
Abstract
Background:
Ovarian transposition is recommended for preservation of ovarian function to prevent the sequelae of early menopause and to retain fertility. Potential postoperative risks of the procedure—including torsion, pain, bleeding, cyst formation, and malignant neoplasms—have been reported with low incidence. The aim of this report is to demonstrate the occurrence of an ovarian pathology in a patient who underwent ovarian transposition even after undergoing chemotherapy and radical surgery for cervical cancer.
Case:
A 44-year-old, gravida 3, para 2, woman presented with an ovarian cystic mass after neoadjuvant chemotherapy, radical hysterectomy with bilateral pelvic node dissection, and ovarian transposition for early stage cervical cancer.
Results:
The patient underwent a laparoscopic right cystectomy. The right ovary was enlarged to a 6-cm, multiloculated cystic mass with a thin capsule and mucinous fluid within it. The histopathology result confirmed that the mass was a mucinous cystadenoma. The patient has been free of disease for more than 10 years.
Conclusions:
Although ovarian transposition aids in preventing ovarian failure that can lead to symptoms of early menopause, there is still the possibility of an ovarian neoplasm arising in the remaining ovaries. Consistent follow-up is recommended to assess patients who undergo ovarian transposition. (J GYNECOL SURG 36:217)
Introduction
Ovarian transposition is a simple but underutilized fertility-preserving procedure that may be included in the comprehensive management of women with gynecologic malignancies who will receive pelvic radiation.1,2 Nearly half of patients with cervical cancer are in the premenopausal age group and are younger than age 45. Hence, preservation of ovarian function is a legitimate concern for this age group. The rationale of preserving the ovaries is to maintain ovarian function to prevent early menopause and to preserve the reproductive ability for future fertility. Ovarian failure leads to early menopause and its accompanying conditions, such as osteoporosis, cardiovascular disease, vasomotor symptoms, urogenital atrophy, and sexual dysfunction. Retaining the ovaries is performed to promote the possibility of oocyte retrieval followed by surrogate pregnancy.
Ovarian transposition should be presented in the treatment options for young patients who will undergo radiation in the pelvic area. Complications from the procedure are minimal. There are low risks of torsion, bleeding, pain, cyst formation, and malignant neoplasms as reported by several studies.
This article reports on a patient of reproductive age with cervical cancer who underwent ovarian transposition and chemoradiation. On a subsequent follow-up, an ovarian mass was detected, which was surgically managed.
Case
The patient was a 44-year-old, gravida, 3 para 2, female who was previously treated with neoadjuvant chemotherapy and radical hysterectomy and bilateral salpingectomy with bilateral pelvic lymph–node dissection and ovarian transposition for cervical adenocarcinoma stage at IB2 10 years prior to this current presentation. This patient was asymptomatic during the postoperative period, and there was no evidence of disease recurrence. Six months prior to this presentation, she began to experience right-sided, lower abdominal pain and felt a palpable mass. Ultrasound revealed a right ovarian cyst measuring 6.8 × 3.1 cm, and her cancer antigen (CA)–125 level was within normal range. An abdominopelvic computed tomography (CT) scan confirmed the benign nature of this right ovarian cystic mass further (Fig. 1A).
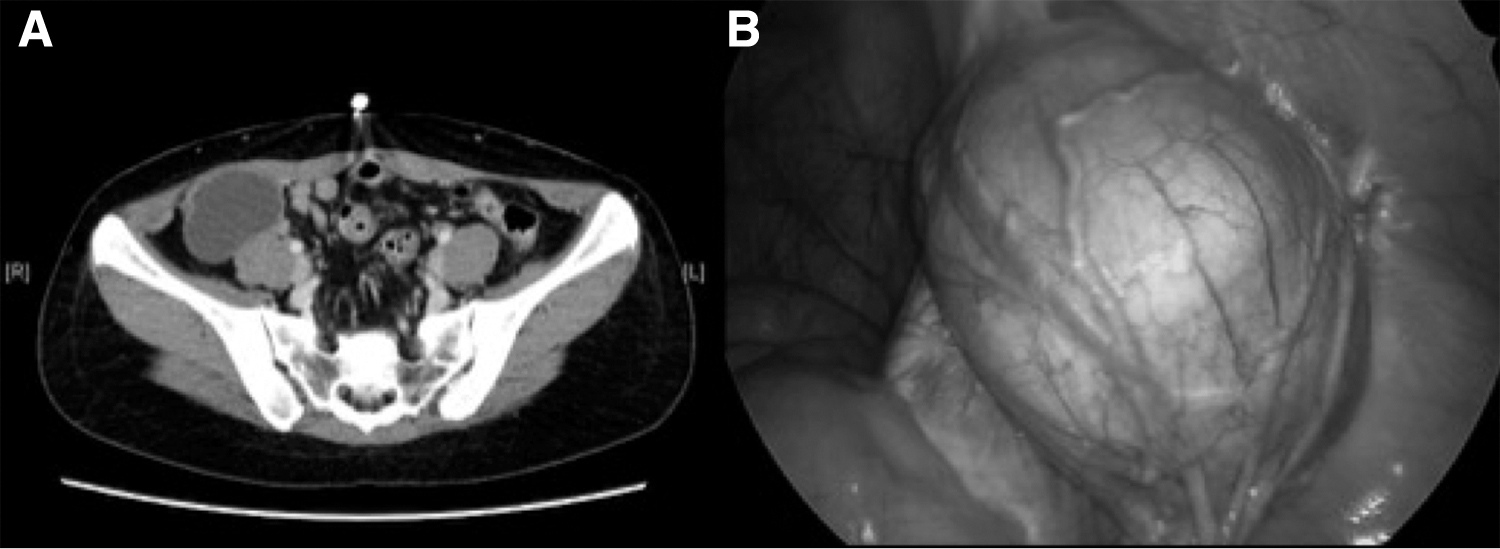
The patient was scheduled for laparoscopic surgery. Under general anesthesia, the operation was carried out using the Lee-Huang point and 3 lateral accessory ports. Intraoperatively, there were adhesions among the anterior abdominal wall, omentum, bowel, and left ovary. Adhesiolysis was performed. The right ovary was enlarged to ∼6 × 6 centimeters and was located at the right paracolic gutter (Fig. IB). A cystectomy was performed, and on cut section, the multiloculated cystic mass had a smooth, thin capsule with mucinous fluid within it. There were no papillary excrescences or solid areas. The left ovary was adherent to the surrounding bowels and omentum but appeared grossly normal. The procedure was completed with no intraoperative complications.
Written informed consent was obtained from the patient for publication of the case report and accompanying images. The institutional review board of the Chang Gung Memorial Hospital at Linkou Medical Center, Kwei-Shan, Tao-Yuan, Taiwan, ruled that approval was not required for this study.
Results
The patient had an uneventful postoperative course. She was discharged after 2 days in an improved condition. The histopathology result revealed that she had a mucinous cystadenoma. She has been having regular follow-ups with no recurrence of cyst formations or any pathologies.
Discussion
Ovarian transposition places the ovaries outside of the pelvis prior to pelvic radiation for gynecologic or nongynecologic malignancy. About 50% of patients diagnosed with cervical cancer are of premenopausal age, and recent trends have shown an increase in the age of first childbearing. In young patients, ovarian preservation is an important issue to prevent the sequelae of menopause, such as increased osteoporosis, cardiovascular disease, and urogenital atrophy. 3 Furthermore, ovarian preservation is essential in preserving their reproductive ability, which will enable future oocyte retrieval that can be used for surrogate pregnancy. 4
Radiation and chemotherapy are toxic to the ovaries. Low doses of radiation can cause permanent damage to the ovaries. There are also chemotherapeutic agents that reduce ovarian function. Hence, for patients with malignancy who need chemoradiotherapy, fertility-preservation treatment options—such as ovarian transposition, ovarian tissue cryopreservation, oocyte cryopreservation, and embryo cryopreservation—should be offered. 4 Ovarian preservation is highest in patients with cervical cancer who undergo surgery alone for their condition with a rate of 90%. For these patients who received pelvic external beam radiation therapy and/or brachytherapy, the ovarian-preservation rate is decreased to 65%. 1
There are risks and complications associated with ovarian transposition. Scattered radiation can still reach the transposed ovaries resulting in a loss of ovarian function.5,6 The ovaries must be placed as cranially and laterally as possible. However, overextension of the ovarian vessels may reduce blood supply to the ovaries, contributing to reduced ovarian function.5,7 Commonly reported complications are torsion, bleeding, pain, and growth of ovarian neoplasms that can be benign or malignant. Cyst formation has been reported to occur in 13%–17% of patients. 1 Although most patients might have received treatment that can cause irreversible damage to the ovaries and make the ovaries nonfunctional, there may be cyst formations or growths on the ovaries.
The current patient had already received chemotherapy for her malignant disease but an ovarian cyst still developed 10 years after treatment. In a case series including 104 patients with cervical cancer who underwent ovarian transposition, 22 were had benign ovarian cysts. 8 The majority of these cysts were managed with oral contraceptive pills with resolution of the cysts. The remaining 3 patients underwent surgical interventions, with findings of benign serous and mucinous cysts. Although the current patient presented with an ovarian mass, it turned out to be a benign entity and had no evidence of malignancy or metastasis. The presence of such ovarian masses is a potentially grave source of anxiety for these patients. It is imperative to investigate such masses, especially in patients with histories of malignancy to eliminate the possibility that the new growths might be recurrences or new malignant disease. In terms of malignant formation, there were only 2 reported patients with adenoid cystic carcinoma and cervical adenocarcinoma in patients with cervical cancer who underwent ovarian transposition. 9
In patients who undergo ovarian transposition, consistent follow-up is warranted in order to monitor hormonal status and possible menopausal symptoms, recurrence of primary cancer, and occurrence of other pathologies such as ovarian tumors. Migration of the transposed ovaries back to the pelvic cavity is also possible and is considered a failure of the ovarian transposition.6,10 Imaging studies may be done as deemed necessary based on the patient's presentation. Ultrasound was enough to detect and confirm the presence of an ovarian mass after the index patient experienced persistent abdominal pain. With the use of ovarian tumor markers and additional imaging testing, the benign nature of the mass was supported with the normal CA-125 level and benign features found on the CT scan.
The rationale behind ovarian preservation is to maintain ovarian function in premenopausal patients. The transposition is a simple and safe procedure that should be offered to young patients who wish to preserve their ovarian function and fertility. There is very little risk of metastasis to the transposed ovaries, and the occurrence of ovarian pathology is rare and usually presents as a benign condition.
Conclusions
Ovarian transposition is a safe procedure that provides young patients afflicted with malignancy to preserve their ovarian function to forestall early menopause and to allow future fertility plans such as oocyte retrieval and possible transfer for surrogacy. Although the risks and complications associated with ovarian transposition are low, the occurrence of ovarian growths should be addressed. Ovarian-cyst development is possible and is usually benign in nature.
Footnotes
Acknowledgments
The authors thank the Asia-Pacific Association for Gynecologic Endoscopy and Minimally Invasive Therapy (APAGE) for providing the International Fellowship in Minimally Invasive Gynecologic Surgery at Chang Gung Memorial Hospital for Dr. Mendoza.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
The authors of this report did not receive a specific grant for it from any funding agencies in the public, commercial, or nonprofit sectors.