (CECT). The patient was reexplored laparoscopically and managed successfully without any bowel ischemia or gangrene.
Results:
Following the second surgery, this patient recovered rapidly and was discharged to go home on a full diet by the fifth postoperative day.
Conclusions:
A strong clinical suspicion should alert the surgeon to consider CECT early in the postoperative course to diagnose and manage Richter's hernia.
Introduction
Intestinal obstruction in the early postoperative period is usually adynamic in nature, and dynamic or mechanical obstruction is rare. The commonest causes of early postoperative mechanical obstruction include adhesions. 1 The advent and wide application of minimally invasive procedures, such as laparoscopic and robotic methods, have introduced different kinds of complications, including bowel herniation leading to intestinal obstruction.2,3 Early port-site or trocar-site herniation—defined as bowel herniation through a port site ≥10 mm within the first week of surgery after laparoscopic radical hysterectomy—is uncommon. 4 It usually presents as Richter's hernia, which involves herniation of a part of the bowel circumference through the port site, leading to partial intestinal obstruction, wherein continuity of the intestinal tract is not compromised.5,6 This poses a diagnostic challenge to the clinician as the patient manifests without any classical signs and symptoms of total intestinal obstruction. A high index of suspicion is needed for early diagnosis, as early surgical intervention is needed, unlike the majority of other causes of early postoperative bowel obstruction, to prevent bowel gangrene and an untoward outcome. 5
Case
A 63-year-old woman, weighing 73 kg with a body mass index of 35.26 kg/m2, with no comorbidities, was diagnosed as having moderately differentiated squamous-cell carcinoma of the uterine cervix, at International Federation of Gynecology and Obstetrics stage1B, and underwent laparoscopic radical hysterectomy following appropriate clinical and radiologic evaluations under general anesthesia. The surgery was performed by a senior consultant with the assistance of 2 residents-in-training and 1 scrub nurse. Two 10-mm ports were used: 1 supraumbilical port for a camera and 1 right iliac-fossa working port. Three 5-mm ports were also used: 1 each in the right lumbar, left iliac fossa, and left lumbar areas (Fig. 1). The umbilical port was first placed by an open method, pneumoperitoneum was created, and other ports were used under camera visualization.

Port placements. Illustration used with permission by Vijayalakshmi Pusuluri, MBBS.
The surgery was uneventful, and specimen were delivered per her vagina, the vault was closed, hemostasis was ensured, a wash was given, and a pelvic drain was inserted. The 10-mm ports were then closed by the senior assistant with port-site closure Vicryl® 1-0 (Ethicon, Johnson & Johnson) after evacuating the CO2 gas, using Langenback retractors. Given that the patient was obese and had very thick abdominal fat, the closure was difficult and involved a great deal of retraction.
On the first postoperative day (POD), the patient's nasogastric (NG) aspirate was minimal and hence the NG tube that had been put in place was removed, and she was allowed to take sips of plain water; this was advanced to a liquid diet on POD 2. In the later part of the day, however, this patient had five episodes of bilious vomiting, which were treated by stopping her metronidazole and tramadol intravenous (IV) injections and an injection of ondansetron was started. On the third POD, the patient tolerated an oral liquid diet and passed flatus, but vomited twice. On the fourth POD, she did not have any vomiting episodes, continued to pass flatus, and tolerated a soft diet. On the fifth POD, her vomiting resumed and worsened to eight episodes with mild abdominal distension; hence, the NG tube was reinserted, oral feeds were stopped, and she was managed with IV fluids, antiemetics, and other supportive measures.
Also on POD 5, an erect radiograph of this patient's abdomen, serum chemistry levels including electrolytes, and ultrasonography of the abdomen were obtained, but were not informative. On POD 6, the vomiting had ceased, the NG aspirate was 450 mL, serum electrolytes were normal, and bowel sounds were sluggish. On seventh POD, the NG tube was temporarily blocked and oral liquids were allowed but she could not tolerate them. On PODs 8 and 9, the NG aspirate continued to be in excess of 1 L, there was still mild distension of the patient's abdomen, and her rectum was empty.
Suspecting a mechanical bowel obstruction, a contrast-enhanced computerized tomography (CECT) image of her abdomen was ordered POD 9. The CECT showed herniation of a partial circumference of the segment of bowel into the umbilical port site, with breakage of the stitching (Fig. 2). A diagnosis of Richter's hernia was made and immediate laparoscopic reexploration was decided upon. At surgery, the right iliac fossa 10-mm port was opened, a blunt trocar introduced, pneumoperitoneum was created, and a camera was introduced. There was a herniation of a part of the jejunal wall into the broken umbilical port site, with moderate dilatation of the proximal bowel (Fig. 3). The umbilical port was then opened, the incision was enlarged, and the herniated bowel was carefully reduced back into the peritoneal cavity. There was a 1 × 1–cm2 serosal tear and congestion with no frank ischemia. (Fig. 4).

Contrast-enhanced computerized tomography of the abdomen showing herniation of bowel through an umbilical port site (Arrow).
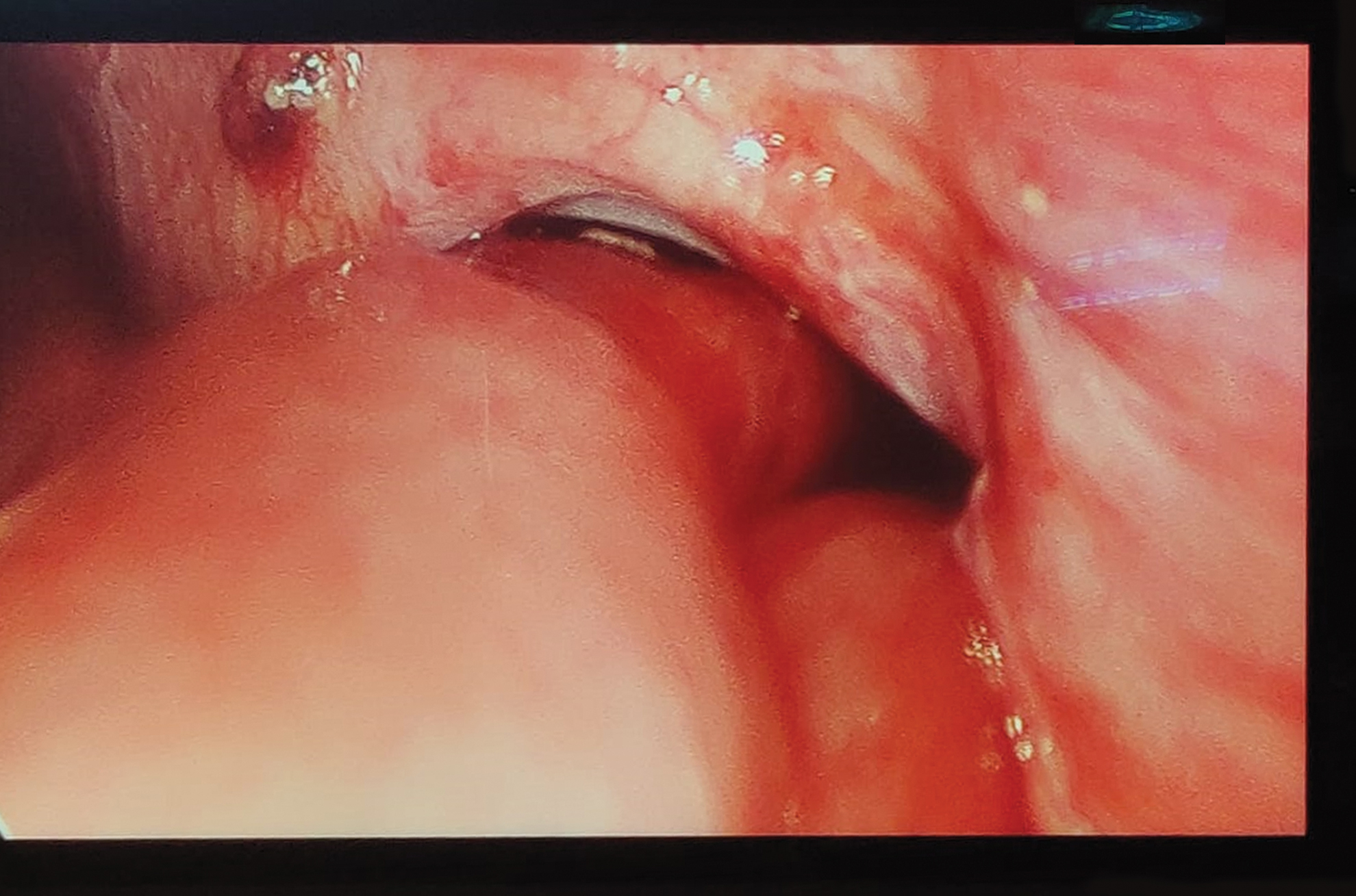
Intraoperative photograph showing herniation of the bowel. Color images are available online.
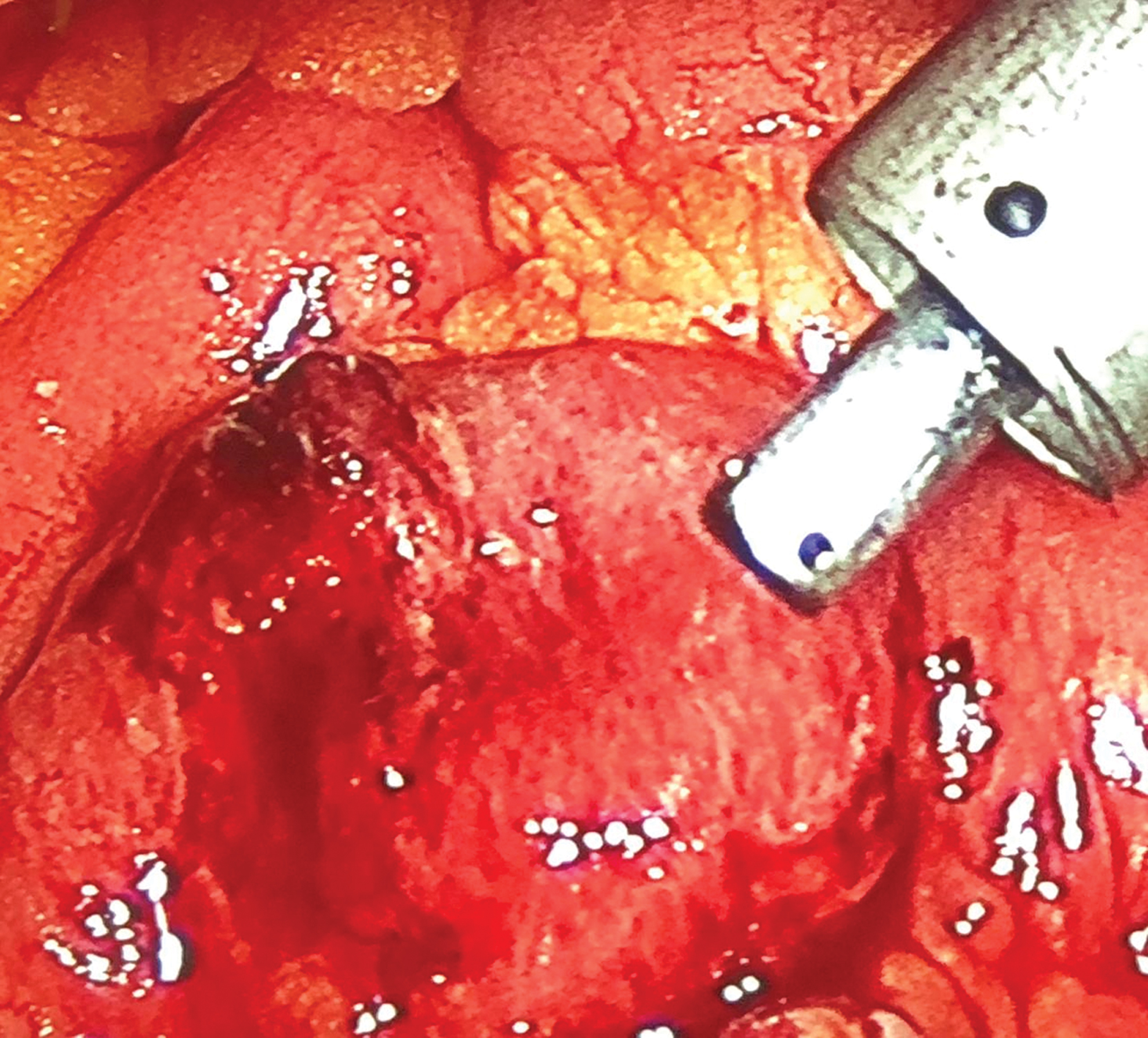
Serosal tear of the bowel at herniated site. Color images are available online.
The anesthetist was instructed to deliver 100% oxygen and warm saline gauze was placed over the congested bowel to ensure that the bowel was healthy and viable. Once the viability of bowel was confirmed serosal tear was repaired with intracorporeal 2-0 Vicryl sutures (Fig. 4). The abdominal drain was repositioned, the gas was evacuated, and the ports were closed by the senior consultant under careful visualization of the wound edges with Prolene® 1-0 (Ethicon) sutures.
Results
Following the reexploration, this patient made a remarkable recovery and was discharged home on the fifth POD on a full diet. Per the decision of the multidisciplinary tumor board of the hospital, she was referred for postoperative adjuvant radiotherapy, which she completed. She has remained disease-free at the time of this writing.
Discussion
Early trocar-site hernias are rare, are seen in <1% of all laparoscopic procedures, and are more common in gastrointestinal surgeries than in gynecologic procedures. The most-common locations of herniation are through umbilical and midline port sites, occurring within first the 10 days of surgery, due to a natural weakness of the linea alba. The most-common type is Richter's hernia, wherein a part of bowel circumference becomes herniated through a port site, leading to partial intestinal obstruction. The risk factors for the development of hernia include: obesity; advanced age; poor nutritional status; diabetes mellitus; use of steroids; large trocar size, technical factors such as multiple trocars and midline trocars; prolonged surgery; repeated insertion of trocars; stretching a trocar site; and incomplete closure and wound infection. 2
In obese patients, such as the current case, thick preperitoneal fat and increased intra-abdominal pressure favors herniation. 7 In this current case, the patients repeated episodes of vomiting in the initial few PODs might have caused the rectus sheath stitches to give way at the umbilical port-site, which could have contributed to the development of her Richter's hernia. Although it was not possible to speculate when the hernia developed, the patient's progressive deterioration by her eighth POD day was due to the development of this hernia. Although Richter's hernia is known to complicate rapidly into gangrene and bowel perforation, fortunately, this patient did not develop this complication. Clinical presentation of Richter's hernia is variable and difficult to differentiate from more-common wound hematomas or infections; thus a strong suspicion is warranted. 2
Port-site or trocar-site hernias could be early or late and are estimated to occur in nearly 2% of all laparoscopic surgeries. 5 Use of a large trocar (≥ 10 mm), improper closure of a fascial defect, a closed-method of port placement, midline ports more commonly at an umbilical site, stretching of a port for specimen retrieval, extension of an umbilical fascial defect, a wound infection, diabetes, obesity, and/or a compression effect of air are all predisposing factors for a port-site hernia.
Although trocar-site hernias were first described by Fear in 1968, 8 Tonouchi et al., in 2004. classified trocar-site hernias into three types, based on time of onset and defect 7 (1) early onset; (2) late onset; and (3) special types. In the early onset type, herniation occurs through a defect in the anterior or posterior fascial layers as well as in the peritoneum during the early postoperative time and often presents with small-bowel obstruction. The late-onset type presents several months postsurgery, and there is dehiscence in both the anterior and posterior fascial layers with the peritoneum forming the hernial sac. The special type involves a through and through defect in the abdominal wall including the skin. A high index of suspicion would lead a clinician to order a CECT, which can be used to diagnose this condition early.6,9 Most of these hernias can be managed laparoscopically, but sometimes open surgery might be needed.
In order to prevent such hernias, any trocar site larger than 5 mm in diameter should be closed at the fascial level meticulously, even if the skin wound needs to be enlarged. In children, defects of any size should be closed. In order to prevent the complication, a sound technique of port-site closure with clear visualization of the defect before closure is needed. Another technique is to use nonbladed cone-tipped trocars, which do not need closure in nonmidline sites above the arcuate line. One of the simple maneuvers is to deflate the abdomen before port removal by opening the valve to prevent herniation. Better fascial closure techniques incorporating a suture carrier, a closure device, a Deschamps needle, or port plugs can reduce the risk considerably. In the end, it is important to note that port-site hernias have increasingly been reported in 5-mm sites also7.10–12
Conclusions
Port-site hernias are rare, a high index of suspicion is needed, and early computerized tomography can confirm the diagnosis. Early surgery prevents bowel strangulation, and almost all patients can be managed successfully with laparoscopic reexploration.