
Abstract
Objective:
To determine the proportion of women with BRCA1/BRCA2 mutations participating in an ovarian cancer screening program who adhere to National Comprehensive Cancer Network (NCCN) guidelines for risk-reducing bilateral salpingo-oophorectomy (BRCA1 = 40 years, BRCA2 = 45 years).
Design:
Retrospective cohort study.
Materials and Methods:
Records were reviewed of all patients with BRCA1/BRCA2 mutations who were screened in Northwestern University's Ovarian Cancer Early Detection and Protection Program from 2002 to 2016. Exclusion criteria included a prior ovarian cancer diagnosis, oophorectomy before screening, or if visits were not recorded in the prospectively collected database. The primary endpoint was age at ovarian removal.
Results:
Of 134 patients identified (BRCA1, n = 83; BRCA2, n = 51), 46 patients underwent risk-reducing salpingo-oophorectomy (RRSO). Most surgeries (38/46, 83%) were performed by the upper limit of the mutation-specific recommended age. Of the 86 patients who have not undergone surgery, 49 patients are not yet at the recommended age for RRSO, 4 chose to continue screening, and 33 transferred care or were lost to follow-up. Patients were more likely to have prophylactic surgery by guideline-recommended age if they identified racially as white compared with non-white (odds ratio 7.5, 95% confidence interval 1.5–36.2, p = 0.02).
Conclusion:
More than 80% of BRCA patients in our program who obtained RRSO did so by the NCCN recommended ages. Indeed, most patients with BRCA1/BRCA2 who have not undergone surgery are still participating in the program. As more malignancy-related genes are discovered and evolving technologies developed for both genetic testing and cancer detection, screening programs may yet find a place in the management of high-risk patients.
Introduction
Ovarian cancer has an incidence of just 1.5%, but usually presents at advanced stage; as such, it has a higher mortality rate than all other gynecological cancers combined. For patients with BRCA1 or BRCA2 mutations, the lifetime risk of ovarian cancer increases to 17%–49% by age 70 years. 1 Although there have been multiple prospective screening trials, there are no proven methods for early detection of ovarian cancer. 2 Ultimately, governing bodies state that although routine screening is not recommended, high-risk patients such as those with BRCA1/BRCA2 may choose to undergo serial transvaginal ultrasound and CA-125 levels. 3
The gold standard for primary prevention and improving overall survival for patients at high ovarian cancer risk is to perform risk-reducing salpingo-oophorectomy (RRSO). For BRCA1/BRCA2 patients, this can decrease subsequent ovarian cancer risks and all cause mortality by 70%–80%.4,5 As such, both the National Comprehensive Cancer Network (NCCN) and the American College of Obstetrics and Gynecology recommend oophorectomy after the completion of childbearing at age 35–40 years for BRCA1, and age 40–45 years for BRCA2 carriers. 6 However, retrospective data from a single cancer center revealed that more than a third of BRCA1/BRCA2 patients who received genetic counseling do not obtain this risk-reducing surgery for various reasons. 7
There is established benefit for prophylactic surgery in women with known genetic risk for ovarian cancer, but an unknown benefit of screening in these patients. We thus sought to determine the rates of adherence to NCCN guidelines for RRSO in patients participating in a structured screening program, and describe factors associated with compliance.
Materials and Methods
Design
This is a retrospective cohort study of patients deemed at high risk for ovarian cancer who are screened in the Northwestern University Ovarian Cancer Early Detection and Prevention Program (NOCEDPP). Patients are referred to this program for various indications and meet with a genetic counselor at least once. Screening visits occur every 6 months up to age 35 years and every 3 months afterward until prophylactic surgery, and include a pelvic ultrasound, CA-125 blood draw, and physician consult. Additional imaging and referrals to gynecological oncologists were provided as necessary based on the screening results. Upon enrollment in the NOCEDPP, patients can provide informed consent for inclusion in a database and allow for review of their medical records for research purposes. Northwestern University Institutional Review Board approval was obtained at the initiation of the NOCEDPP.
Patients were included in this study if they were first seen in the NOCEDPP from 2002 to 2016, had a documented BRCA1 or BRCA2 mutation, provided informed consent, and had visits documented in the database and/or electronic medical record. They were excluded if their initial visit was after their mutation-specific NCCN-recommended age for RRSO (>40 years for BRCA1 or >45 years for BRCA2) or if they had a pre-existing ovarian cancer diagnosis or an oophorectomy before their first visit.
The database and electronic medical record were reviewed for clinicodemographic data, including age, racial identification, reason for initial gene testing, and dates of genetic testing, screening visits, and surgery. Surgical pathology was also reviewed if available.
Data analysis
The primary outcome was adherence to mutation-specific NCCN-recommended age guidelines for RRSO. Associations with clinicodemographic data were explored with univariate analysis. Demographics are reported as medians with interquartile ranges (IQRs) or proportions depending on the normality of the distribution. Odds ratios (ORs) with 95% confidence intervals (CIs) or Fisher's exact tests were calculated as appropriate, with p-value <0.05 considered significant. All statistical analyses were conducted using GraphPad Prism (version 7.00; GraphPad Software, La Jolla, CA, www.graphpad.com).
Results
There were 196 patients with a documented BRCA1/BRCA2 mutation seen in clinic through the NOCEDPP from 2002 to 2016 who consented for chart review (Fig. 1). After exclusion criteria were applied, there was a total of 134 patients included in the final analysis (BRCA1, n = 83; BRCA2, n = 51).
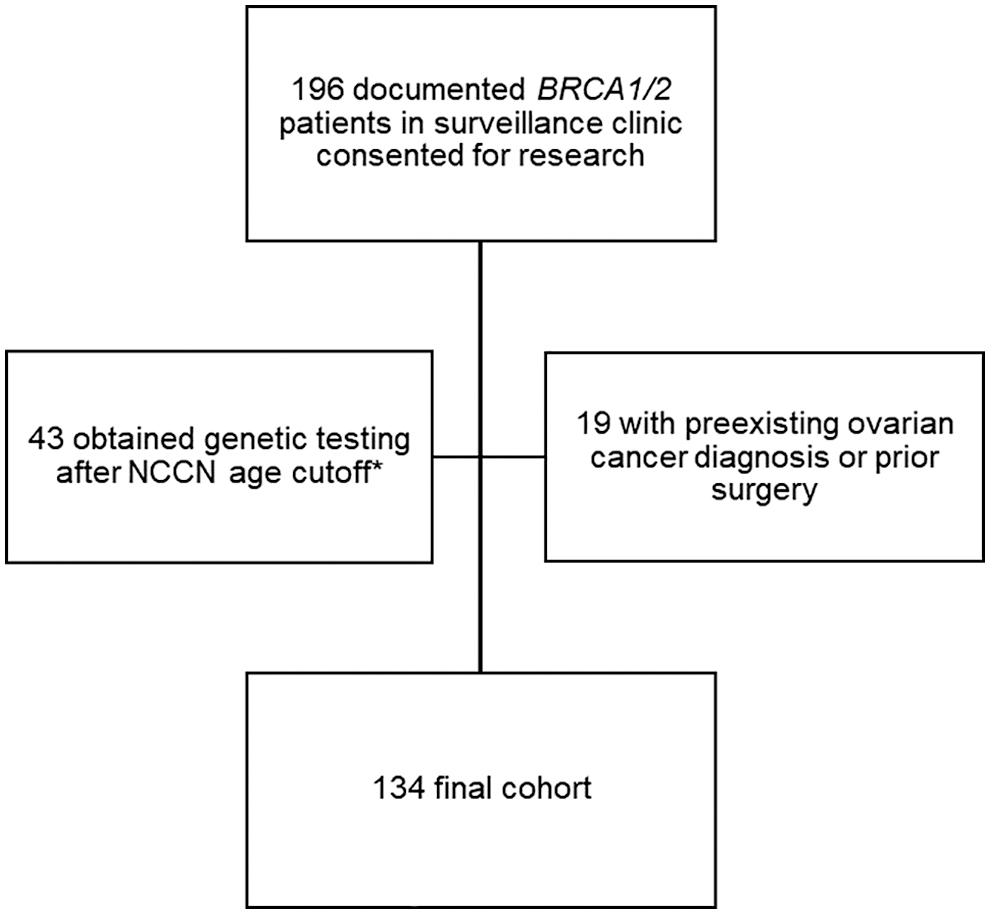
Patient selection criteria. A diagrammatic overview of inclusion and exclusion criteria. *Excluded cohort used for post hoc analysis. NCCN, National Comprehensive Cancer Network.
Most patients presented for genetic testing because of family history at a median age of 31.5 years; a majority were of Caucasian/white race and multiparous. Patients participated in the program for a median of 43 months and nine visits (Table 1).
Demographics of Participants with BRCA1/BRCA2 Screened in the Northwestern University Ovarian Cancer Early Detection and Prevention Program
IQR, interquartile range.
Of the 134 patients, 46 had RRSO surgeries and 2 had oophorectomies performed after a positive screening test (i.e., mass visualized on ultrasound or elevated CA-125); the latter 2 patients were not included in the risk-reducing surgery analysis. The median age at RRSO was 39.5 years (IQR 37–41; BRCA1 = 37 years IQR 36–40, BRCA2 = 40 years IQR 39–42) and 38 (83%) of the surgeries were performed by the upper limit of the NCCN-recommended age for their respective mutations (BRCA1 = 40 years, BRCA2 = 45 years). After obtaining genetic testing, patients waited a median of 51 months (IQR 10.8–110) before obtaining surgery (Table 2).
Information of Participants Who Obtained Risk-Reducing Surgery
Data are n (%) unless otherwise specified.
The eight patients who obtained surgery past the recommended age guidelines for RRSO were at a median age of 42.5 years (IQR 41–45.3), and all but one had BRCA1 mutations. For these patients, a median of 128 months (IQR 63–145) elapsed from their gene testing until their surgery and half of them chose to delay RRSO due to a desire for future childbearing.
There were 86 patients who have not yet undergone surgery as of the data cutoff date. Forty-nine (36.6%; BRCA1 = 31, BRCA2 = 18) are continuing screening before the NCCN-recommended age for RRSO, 4 (3.0%) (BRCA1 = 3, BRCA2 = 1) are continuing screening past the NCCN-recommended age for RRSO, and 33 (24.6%) (BRCA1 = 20, BRCA2 = 13) were lost to follow-up or transferred care.
The only factor significantly associated with an increased likelihood obtaining RRSO by guideline-recommended age was identifying as white compared with non-white (OR 7.5 95%, CI 1.5–36.2, p = 0.02; Table 3). There was a trend for patients with BRCA2 mutations to obtain their surgeries by the recommended age as compared with a BRCA1 mutation (94% vs. 75%, p = 0.12). Age at first visit or genetic testing, parity, time in program, or reason for testing (personal or family history of cancer) all were not associated with surgery timing. There were no occult malignancies discovered at the time of RRSO. One (4.3%) serous tubal intraepithelial carcinoma (STIC) was diagnosed in a BRCA1 patient who obtained her RRSO at age 43 years. There were no malignancies diagnosed on pathology, and both oophorectomies performed after a positive screen (2/134, 1.5%) were negative for malignancy.
Factors Affecting Likelihood of Obtaining Risk-Reducing Surgery by Recommended Age
As a comparison, we also examined data for the excluded 43 participants (Fig. 1, exclusion group; Supplementary Tables S1 and S2) who entered the screening program after the recommended age of RRSO (>40 years for BRCA1, >45 years for BRCA2). These patients were in a median age of 51 years (IQR 44–62.5) at genetic testing, with 51% pursuing testing because of a personal history of breast cancer. Seventy-two percentage of the patients (n = 31) obtained their RRSO after a median of 5 months from gene testing (IQR 3–11.5 months) at a median age of 53 years (46.5–59.5), with two STIC lesions diagnosed. There were also three surgeries leading from a positive screen, including one malignancy (stage 2B papillary adenocarcinoma arising from the fallopian tube).
Discussion
For patients with BRCA1 and BRCA2 mutations who entered a structured ovarian cancer screening program before the NCCN-recommended age for risk-reducing surgery, 82.6% (38/46) of those who obtained prophylactic surgery did so by the mutation-specific age. Of patients who had not yet had surgery, 57% (49/86) continued screening before reaching that age. Overall compliance with screening guidelines was thus 65.9% (87/134). Nine percent (n = 12) of patients delayed surgery or continued screening after the recommended age and 24.6% (33/134) were lost to follow-up. The only factor associated with having RRSO by the guideline recommended age was white race.
The rates of RRSO uptake in this study are higher than the published literature on BRCA1/BRCA2 patients, which have reported a rate of RRSO between 40% and 70%.7–13 Reasons behind previously reported lower uptake may be due to a shorter follow-up time in these studies, and changes in medical practice over the years to increasing acceptance and adoption of risk-reducing surgery. Some of these studies were also conducted as retrospective population reviews, whereas our patients have regular counseling by trained genetics providers who keep patients up-to-date on current guidelines and remind them of the benefit of prophylactic surgery. This portends a possible benefit of screening programs perhaps not for early detection, but in engaging high-risk patients into appropriate care.
On average, patients obtained their surgeries after 43 months (3.5 years) in the program, which is a shorter interval compared with research suggesting that most women diagnosed with BRCA1/BRCA2 had risk-reducing surgeries (both mastectomy and oophorectomy) within 5.3 years. 7 Previous publications associate the likelihood of RRSO with increasing age,7–9,11,12 higher parity,9,13 higher socioeconomic status, 11 personal history of breast cancer,7–9 and identifying racially as white.9–11 Interestingly, the only significantly associated factor with obtaining RRSO by the recommended age in our group of BRCA1/BRCA2 patients was identifying as white.
This racial disparity in prophylactic surgery has been described to be particularly striking for black Americans 10 despite high BRCA1/BRCA2 pathogenic variant prevalence in individuals of African descent. 14 The reasons behind the disparity are multifaceted, and suggested to be related to cultural, geographic, and psychological factors. In one study of black, Hispanic, and non-Hispanic white BRCA patients, the strongest link to a patient obtaining treatment is having a provider discuss their genetic results. 10 In the NOCEDPP, all patients obtain genetic testing and meet with a provider at each visit, so lack of genetic counseling should not be the reason for non-white participants being less likely to obtain RRSO by the recommended age. However, we cannot comment on the content of patient–provider interactions, and whether there were discrepancies in the actual surgical recommendations.
The lack of other associations such as age and parity may be due to the upper age restriction we placed on the cohort. Post hoc analysis of the older excluded participants who entered the screening program after the recommended age for RRSO revealed a shorter interval to surgery, higher parity, and a greater number with a personal history of breast cancer. Thus, the associations noted from prior studies with likelihood of RRSO were possibly mediated by inclusion of patients of all ages, and our results are uniquely representative of a younger population of BRCA carriers.
Practice implications and research recommendations
Although few concerning findings requiring surgery were detected in this cohort, the benefit of the NOCEDPP lies in the improvement in adherence with NCCN guidelines for RRSO compared with other published experience. As access to genetic testing improves and guidelines evolve to include additional moderate-risk genes such as BRIP1 or RAD51C/D, our finding may become more important. 3 Moreover, older patients may still benefit from participating in a screening program despite not meeting the recommended surgical age cutoff, as evidenced by the short interval between genetic testing and RRSO for the cohort who entered the program after the recommended age for prophylactic surgery. Indeed, of the 31 older patients, 1 was diagnosed with a stage 2 malignancy and 2 were diagnosed with STIC lesions (6.5%), which is a higher rate than 1%–2% reported STIC identification during RRSO.15,16 Arguably, the one malignancy that may have been prevented with earlier participation in a screening program.
In addition, studies need to be conducted to determine whether the improved adherence with guidelines and engagement in the screening program are due to the ovarian cancer screening program, or simply due to the regimented and close follow-up. Furthermore, research is required to determine actionable methods to address the racial disparities behind both screening itself and receipt of risk-reducing surgery, as we found racial disparities in surgery rates even among patients already undergoing screening.
Strengths and limitations
The main strength of this study is the data source of a large database of information collected prospectively over a period of 15 years with longitudinal follow-up. The sample size is comparable with previously published single-cohort observational studies of BRCA1/BRCA2 patients.7–11 We also present data specifically for patients before an age of actionable risk-reducing surgery, which is a cohort that has not been previously described in the literature and may have unique benefit from early detection and screening programs.
The major limitation of the study is the small number of patients who identify as non-white, echoing the dearth of racial diversity in similar studies in the literature and reflecting a reality wherein minority patients undergo both genetic testing and counseling less often than their white counterparts.9,10,17 A second limitation is the generalizability of this cohort who may intrinsically be more engaged in medicine, and the practice setting that includes easy access to genetic testing, counseling, and regular follow-up. With the current state of ovarian cancer screening, most studies on the behaviors of BRCA1/BRCA2 patients are abstracted from genetic or cancer research centers.7–9,13,18 Research in real-world settings outside of these specialized centers is of great interest. Third, we were unable to determine the compliance outcomes for 25% of patients because they were lost to follow-up or transferred care.
Conclusion
Despite the uncertain benefit for ovarian cancer screening on mortality, 6 we show that screening programs may be instead useful for engaging patients with actionable genetic mutations such as BRCA1/BRCA2 and ensuring that they obtain the recommended prophylactic treatments. As surgical prophylaxis guidelines evolve for additional malignancy-related genes, screening programs may yet find a place in the management of high-risk patients.
Footnotes
Acknowledgment
The authors thank Kisha Hope, the Clinical Research Coordinator and the Database Administrator of the research arm of the Northwestern University Ovarian Cancer Early Detection and Prevention Program, for helping accrue data.
Author Disclosure Statement
Authors X.M.G., M.C., A.P., L.S., and E.L.B. report no conflict of interest.
Funding Information
This study was supported by Bears Care, a charitable beneficiary of the Chicago Bears.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.