
Abstract
Background:
An angiomyofibroblastoma (AMF) is a mesenchymal tumor that affects mostly reproductive-age woman; very rare cases have been reported in men. An AMF is generally an asymptomatic mass that primarily arises in the vulvar region. The tumor grows slowly but becomes quite large.
Case:
A 29-year-old nulliparous woman was diagnosed with having an AMF that was asymptomatic and huge. The AMF distorted both labia. This case was managed with a total vulvectomy and by addressing the serious skin defect caused by this surgery. A “double-barreled” colostomy was performed to protect this patient from any potential stool-induced infection. After these procedures, she received negative-pressure wound therapy (NPWT) dressings for 2 months, and reconstructive surgery with full-thickness skin grafts from both thighs was then performed. The colostomy was closed once the skin defect was closed.
Results:
The reconstructive surgery was successful with no adverse outcomes.
Conclusions:
It is important to confirm AMF histopathologically. When AMF is suspected for a vulvar lesion, complete excision of this tumor is the treatment of choice. NPWT is an appropriate way to facilitate wound healing. In a limited-resource country, NPWT can be useful for patient care.
Introduction
An angiomyofibroblastoma (AMF) is a generally asymptomatic mass that arises in the vulvar region. This tumor generally affects woman during reproductive age. Rarely AMFs have occurred in men. This article describes a woman's huge vulvar tumor that was confirmed to be an AMF.
Case
A 29-year-old nulliparous female presented with a 5-year history of progressive swelling of both labia with pockets of foul smelling discharge mixed with pus. Externally she appeared to have 1 mass of ∼3 × 10 × 3 cm of the right vulva and 1 mass of ∼5 × 12 × 9 cm of the left vulva. Both of these masses were rubbery firm, completely replacing both labia major (Fig. 1).

Angiomyfibroblastoma arising from both labia major.
This patient's history revealed that these masses initially started as 1 small hard nodule on the lower part of her right labia major about 6 years ago. The nodule was mild and painful, with a pus-like discharge that was mixed with blood. After an unnoticed time interval, she found another lesion growing from the lower part of her left labia major. Both lesions grew slowly as time passed. The masses became painless but caused an inability to walk freely due to the massive swelling of both labia.
Also included in this patient's history was a swollen lesion of both axillae 8 years ago. One lesion on the right axilla was itchy, mild, and painful, with a scanty pus-like discharge. Subsequently, multiple small lesions developed. After some time, these lesions coalesced into 1 large lesion, and the same pattern of development occurred on the left axilla within a short time. She had been treated at several health facilities, being given antibiotics and herbal medications. She was also treated twice for suspected extrapulmonary tuberculosis (TB), with 6 months and 8 months of anti-TB treatments, respectively, in 2007 and 2013. Axillar biopsies and pus cultures were performed but no report documented any results. However, no improvement occurred in her lesions.
There was no family history of hypertension, diabetes mellitus, or gynecologic cancer. Of her family's 9 children, this patient was the first-born child. She was not married and did not use alcohol or smoke cigarettes. She was not undergoing hormone-replacement therapy.
This patient's gynecologic history showed that she attained menarche at age 13, had 28-day regular cycles, with 5 days of menstrual flowing that was not painful. She had no history of contraceptive use, sexually transmitted diseases, or gynecologic procedures. She had no history of fever, cough, night sweating, or weight loss. Her gynecologic examination was normal, and there were no palpable inguinal lymph nodes. Her hematologic and biochemical parameters were also normal.
The initial suspected diagnosis was a vulvar malignancy, but this diagnosis was changed to a vulvar AMF after histologic results from a partial excision of the right vulvar mass (Fig. 2). The patient then underwent a total vulvectomy with partial closure (Fig. 3). She had a wet dressing applied every day. A “double barreled” colostomy was also performed due to the risk of wound contamination by the patient's stools. Afterward, she was started on negative-pressure wound therapy (NPWT) dressings, using an InfoVAC™ therapy system (KCI, 3M, St. Paul, MN, USA) for 2 months (Fig. 4). Vulvar reconstruction surgery with full-thickness skin flaps was performed, using skin from both posteromedial upper thighs (Fig. 5). Finally, closure of the double-barreled colostomy was performed.
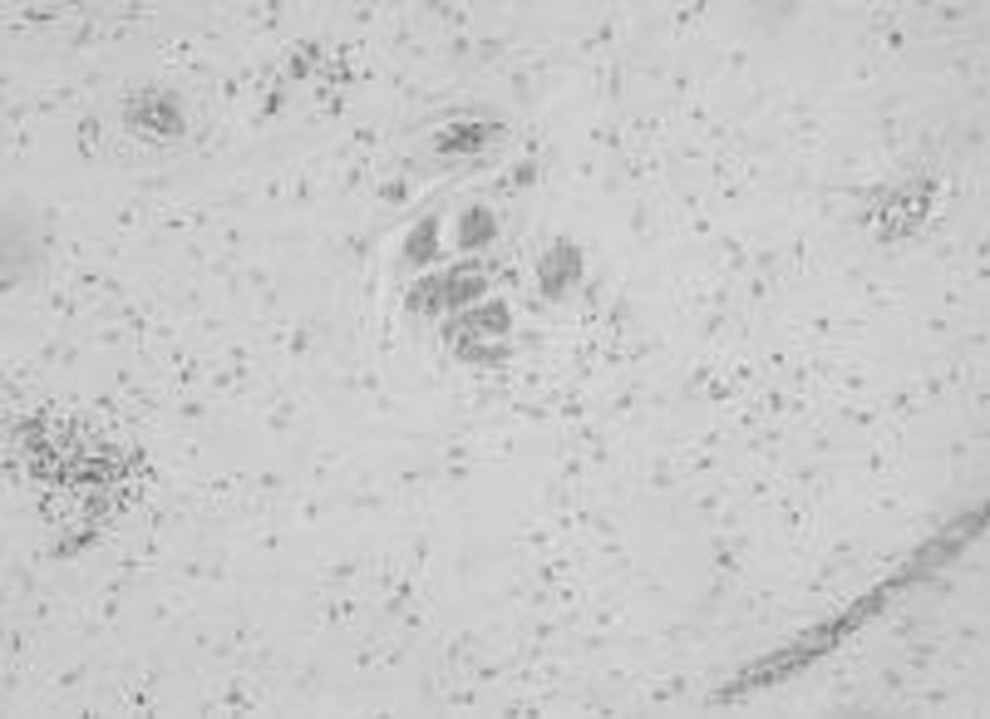
Histologic report: Tumor cells are spindled with low-level nuclear atypia and focally clustered with myoid cells (hematoxylin and eosin stain × 200).

Operation finding of total vulvectomy.
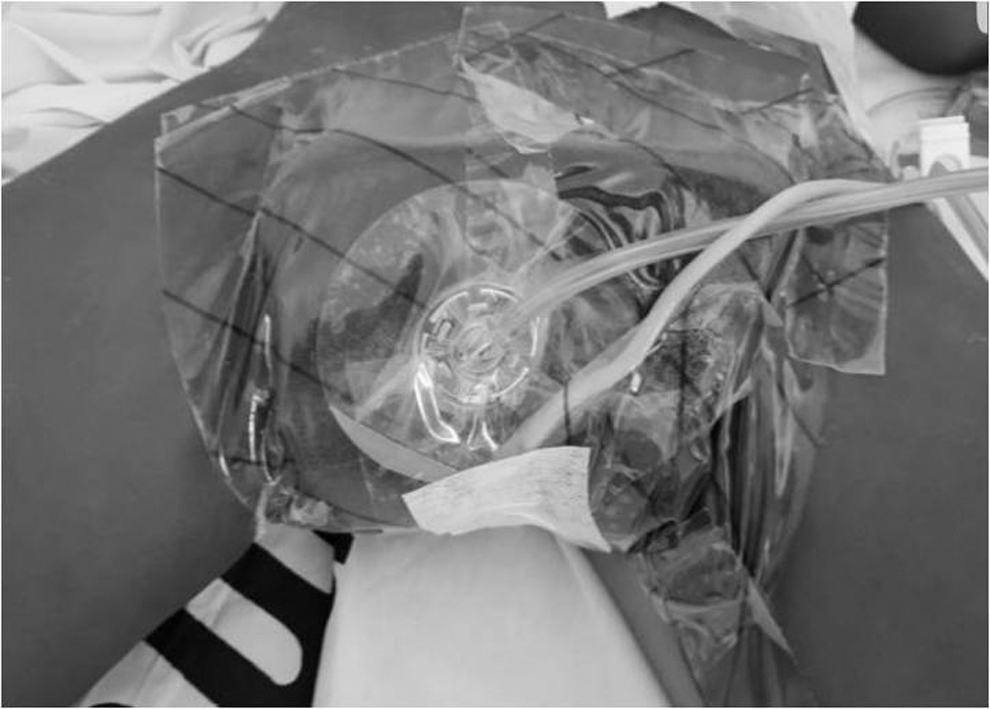
Negative-pressure wound therapy system applied.

Vulvar and perineal reconstruction with bilateral thigh flaps and skin graft.
Results
The reconstruction was successful.
Discussion
An AMF is a rare tumor. There are many differential diagnoses for AMF, including angiofibroma, angiomyolipoma, juvenile nasopharyngeal angiofibroma, solitary fibrous tumor, spindle-cell tumor, and angiomyxoma
The AMF was first described in 1992 by Fietcher et al. 1 Afterward, many cases were reported. These cases were found mainly in reproductive-age woman, with about 10% of patients being postmenopausal. Many of these AMFs were found on the vulva, and 10%–15% of these cases originated from the vagina. In men, paratesticular tumors were reported as homologous organ scrotums,2,3 inguinal hernias, and spermatic cords.4,5 A rare case of AMF was found at the orbit 6 and the mandible. 7
The diagnosis of AMF is made by based on several findings: superficial location; a well-margined tumor; spindled bland epithelial cells; numerous small- and medium-sized vessels with fibrinoid and hyalinized walls set in edematous collagenous stroma; low cell-mitotic activity; strong and diffuse vimentin activity; negative staining for actin and desmin; and mast cell and CD34–positive immunoreactivity staining. 8
AMF can be distinguished from an angiomyxoma by immunostain tests, such as that used for CD34. In the current case, hematoxylin and eosin staining was used only, due to very limited resources. Spindle-shaped–to-plump cells in loose stroma with prominent vascularity were noted (Fig. 2).
Surgical excision is the treatment of choice for AMF. These tumors grow slowly and rarely recur. Thus, complete excision is important. In the current case, after surgery to remove the tumor, the patient had a broad skin defect and the possibility of infection from her stools. A colostomy was performed. To facilitate wound healing, a wet dressing and then NPWT dressings were applied because of absence of an available reconstructive surgeon.
NPWT is a therapeutic technique using a vacuum dressing to promote healing in acute or chronic wounds and to enhance healing of second- and third-degree burns. NPWT promotes wound healing by applying a vacuum through a specially sealed dressing. The continuous vacuum draws fluid out from the wound and increases blood flow to the area. 9 The dressing is changed 2–3 times per week 10
A reconstructive operation with a full-thickness skin flap was performed by the plastic surgeon.
Conclusions
AMF has a better prognosis, if an early diagnosis and excision are performed before the tumor grows too large in any case.
Footnotes
Acknowledgements
Stephen Mihungo cared the patient everyday dressing.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this article.