
Abstract
Background:
Aggressive angiomyxoma is a benign, rare, and locally aggressive neoplasm that can be found in the perineal or pelvic region of female patients of the reproductive age group.
Case:
We present the first case report in Australia of a vaginal aggressive angiomyxoma in an obstetric patient during her 24th week of pregnancy.
Results:
The patient underwent surgical excision and close follow-up with no evidence of tumor recurrence in 2 years.
Conclusion:
Aggressive angiomyxoma is associated with a high rate of local recurrence and the recommended approach is preoperative imaging, surgery, and close follow-up. (J GYNECOL SURG 36:151)
Background
Aggressive angiomyxoma is a rare soft tissue tumor from myxoid cells, a cell type found in connective tissue. It usually presents as a painless lump, polypoid mass, or vaginal prolapse that may cause compression of the surrounding structures, leading to urinary frequency, urgency, or constipation. 1 It is termed aggressive due to the neoplastic nature of its blood vessels, local infiltrative behavior, and high risk of local recurrence. It is often misdiagnosed and confirmatory diagnosis is made after histologic examination. Macroscopically, it is characterized by its grossly gelatinous appearance and homogeneous consistency. 2 Microscopic characteristics include the presence of stellate or spindle cells with low mitotic activity, held together by a loose myxoid stroma, supplied by rich vascular network of thick-walled vessels and lacking a capsule. 3 Its differential diagnoses include a series of benign and malignant soft tissue tumors, including Gartner's duct cyst, vaginal prolapse, cystocoele, lipoma, or levator hernia. This tumor was first described in 1983 in a pathology journal. 4 To date, given the rarity of this tumor, there have been <350 case reports published internationally on aggressive angiomyxomas, but to our knowledge, none in Australia during pregnancy. 5
Case
Patient S was a 37-year-old primigravida who presented to the emergency department with a prolapsed mass arising from the anterior vaginal wall during the 24th week of her pregnancy. Her medical history included essential hypertension and her medications were methyldopa, aspirin, and a multivitamin. The vaginal mass was first noted during her 15th week of pregnancy. At that time, it was felt to be a 2-cm Gartner's duct cyst and was managed conservatively.
It was firm and gelatinous in texture, beefy-red, 9 cm, and held by a thick pedicle to the anterior vaginal wall. Careful examination confirmed a closed cervix and excluded protruding membranes through the cervix. The remainder of the genital examination was normal. Under a spinal anesthetic in theater, the mass was excised as closely to the anterior vaginal wall as possible and the stump was ligated with one Vicryl suture (Fig. 1). Histopathology confirmed an aggressive angiomyxoma (Figs. 2–4).

Macroscopic photograph of excised aggressive angiomyxoma. The received specimen was a polypoid piece of gray and tan skin, 92 × 63 × 40 mm.

Macroscopic photograph of polyp serially transverse sectioned. The cut surface of the polyp is solid, opaque, and gelatinous with areas of hemorrhage.
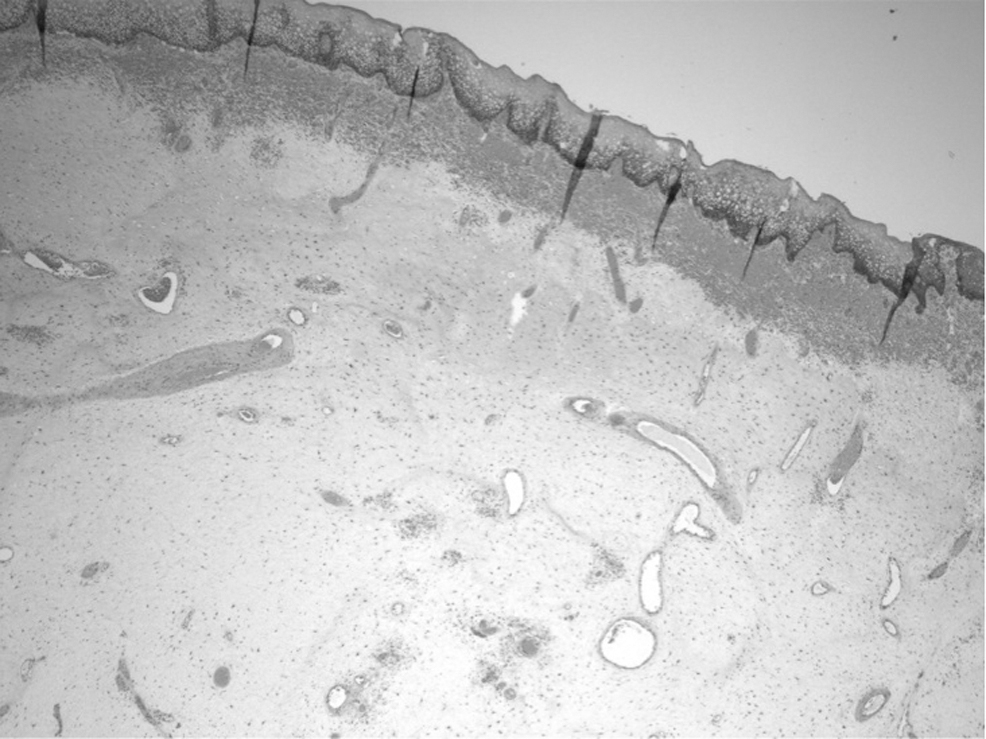
Microscopic photograph. Aggressive angiomyxoma characterized by a paucicellular to mildly cellular lesion composed of bland spindled to stellate mesenchymal cells embedded in a uniformly loose myxoid stroma. There is lack of necrosis and lack of mitotic activity. (H&E stain, 20 × magnification).

Microscopic photograph. Aggressive angiomyxoma showing prominent, often dilated, stromal vessels of varying caliber, and including thin-walled veins and thick-walled muscular arteries. (H&E stain, 40 × magnification).
The gynecology oncology multidisciplinary meeting recommended close clinical examination antenatal, and during the postpartum period. All vaginal examinations during the antenatal and postpartum period remained normal with no gross evidence of recurring disease. Patient S opted to have an elective cesarean section at 39 weeks due to concerns about local spread after possible vaginal trauma at birth. She had pelvic magnetic resonance imaging (MRI) at 3 months postpartum, followed by a positron emission tomography-computed tomography (PET-CT) scan and clinical review at 6 months postpartum, which were normal. Currently, Patient S is having annual gynecology follow-up and there has been no evidence of tumor recurrence to date.
Discussion
There are two types of angiomyxomas, superficial and aggressive. The etiology is not completely known but most likely arises from specialized stromal cells of the lower genital tract. 6 Generic aberrations have been described in pathogenesis of aggressive angiomxyomas, namely the high-mobility group AT-hook 2 (AMGA2) gene that is located on chromosome 12q15. 7 Most of these tumors are hormone sensitive and may express estrogen or progesterone receptors, causing them to grow bigger during pregnancy.
The mainstay of treatment is surgical excision. Complete excision of margins may be difficult due to the infiltrative margins of the tumor and the absence of a capsule. Recommended management will include preoperative radiologic assessment of simultaneous pelvic or perineal involvement (CT, MRI) and surgery to achieve tumor-free margins to reduce recurrence rate. 8 Higher recurrence rates have been described from incomplete excision, especially in cases where the lesions extend to the resection margins. 6 In a rare case, an aggressive angiomyxoma had been reported to infiltrate through bladder, bowel, and pelvic bone. 6 Some have been managed with hormonal treatment, such as gonadotropin-releasing hormone agonist and tamoxifen. Limited case reports have described some effectiveness of this treatment in shrinking the size of the tumor when surgery may not be an option. 9 Radiotherapy or chemotherapy is unlikely to be helpful as this type of tumor has low mitotic activity.
Follow-up is important given the risk of tissue regrowth and recurrence. Local recurrence has been reported up to 10–15 years after excision and in 30%–72% of cases. 6 Distant metastasis is extremely rare but reported in two cases, in distant metastasis to the lungs and mediastinum. 10
Conclusion
Preoperative diagnosis is difficult given its rarity and absence of diagnostic features, but should be considered in every woman presenting with a pelvic or perineal mass at a reproductive age. Suspected cases should undergo radiologic workup before excision and surgery should aim to achieve tumor-free margins. Given its tendency to recur locally, long-term follow-up is required. There is a paucity of data in the literature to guide optimal follow-up intervals and methods.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.