
Abstract
Objective:
The aim of this study was to explore the effects and applications of a robotic minimally invasive bowel-segmental resection, following intracorporeal anastomosis for treatment of deep infiltrating endometriosis (DIE). The procedure reconciled a totally intracorporeal anastomosis (TIA) procedure and robotic natural-orifice specimen extraction (R-NOSE) associated with Firefly™ fluorescence (F) technology (Intuitive Surgical Inc., Sunnyvale, CA) for optimizing outcomes in colon and rectal resection. The authors' initial group experience is also mentioned.
Materials and Methods:
Fifty-six patients with DIE of the colon and rectum underwent the surgical procedure in a tertiary-care referral institution for endometriosis. A standardized robotic procedure was performed with bowel resection and indocyanine green–induced F used for bowel-perfusion assessment. Specimen withdrawal was performed through natural orifices. Patients underwent the surgical procedures from December 2015 to October 2019. Surgical outcomes data and patient follow-ups are reported.
Results:
All patients had robotic minimally invasive bowel segmental resection, following intracorporeal anastomosis. The group's mean age was 36.8 (range: 28–46 years); with a mean body mass index of 22.88 kg/m2 (range: 18.9–28.3 kg/m2). In all cases, end-to-end position anastomoses were performed, using a circular stapler; no conversion or diverting stoma were needed. All patients had indocyanine F imaging assessment for bowel and anastomosis perfusion. Mean hospitalization was 4.5 days (range: 3–6 days), and no mortality occurred. No anastomotic leakage or rectovaginal fistula were observed.
Conclusions:
R-NOSE with TIA including Firefly F is a safe and feasible minimally invasive approach to benign bowel disease, reconciling prevalent procedures for endometriosis and colorectal surgical treatment. (J GYNECOL SURG 36:128)
Introduction
Endometriosis affects 10
Currently, a minimally invasive approach, laparoscopic or robotic-assisted surgery, remains the “gold standard” for radical treatment of DIE of the rectum and sigmoid colon (DIERS). 4 The surgical approach could involve a conservative procedure, mainly based on shaving, discoid excision, or a radical procedure (i.e., colorectal segmental resection). In colorectal resection for other benign conditions, such as diverticular disease, the minimally invasive approach is considered to be a safe and effective option. The use of fluorescence (F) angiography for bowel-perfusion assessment with indocyanine green for left-side resections could also contribute to a well-vascularized colorectal anastomosis. 5
Classically, to retrieve a specimen retrieved with a laparoscopic technique involves performing a Pfannenstiel incision or enlarging the trocar site. These procedures can cause complications, such as wound-site infections, incisional hernias, or abdominal pain. 6 Thus, an alternative procedure based on natural-orifice specimen extraction (NOSE), such as the vagina or anus (transrectal, transanal, transcolonic extractions), has been proposed in the literature as a way of enabling reduction of surgical traumata without compromising efficiency.
The NOSE procedure was first described in 1996 by Redwine et al., 7 who used an assisted transvaginal approach to extracorporeal anastomosis. Similar techniques were reported by Abrao et al. 8 and Ghezzi et al. 9 ; therefore, reinforcing their feasibility and low morbidity. So far, rectovaginal-fistula development and longer dissection of the mesocolon remain the major procedures.
The purpose of this article is to describe a robotic NOSE (R-NOSE) and intracorporeal anastomosis technique (TIA) associated with Fireflytm F (Intuitive Surgical Inc., Sunnyvale, CA) imaging for treatment of colorectal benign diseases, which is demonstrated in DIERS better. In addition, this article reports brief results and postoperative outcomes from a previous case series of patients who underwent the procedure.
Materials and Methods
This study was approved by the Ethics and Research Committees (Comitê de Ética e Pesquisa) concerning its requirements and orientations; and this publication was endorsed by the institutional review board. All procedures were performed in accordance with its regulations at the Sociedade Beneficente Brasileira Hospital Israelita Albert Einstein, in São Paulo, SP, Brazil, where the study was performed.
The procedure involved using a 4-arm standard Da Vinci® Si or XI surgical system (Da Vinci Surgical System; Intuitive Surgical, Inc., Sunnyvale, CA) including Firefly™ F imaging (Intuitive Surgical Inc.). Patients underwent a mechanical bowel preparation 1 day before the surgical procedure using mannitol or a rectal fleet enema, if necessary. Intravenous antibiotic prophylaxis was administered using ceftriaxone before the skin incisions and general anesthesia. Each patient was placed on a 21° Trendelenburg lithotomy position, after a bladder catheter was placed to control urine output while a uterine manipulator was placed through the cervix. The peritoneal cavity was accessed in the umbilical site with a Veress needle, a pneumoperitoneum was established with a pressure of 20 mmHg for camera-trocar insertion, and pressure was reduced to 15 mm Hg for placement of the remaining ports. The sections below describe the technique in detail.
Step 1. Surgical room set up with robotic docking and port placement
Low inferior left-quadrant docking was used for the Si platform with a port placement including a 12-mm 30°-umbilical robotic laparoscope, a 12-mm port placed in the right flank with two 8-mm trocars and one 5-mm trocar, which were arranged in a W shape (Fig. 1). For the Da Vinci Xi platform, standard docking and pelvic targeting were performed with subsequent 8-mm trocars positioned as previously mentioned. The 4-arms docking was associated to a port-in-port technique.
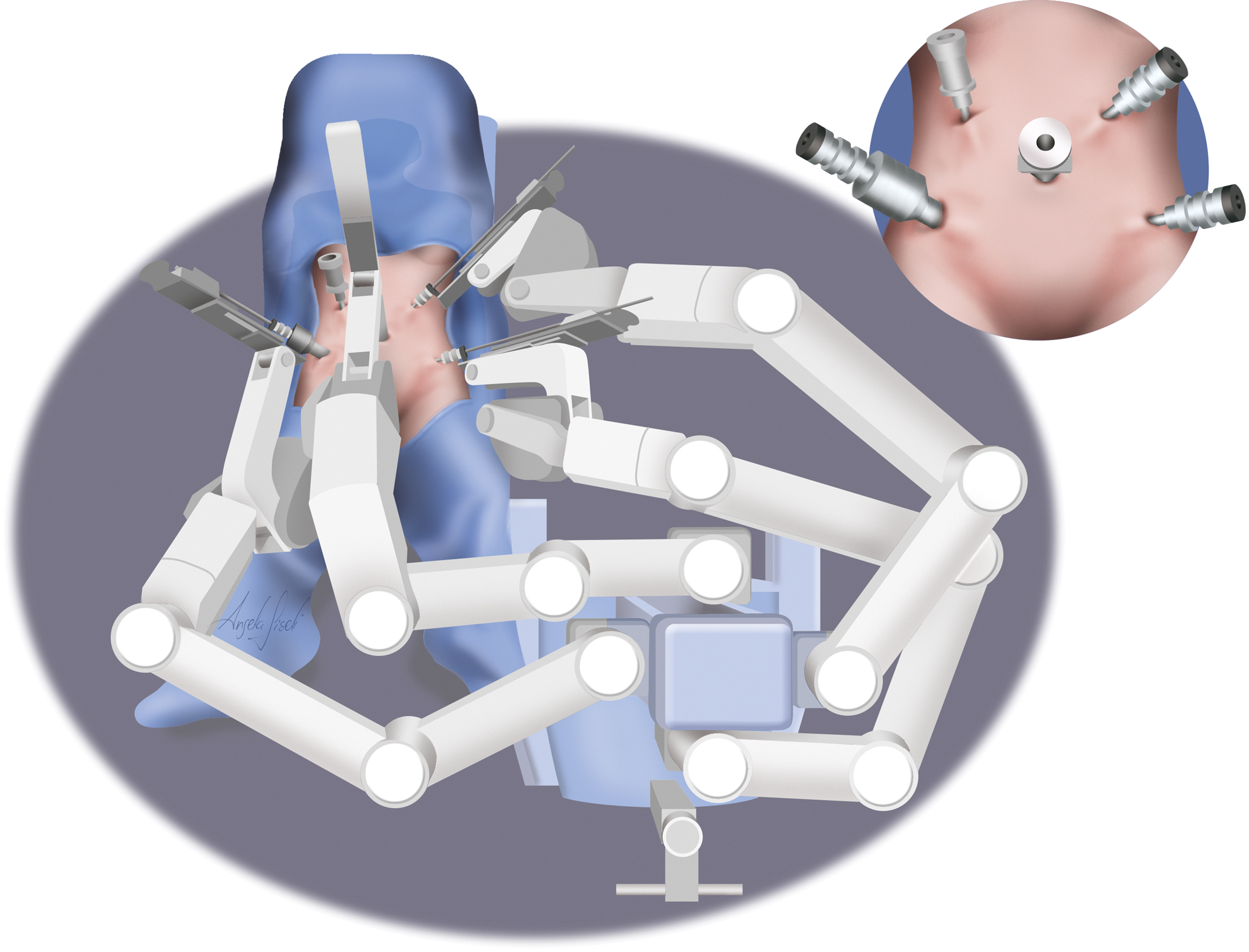
Standard 4-arm Da Vinci® (Intuitive Surgical Inc., Sunnyvale, CA) robot docking and trocars placement position enhancing the port-in-port technique in No. 1 arm. Color images are available online.
Step 2. Cavity diagnosis and staging
After pneumoperitoneum induction, trocars and the robotic 30°-camera insertion, the abdominal cavity was inspected, followed by a careful evaluation of the disease.
Step 3. Brief mesocolon dissection and mobilization
Once the intestinal segment to be resected was mapped, ligation of the mesocolon was performed as closely as possible to the intestinal wall. Identifying inferior mesenteric vessels; and safeguarding the left ureter, gonadal vessels, and autonomic hypogastric nerves, were crucial for avoiding undesirable complications. The ovaries were fixed to the anterior abdominal wall, using a No. 4-0 Prolene® double-armed suture with a linear needle (Ethicon, Somerville, NJ). Mesocolon mobilization was performed by incising Toldt's fascia; not requiring a large dissection, whereas an intracorporeal anastomosis was intended.
Step 4. Bowel delimitation
After sealing the mesenteric vessels with the harmonic device (Da Vinci Harmonic® ACE®; Intuitive Surgical Inc.), distal and proximal margins of resection were prepared using Firefly F imaging (Figs. 2 and 3). A total of 25 mg of indocyanine green was diluted in 10 mL of sterile water, and 4 mL of its solution was infused intravenously followed by 10 mL of a saline push. The green pigment provided additional information about bowel perfusion, and promoted a well-vascularized remnant colon to enable a secure colorectal anastomosis. Once both proximal and distal margins were defined, they were sectioned using the harmonic device (Da Vinci Harmonic ACE), leading to a tissue retraction and minimizing cavity gross contamination (Fig. 4). When opting for transvaginal extraction, bowel distal margin may be stapled rather than just sectioned, and this can lead to an already prepared rectal stump.

Bowel segment after mesocolon vessels' sealing in a conventional visualization. Color images are available online.

Bowel segment vascularization enhanced when using Firefly™ fluorescence (Intuitive Surgical Inc., Sunnyvale, CA) imaging technology. Color images are available online.
After Firefly™ (Intuitive Surgical Inc., Sunnyvale, CA) delimitation, segmental bowel is sectioned using Da Vinci Harmonic™ ACE (Intuitive Surgical Inc., Sunnyvale, CA) on its distal and proximal margin. Color images are available online.
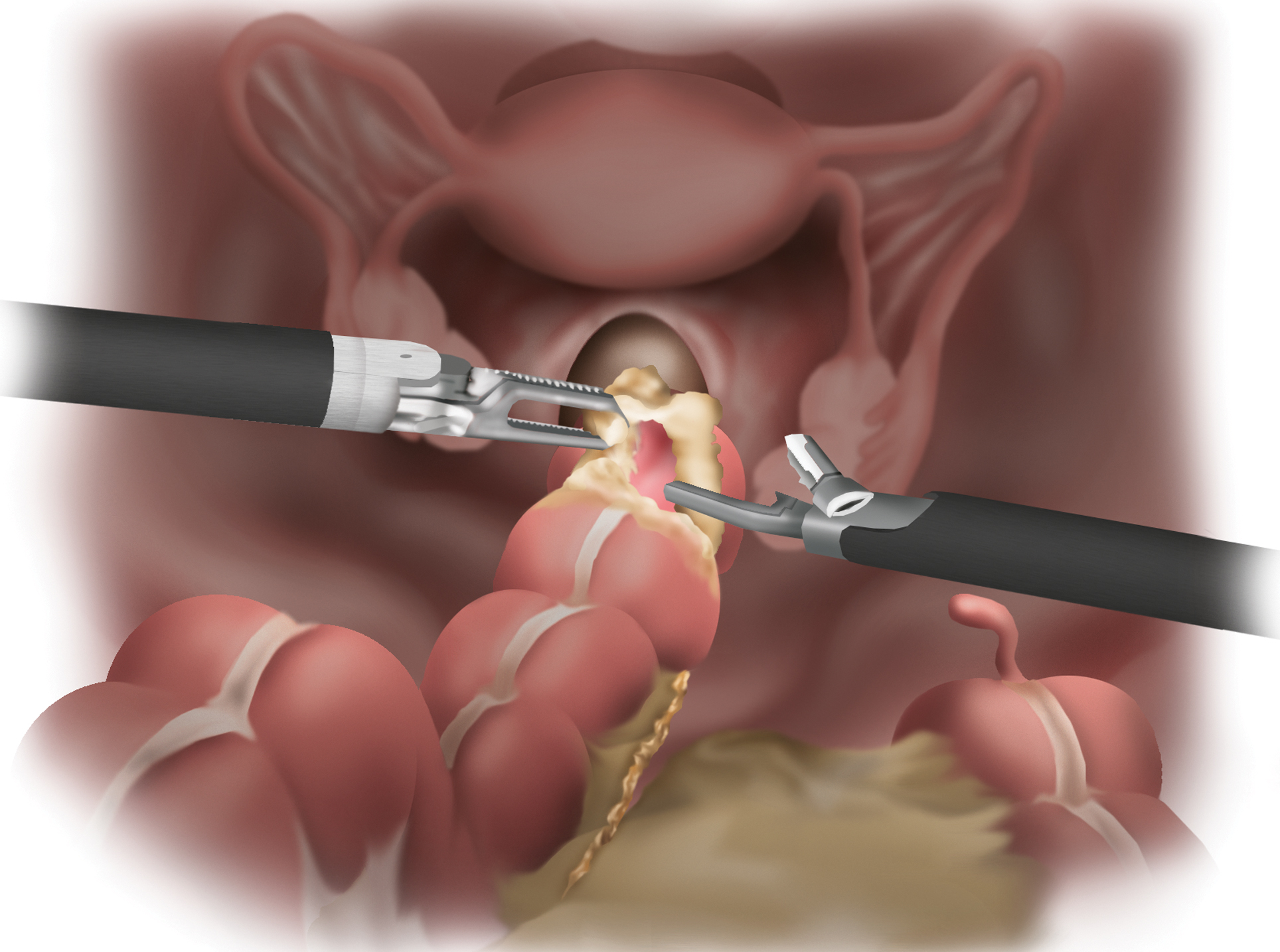
Step 5. Specimen extraction
Specimen withdrawal was accomplished by way of transrectal (Fig. 5) or transvaginal access (Figs. 6 and 7) depending upon the type of resection and in cases when colpotomy was needed. If a colonic or rectal resection was mandatory because of endometriosis impairment, a transrectal extraction with vaginally preservation was preferred. A sponge forceps was introduced through the orifice site by the surgeon assistant to extract the specimen in a careful low-traction maneuver, avoiding tissue laceration.

Transrectal extraction is performed after complete bowel section using a sponge forceps. Color images are available online.

When opting for a transvaginal extraction, a colpotomy is performed. Color images are available online.
Transvaginal withdrawal can also be performed by careful traction of the specimen with a sponge forceps through the colpotomy orifice. Color images are available online.
Step 6. Intracorporeal anastomosis and orifice closure
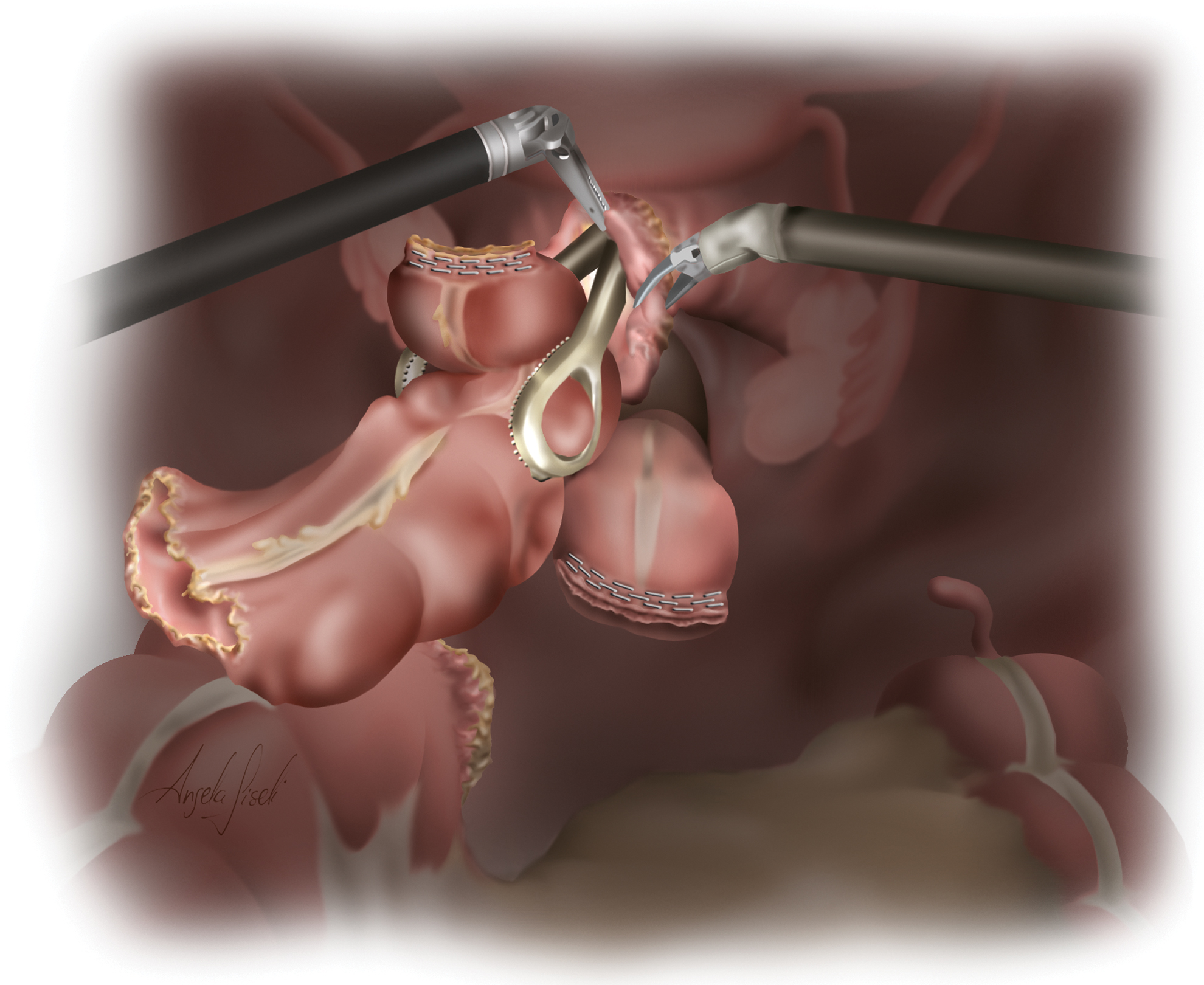
For an intracorporeal anastomosis, the anvil was introduced retrograde through the anal or vaginal opened orifice, attached to a linear Kelly forceps, passed by a distal margin that was sectioned and placed in the abdominal cavity. By pulling the opened distal colon with remaining robotic instruments, single linear stapling was performed to close the rectal part when confronted with a long and outward residual rectal stump. In some cases, when the remnant rectal part was too short and inward toward the pelvis, 3 border stitches were made for traction followed by an inversion of the robotic arms command; facilitating the linear stapling. The current authors recommended firing twice with linear staples when confronted with a very-low remnant rectal stump in order to achieve a more-hermetic and transversal staple line when performing the subsequent circular stapling.
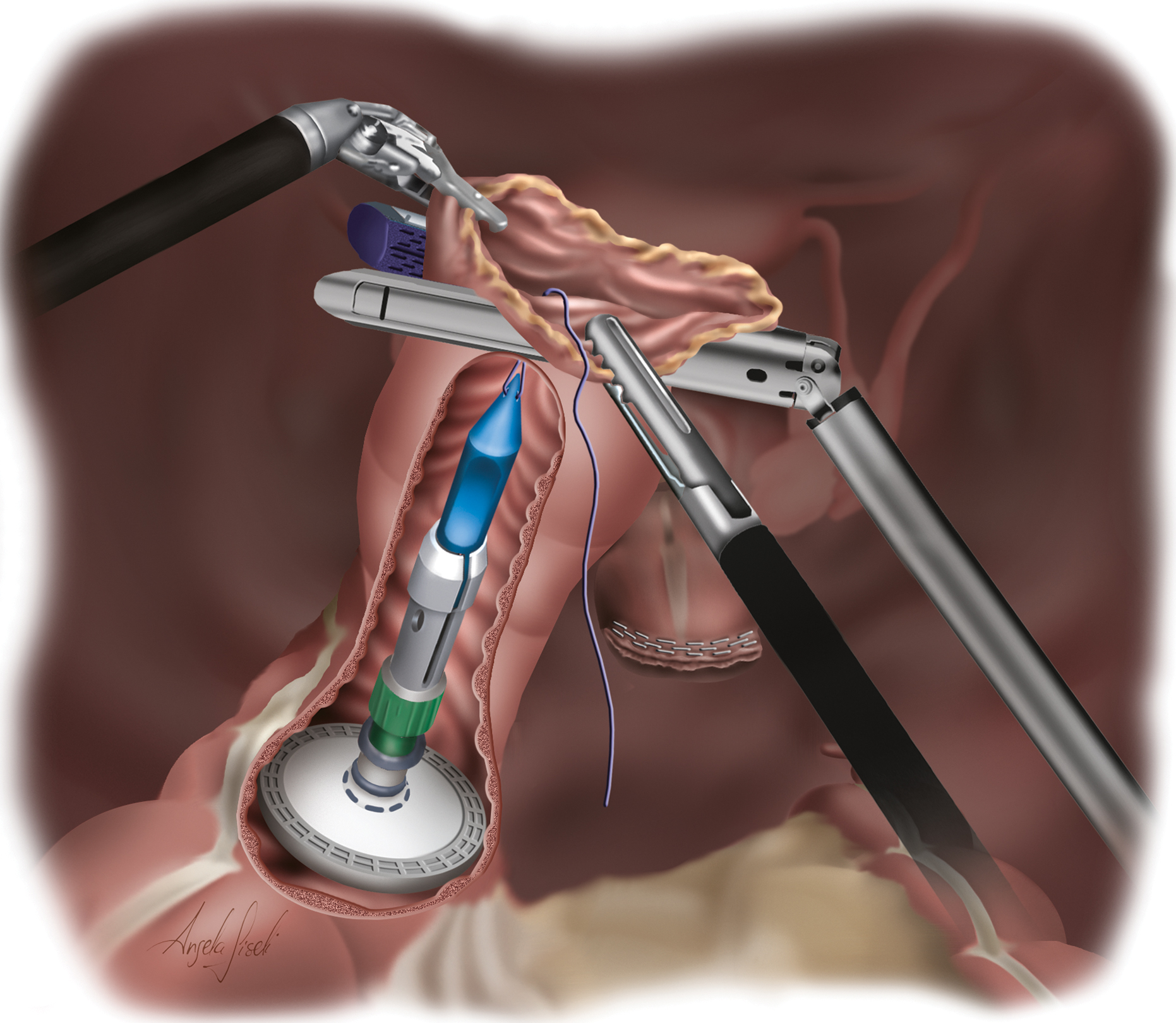
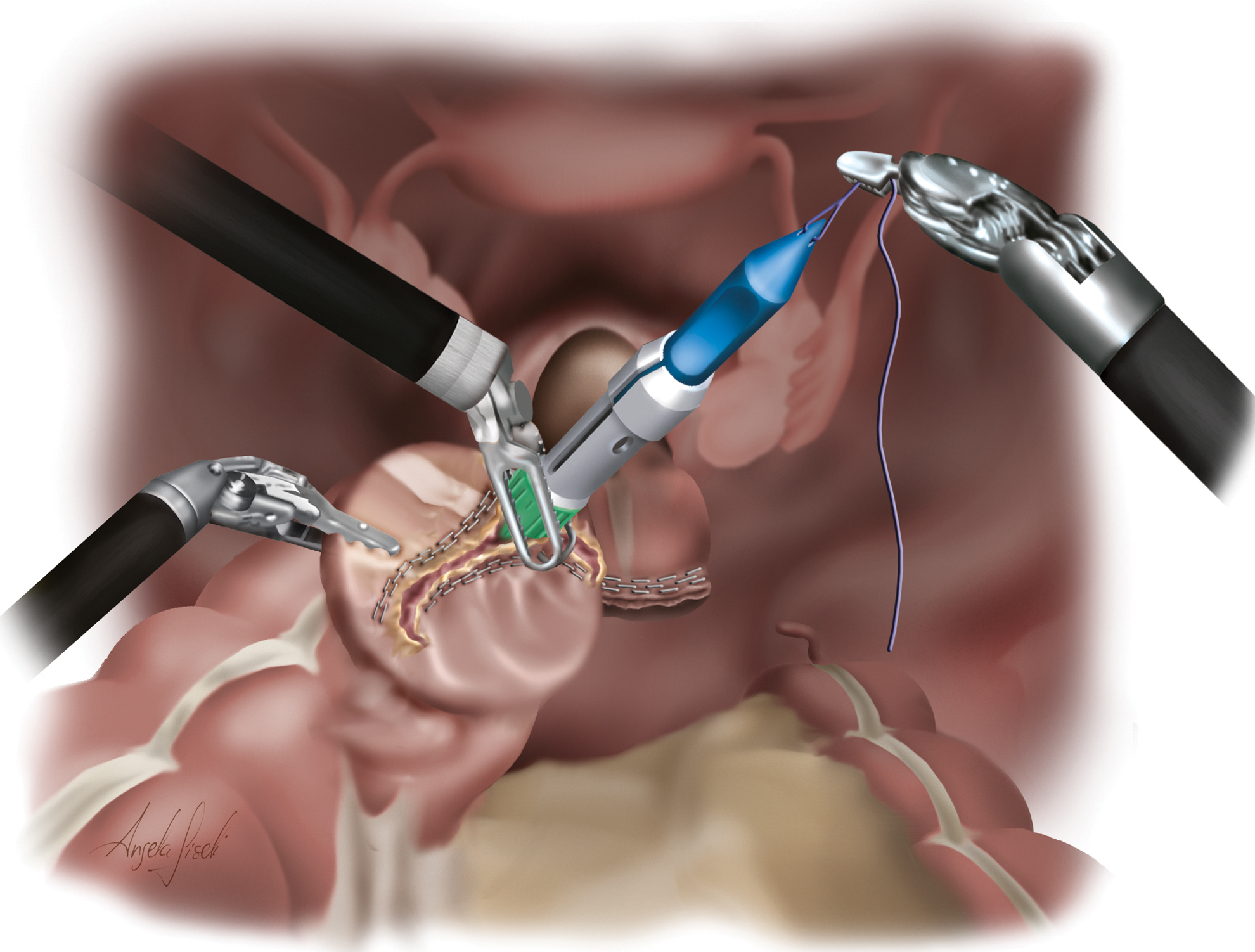
After returning to pattern port placement, the anvil was secured to the proximal colon, using a “flying saucer maneuver”; two types of anastomosis can be performed easily due to the anvil's retrieval, which was end-to-end or lateral-to-end, depending on the surgeons' choice. Posteriorly to the anvil's insertion, a “purse-string” suture can be made with No. 2-0 Prolene for margin holding (Fig. 8). Another possibility of positioning the anvil is by introducing it into the proximal bowel attached by a small suture that is followed by a linear stapling of the margin (Fig. 9). Exteriorization of its spike is made with careful traction, coming out through the stapling line or at the antimesenteric border (Figs. 10 and 11). The latter option will result in a lateral-to-end anastomosis, unlike the first option, which results in an end-to-end shape.
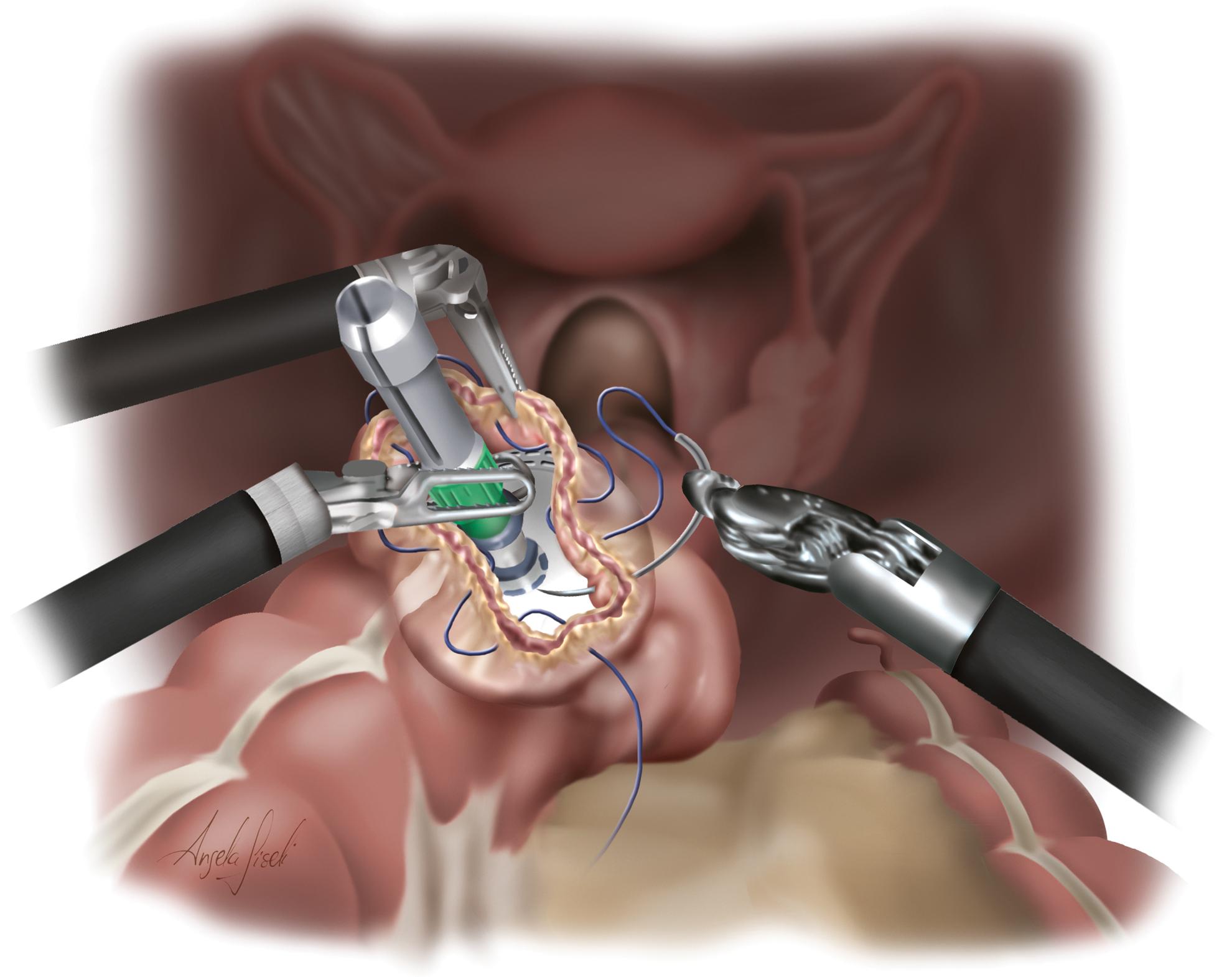
For a termino–terminal anastomosis, a “purse string” suture may be performed, holding the anvil to its margin. Color images are available online.
When opting for an end-to-end anastomosis using a linear stapler, the anvil's insertion to the proximal bowel with a prolonged stitch was used to facilitate exteriorization. Color images are available online.
After stapling the proximal margin, careful traction of the external stitch to the anvil's exteriorization fits the stitch at the bowel's margin. Color images are available online.
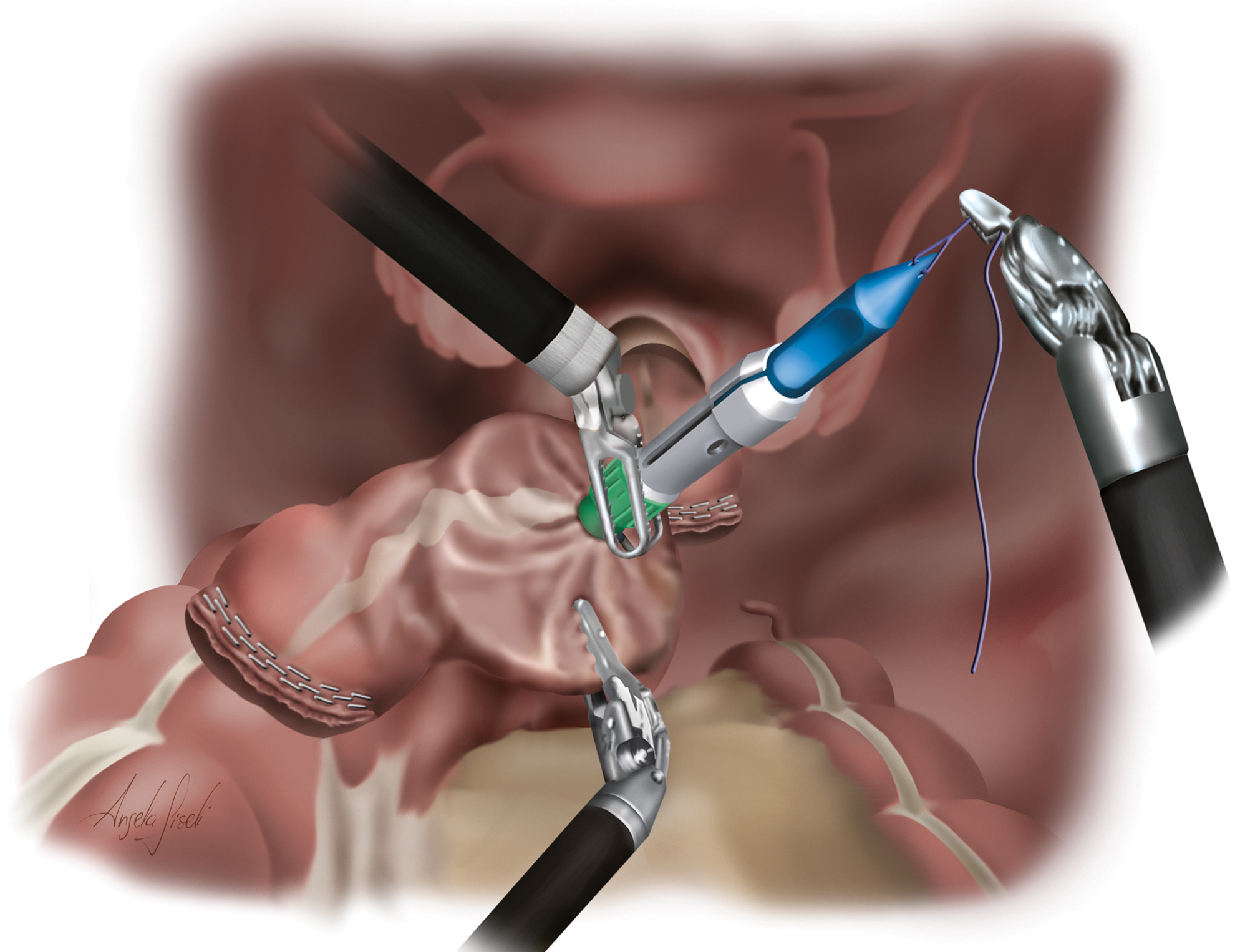
Another option for performing the anastomosis is in a lateral-to-end position by laterally extraction of the anvil on the proximal bowel. Color images are available online.
Finally, the circular stapler was inserted in the rectum, and the colorectal anastomosis was performed, end-to-end or lateral-to-end depending on the anvil's presentation (Fig. 12). If the extraction was performed transvaginally, a longitudinal colporrhaphy was made, using No. 2-0 Vicryl® (Ethicon) in a posterior-to-anterior direction. The first stitch is attached to the vaginal posterior margin, and, by assistant suture traction, a longitudinal running suture was performed with the Nos. 1 and No. 2 robot arms easily.
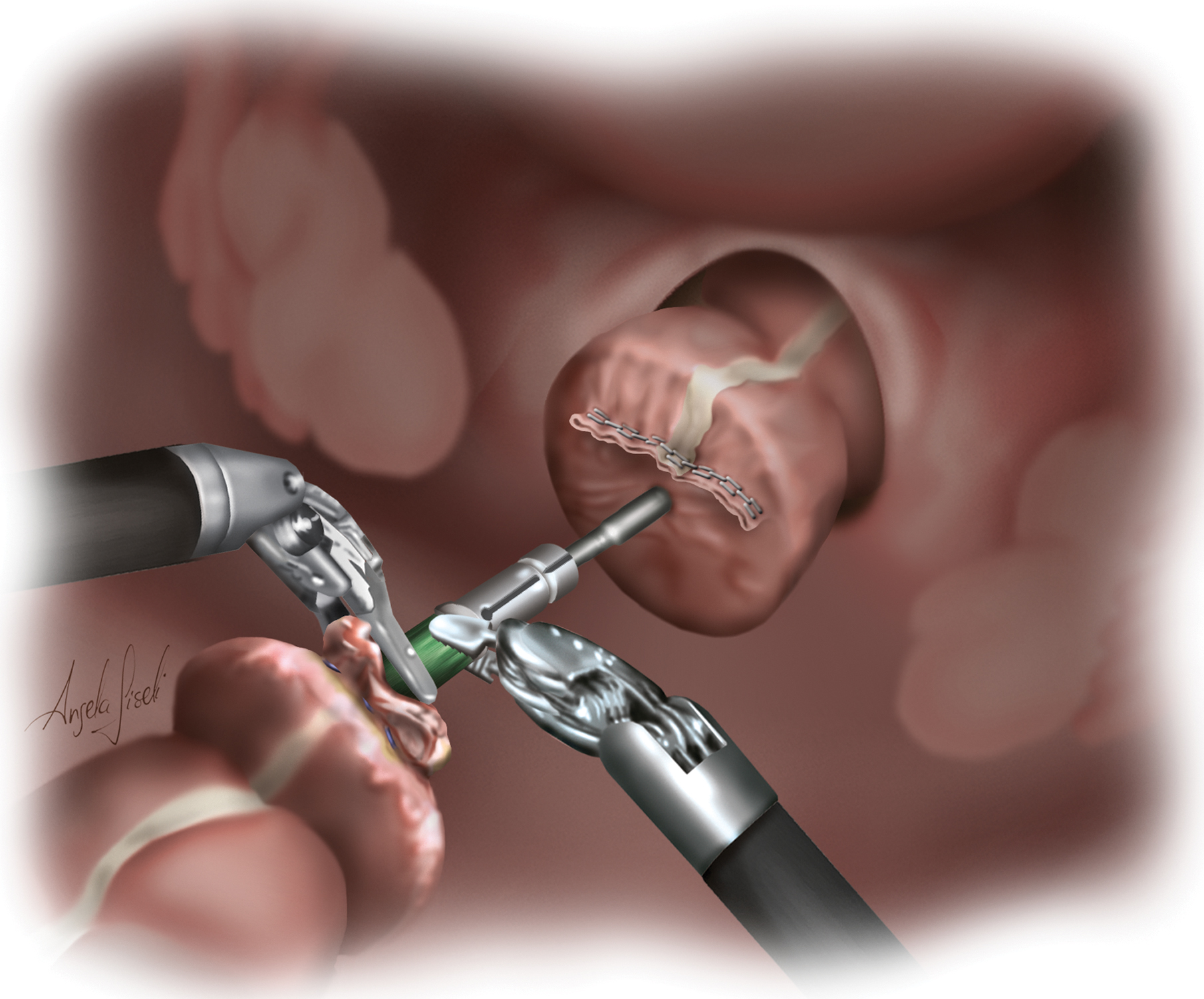
By inserting the circular stapler inside the rectal stump and correcting the anvil's attachment, the colorectal anastomosis is performed while No. 1 and 2 arms ensure best bowel positioning for hermetic stapling. Color images are available online.
Step 7. Anastomosis testing
Anastomosis integrity was tested, using methylene blue to Firefly F imaging with another 10 mg of indocyanine green for perfusion assessment, if possible. A second suture line with No. 4-0 Caprofyl (Ethicon) was performed if a methylene blue overflow was seen from the anastomosis. An additional air-leak test may also be performed if needed. The 2 remnant doughnut rings of bowel tissue extracted were also checked by a pathologist for confirmation of an endometriosis-free margin in endometrial cases. Transposing the omentum for omentoplasty may be performed in low rectal anastomosis or when concomitant colporrhaphy is performed.
Step 8. Drainage
An active silicone drain was positioned near the anastomosis for to monitor it as a routine. When performing abdominal drainage, the undocking of arm No. 3 kept the trocar in its position and facilitated the trocars' linearity. By using arm No. 1, a laparoscopic needle holder was inserted and exteriorized at the No. 3 corresponding trocar for the drain clinch.
Results
To introduce this technique, this case series involved a total of 56 patients who underwent a R-NOSE TIA procedure for treatment of colon and rectal endometriosis disease from December 2015 to October 2019. All selected patients had endometrial disease. They were helped by a multidisciplinary team and referred to the gynecology unit. In addition, the patients were evaluated with magnetic resonance imaging added to an experienced sonographer endometriosis-specific–prepared transvaginal ultrasound examination, being diagnosed with symptomatic and nonresponsive endometrial disease to medical therapy.
No colorectal malignant disease was addressed with this procedure. The median age was 36.8 (range: 28–46 years) and the mean body mass index was 22.88 kg/m2 (range: 18.9–28.3 kg/m2). Regarding the patients' clinical conditions, their American Society of Anesthesiologists Physical Status classifications ranged from 1 (normal healthy patient) to 2 (mild systemic disease).
All 56 patients underwent segmental bowel resection according to their conditions. Splenic flexure mobilization was not performed in any case and the methylene blue and air-leak test was positive in 1 case, which had an additional suture in the detected area and become negative on a second test. Firefly F imaging was used for bowel perfusion assessment before bowel resection and after anastomosis. The anvil's positioning into the proximal colon was performed with a purse-string suture in 51 cases and, in 5 cases, by positioning the anvil after linear stapling. All colorectal anastomosis were carried out in an end-to-end position; diverting ileostomy was never performed. Specimen transrectal extraction occurred in 49 cases and transvaginal extraction in was performed 7 cases. No conversion to open surgery was needed nor was blood-transfusion therapy required.
The mean length of hospital stay was 4.5 days (range: 3–6 days). Concerning postoperative complications, according to the Clavien–Dindo classification system, no severe complications were observed. All patients had normal postoperative bowel movements during hospitalization. No postoperative anastomosis leak (AL) or rectovaginal fistulae were observed. No blood transfusion was needed because of any intraoperative blood loss. Pathologic examinations of the specimens confirmed DIE in all 56 patients, and no postoperative mortality was seen.
Discussion
Endometriosis effects on general physical and mental status, and also on social well-being are well-established. Treatment should be individualized and surgical management remains the gold standard approach to DIE for improving patients' of quality of life (QoL). Different forms of surgical approach are possible for treatment, and this study introduced a robotic minimally invasive procedure with minor surgical traumata and with good outcomes.
Laparoscopic and laparotomy techniques are known worldwide as feasible for addressing colorectal diseases, with satisfactory endometriotic-tissue excision and good long-term outcomes. Laparoscopic surgery is generally preferred to laparotomy because laparoscopic surgery it is associated with shorter hospital stays, promotes quick recovery and better cosmetic outcomes, although some disadvantages have been documented. 10 Similarly, robotic-assisted surgery is spreading quickly and has shown to overcome the intrinsic limitations of laparoscopy.11,12 Three-dimensional stereoscopic vision and magnification, a stable camera platform, improved ergonomics, hand-tremor filtering, and superior range of motion and motion scaling are remarkable advantages. 13
Applied to endometriosis, fine dissection and easier identification of cleavage planes can provide better results, especially in a narrow or fixed surgical site, which is common in pelvic dissection. 14 Since the first reported robotic-assisted colorectal procedure, described in 2002 by Weber et al., 15 its feasibility has been proven and this approach can simplify and ensure safety in complex cases. 16
Totally minimally invasive colectomy of the left colon and rectum is considered effective and produces good short- and long-term results due to the use of circular staplers. 17 Regarding right-colectomy, technical difficulties with using linear staplers, and the option for intra- or extracorporeal anastomosis are still debatable. 18 DIE with intestinal bowel involvement is predominantly on rectosigmoid transitions. A totally minimally invasive procedure with intracorporeal anastomosis is safe, reduces clinical symptoms, and produces better postoperative recovery, avoiding a large abdominal incision. 19 More importantly, a totally intracorporeal anastomosis requires no extensive dissection or mobilization of the mesocolon, and decreases surgical trauma and morbidity. 20
A NOSE procedure facilitates both extraction and placement of stapler anvils into the abdominal cavity. Instead of making a small laparotomy or expanding a port site, a natural-orifice extraction results in decreased surgical trauma, less postoperative pain, and reduction of wound complications and incisional hernias. A number of series have been reported in which laparoscopic bowel resection with NOSE was used for severe endometriosis, and the results have shown improvements in safety and effectiveness. Recently, Wolthuis et al. 21 showed no major impacts, such as developing pelvic abscesses or postoperative complications related to intraoperative bowel openings and manipulations. Microbiology analysis for assessing peritoneal contamination related to colostomy procedures is still unclear in studies published in the literature.
Both transvaginal or transrectal removal are possible with NOSE procedures, and do not prolong operation times. 22 Transvaginal extraction has been established initially in NOSE because of the resulting improved healing and elasticity. This procedure is suitable for all segments of the large intestine; however, the risk of rectovaginal fistulae should be not disregarded.23,24 Proximity of staples lines and rectal and vaginal sutures may be related to the development of rectovaginal fistulae. 9 Transanal extraction must be performed carefully to protect the anal sphincter and prevent rectal prolapse. In the present technique, if the vagina stump is already opened due to endometriotic-tissue resection, a transvaginal extraction should be performed; however, when this is not manipulated, it should be made transrectally.
AL has been always a major concern in minimally invasive colorectal surgery. Although the double stapling technique shows higher safety and reduced the AL rate for intracorporeal anastomosis over hand-sewn anastomosis, the rate is still high and ranges from 5% to 19%. 25 A patient's features, the procedure(s) performed, and instruments used may influence AL occurrence. Fluorescence imaging may provide additional bowel-perfusion assessment; however, the real effect on AL occurrences remains uncertain, and requires further analysis. 26
Kawada et al. 27 demonstrated that precompression before stapler firings is an independent factor for leakage. However, Ito et al. 28 showed that 3 or more stapler firings during rectal division was a significant factor in increasing the risk of AL. An end-to-end or lateral-to-end anastomosis may be performed depending on bowel-remnant length and previous mesocolon mobilization. A purse-string suture is preferred than the use of a linear stapler to avoid an additional suture line and overlap. This approach may influence AL. 29 Regarding clinical application, when using a linear stapler, suture lines are not recommended to be overlapped. An endoscopic analysis of colorectal anastomosis identified AL occurrences related to the circular stapling line and its overlapping points, therefore, showing that additional hand-sewing reinforcement may play a role in specific cases. 30
Conclusions
The preliminary experience described in this study demonstrates a safe and feasible surgical procedure for endometriosis treatment. Recently, to the current authors' knowledge, few studies have been published in the literature on R-NOSE with a TIA colorectal procedure. This surgical approach was designed to produce good results in colorectal resection and produce evidence for endometrial treatment, improving patients' QoL.
In addition, this technique can promote better postoperative and cosmetic outcomes in cases for which minimally invasive surgery is preferable. Limitations of this study included its retrospective nature as well as having a small number of patients. Because of the modern status of R-NOSE procedures, further studies are still warranted to define long-term outcomes. R-NOSE minimally invasive procedures continue to expand worldwide, and the favorable results achieved so far are encouraging.
Footnotes
Acknowledgments
The authors thank all of medical staff members and the multidisciplinary health team for collaboration during this study's development. The research and education institutes are especially recognized for all their support.
Author Disclosure Statement
No competing financial interest exist.
Funding Information
No funding was received for this article.