
Abstract
Background:
Genitourinary tract actinomycosis is the second most frequent clinical form of actinomycosis. Although it has been recognized for over a century, owing of its infrequent and invasive nature, it often escapes proper diagnosis and mimics malignancy or tuberculosis.
Case:
This is a case of a uterine actinomycosis with extensive pelvic involvement that was preoperatively impressed as uterine adenomyosis but finally turned out to be a case of pelvic actinomycosis involving uterus, bilateral adnexae, sigmoid, and appendix.
Results:
Final histopathology revealed actinomycosis of sigmoid colon, endometrium, myometrium bilateral adnexae, and appendix.
Conclusions:
High index of suspicion and investigation to prove the diagnosis leads to optimum management of genital actinomycosis. (J GYNECOL SURG 36:214)
Background
Actinomycosis is a rare chronic disease caused by Actinomyces spp., anaerobic Gram-positive bacteria, which normally colonize human mouth, digestive, and genital tracts. Genitourinary tract actinomycosis is the second most frequent clinical form of actinomycosis. 1 Although it has been recognized for over a century, owing of its infrequent and invasive nature, it often escapes proper diagnosis and mimics malignancy or tuberculosis. 2 As a result, most of the patients undergo surgical management who if diagnosed preoperatively can be managed by prolonged antibiotic therapy. Under normal condition, Actinomyces spp. does not cross mucosal barrier, so even if detected in Papanicolaou smears, it warrants no treatment. 3 But because of mucosal trauma during intrauterine device (IUD) insertion, Actinomyces spp. may grow as colonies that extend slowly across natural anatomic boundaries, forming abscesses and sinus tracts filled with polymorphonuclear leukocytes and surrounded by thick indurated fibrotic tissue. The purulent exudate within actinomycotic abscesses frequently contains characteristic yellow or brown sulfur granules that are composed of Actinomyces colonies, tissue debris, and calcium phosphate. The incidence of actinomycosis increases with increase in number of years of use. 4
We describe a case of uterine actinomycosis with extensive pelvic involvement, which was preoperatively impressed as uterine adenomyosis but finally turned out to be a case of pelvic actinomycosis involving uterus, bilateral adnexae, sigmoid, and appendix.
Case
A 54-year-old woman, P3L3, presented at Chang Gung Memorial Hospital, Linkou, Taiwan, with chief complaints of pain in lower abdomen for 2 months. She also suffered from recent constipation without other systemic complaints. On examination, her vital signs were stable but she was severely pale. Pelvic examination showed cervix erosion and revealed IUD tail that was inserted 30 years back. Her uterus was tender, enlarged as 16 weeks gestational age with normal bilateral fornix. Ultrasonography impressed as uterine myoma with large adenomyosis and an IUD in situ (Fig. 1). Laboratory data revealed mild elevated CA-125 (49.4 U/mL) with hemoglobin of 8.8 mg/dL. Under the impression of adenomyosis with anemia, she was admitted for further evaluation and management. After transfusing 4 U of blood, she was taken up for exploratory laparotomy.

Ultrasonographic image showing enlarged uterus with suspected adenomyosis with IUD in situ. IUD, intrauterine device.
Laparotomy was done through midline incision and intraoperatively there was dense pelvic adhesion with confluent fibrosis over uterus, adnexae, cul-de-sac, sigmoid, and small intestine with abscess formation. There was right hydroureter with abscess formation in pockets of fibrosis. The sigmoid looked ulcerative with external invasion involving whole circumference. Abdominal total hysterectomy, sigmoid colectomy with primary reanastomosis, appendectomy, and cytoreduction of abscess wall were performed. As shown in Figure 2, cut surface of uterus showed yellowish irregular granular surface with areas of hemorrhage with IUD in situ. Also seen is the specimen of sigmoid colectomy with irregular hemorrhagic surface.
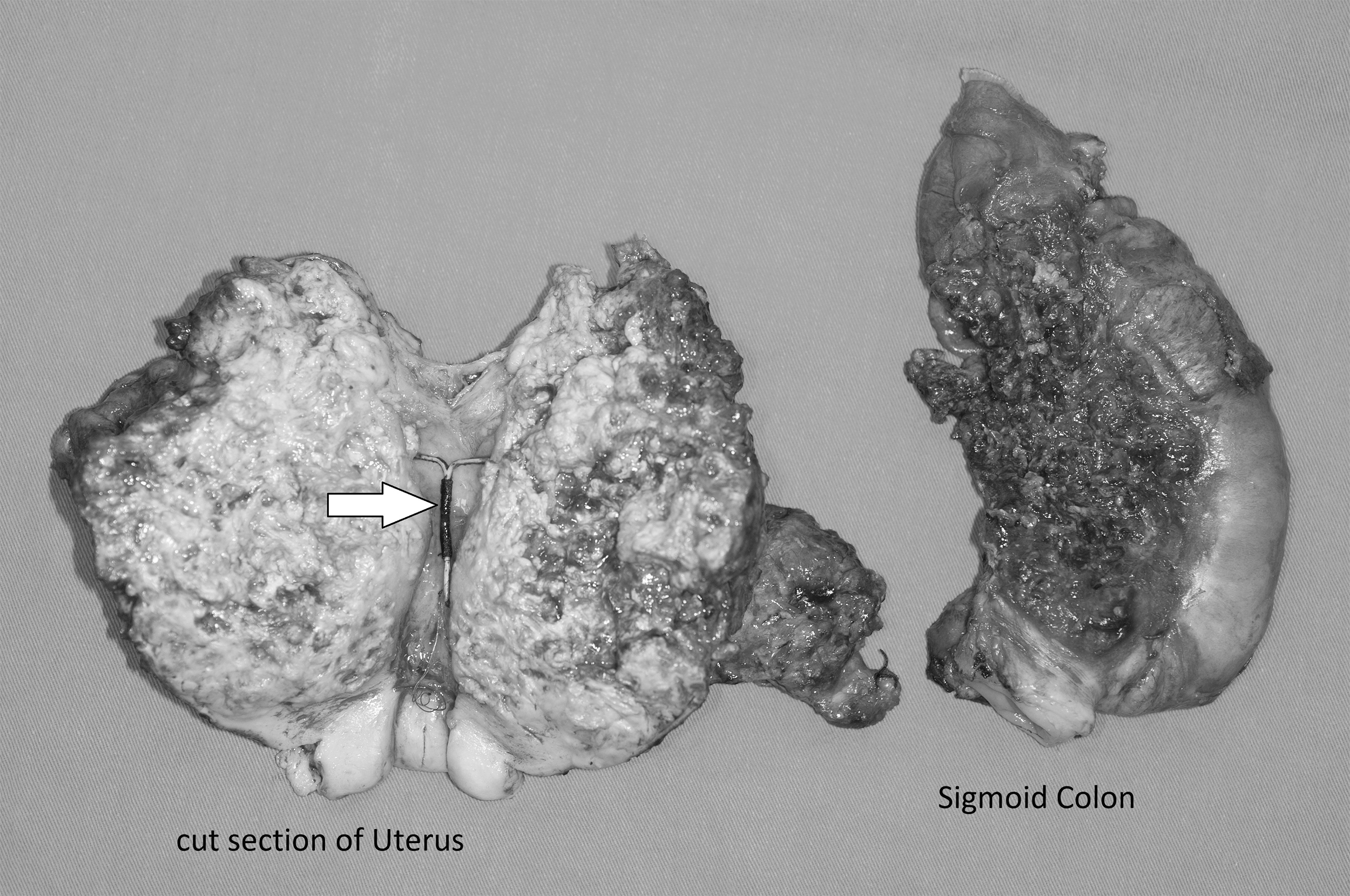
Cut surface of uterus showing yellowish irregular granular surface with areas of hemorrhage with IUD in situ (white solid arrow). Also seen is specimen of sigmoid colectomy with irregular hemorrhagic surface.
Final histopathology revealed actinomycosis of sigmoid colon, endometrium, myometrium bilateral adnexae, and appendix. Postoperatively the patient was treated with prolonged antibiotics and did well. For 3 years following surgery, she had no further evidence of persistent actinomycosis.
Discussion
IUD-associated pelvic actinomycosis is infrequent but is directly associated with duration of use. Women carrying an IUD for >5 years and presenting with a pelvic mass have a high index of suspicion for IUD-related actinomycosis. There are no data comparing copper, hormonal, or inert IUDs in terms of the risk of actinomycosis. During IUD-associated actinomycosis, abscess formation is frequently observed in the genital tract, and creates dense adhesions with contiguous structures such as small bowel, promoting extensive fibrosis, fistulas, and peritonitis.5–7 Quite similar picture of fibrosis and abscess formation was seen in our case too. Symptoms of patients with pelvic IUD-associated actinomycosis may mimic symptoms of gynecological malignant tumors, or uterine myoma or adenomyosis, by presenting as abdominopelvic mass without fever.5–7
Removal of the IUD is crucial in patients with IUD-associated actinomycosis. Open surgical resection, often required for the definite diagnosis of genitourinary tract actinomycosis, facilitates the cure, but may be mutilating, especially if hysterectomy or bladder and bowel resection is performed like the index patient. Antimicrobial therapy is the main treatment for genitourinary tract actinomycosis. Patients with genitourinary tract actinomycosis usually receive several weeks of intravenous high doses of a β-lactam, followed by oral therapy for 2 to 6 months. The duration of antimicrobials should probably be reduced in patients with extensive surgical resection of a small genital mass. Specific preventive measures by change of IUD at the end of its recommended time depending on the type used may limit the occurrence of actinomycosis.
Conclusion
Physicians must be aware of clinical presentations of pelvic actinomycosis in women with an IUD. Clinical signs of the actinomycosis can be nonspecific, frequently including indolent infiltration with abscesses and draining sinuses and can mimic other diseases, most often malignancy. High index of suspicion and investigation to prove the diagnosis leads to optimum management of genital actinomycosis.
Footnotes
Acknowledgment
The authors thank the Asia-Pacific Association for Gynecologic Endoscopy and Minimally Invasive Therapy (APAGE) for providing the International Fellowship Endoscopy Training Program at Chang Gung Memorial Hospital.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No funding was received for this article.