
Abstract
Objective:
This study aims to determine the anatomical outcome of sacrospinous fixation (SSF) technique.
Design:
This study uses a retrospective cohort design with archival study.
Materials and Methods:
Data were taken from secondary medical records for evaluation of operating outcomes of SSF, in the form of Pelvic Organ Prolapse-Quantification (POP-Q) scores of preoperative and postoperative procedure. Thirty-four patients who have gone through the inclusion and exclusion criteria were analyzed by their C-point position preoperatively and postoperatively. Paired t-test was used for normally distributed variables, whereas the Wilcoxon signed-rank test was used for not normally distributed variables.
Result:
From 34 patients, we found that the average age is 55.1 years, with a median body mass index of 25.2 kg/m2, multiparity 66.7%, prolapse stage III–IV (67.6%), and previous hysterectomy (17.6). The measurement of POP-Q score was conducted before and after the operative procedure, with an average C-point score of 3.62 ± 1.12, median of 3.0, minimum score of −1, and maximum score of +9. In measurement post-procedure, we found an average C-point score of −4.56 ± 0.82, with a median of −5.0, minimum score of −8, and maximum score of +4. From comparative analysis of preoperative and postoperative procedure, it is found to be statistically significant (p < 0.001).
Conclusion:
The SSF has a good operating outcome especially for the improvement of the apical compartment with successful rate of 14/16 (87.5%).
Introduction
Pelvic organ prolapse (POP) is a protrusion or descent of the vaginal wall along with pelvic organs inside it (uterus, bladder, intestine, and rectum) into the vagina or out of the vaginal introitus. 1 The prevalence of POP in the world as reported by various studies varies greatly from 3% to 50%. 2 In the United States, 6% of women aged between 20 and 29 years are affected by POP. While for women aged 50 to 59 years, it reaches 31%. Nearly 50% of women with POP are aged 80 years or older. 3
Based on epidemiologic studies, there are several factors that can increase the risk of POP (primary prolapse), such as vaginal delivery, old age, menopause, increased intra-abdominal pressure, and obesity.4,5
Signs and symptoms of prolapse are closely related to the degree and location of the prolapse. 6 Prolapse location can be identified through physical examination via inspection of third- and fourth-degree prolapse. Speculum examination is useful for evaluating prolapse below third degree. Afterward, the physical examination findings are applied to POP degree classification using Pelvic Organ Prolapse-Quantification (POP-Q). 7
The most notable impacts of POP are pelvic pain, urinary disorders, defecation problem, and also sexual dysfunction. All these problems are non-life-threatening; nevertheless, it can significantly diminish women's quality of life. Therefore, the management of POP has to be precise and individualized to each patient.
The management of POP cases is currently divided into two options: conservative and operative. A conservative approach (use of pessary, healthy lifestyle modification, and pelvic floor muscle training) is carried out in mild-to-moderate cases, especially in women who are still sexually active and are planning to have children. However, in moderate-to-severe POP (degrees >2) in women who have had enough children, definitive therapy/surgery that aims to prevent recurrence is highly recommended.8,9
Definitive therapy for POP is through surgical intervention that includes reconstruction (sacrospinous fixation [SSF], McCall culdoplasty, uterosacral ligament suspension) and obliteration (colpocleisis). SSF technique is one of the techniques often used in Cipto Mangunkusumo Hospital (RSCM). Beside its relatively high success rate (70%–80%), SSF has other advantages such as short procedure duration, faster postoperative recovery, and minimal incision wound.8,10,11 Although SSF is used very often worldwide, data of anatomical appearance and recurrence rate of postoperative POP in Indonesia are still limited. Thus, this study is conducted to determine the anatomical outcome of SSF technique.
Materials and Methods
This study is a descriptive one with retrospective cohort design. Secondary data were obtained from patients' medical records that include evaluation of postoperative POP-Q after SSF procedure in RSCM. The study was conducted in RSCM from March 2019 until November 2019. Subjects in this study are postoperative POP patients who have undergone SSF procedure in RSCM from January 2013 to December 2018. Data were taken retrospectively to observe anatomical outcome after SSF procedure. There are no ethical problems in this study as it is based on secondary data (medical records).
Inclusion criteria in this study are women with POP who have undergone SSF reconstructive technique in RSCM from 2013 to 2018, patients who were studied have medical records stored in RSCM, patients who came to outpatient clinic after the surgery, and patients who have POP-Q obtained by obstetrics and gynecology (OBGYN) specialist (trainee) or urogynecology consultant. While the exclusion criteria are patients with recurrent POP history who have at least two surgeries before, active smoker, patients who did not show up to the outpatient clinic within 3 months after the surgery, patients who only checked once for POP-Q after the surgery, and unreadable or unwritten C-point in POP-Q evaluation in the medical record.
Total sampling method was applied in this study, which includes all available and accessible medical records. Data analysis was performed using SPSS 20. Demographical data distribution is processed with descriptive univariate analysis and is represented as mean and median. Qualitative data are presented in both narrative and table form, whereas quantitative data will be first analyzed for its data distribution using the Kolmogorov–Smirnov test to observe whether it is normally distributed or not. Data with normal distribution are presented as mean ± standard deviation. However, data that are not normally distributed are presented as median. Data presentation for descriptive result and data analysis are made in the form of text, table, or diagram.
Results
Data collection was obtained from 2013 to 2018, and there were 92 reconstructive surgeries with SSF technique. From this number, further screening was conducted. A total of 58 subjects were excluded due to missing medical records, unmet inclusion criteria, insufficient number of visits to outpatient clinic, and incomplete or irrelevant POP-Q results. At the end of screening process, a total of 34 subjects were eligible for data analysis.
From these 34 subjects, 19 underwent total vaginal hysterectomy, SSF, anterior colporrhaphy, and colpoperineorrhaphy. Furthermore, eight patients who had apical vaginal prolapse have undergone SSF and seven patients have undergone sacrospinous hysteropexy. Cervical hanging onto sacrospinous ligament was performed for patients who want to preserve their uterus. Surgeries were conducted by OBGYN trainee under the supervision of urogynecology consultant.
In this study, 24/34 (70.5%) patients were younger than 60 years, with an average age of 55.1 years. Patients who had nonobese body mass index (BMI) were 58.8%, and 67.6% had severe POP (third or fourth degree). Based on parity status, there were 23 multipara subjects (70.7%) and 1 nullipara subject. Based on the baby's birth weight, there were 10 subjects with a history of giving birth to macrosomia. Seventy-three percent of the subjects had never had a hysterectomy before. There were no patients with a history of smoking. There were 79.4% of patients who came to the hospital with BPJS (national health insurance) payment/referral. Subject characteristics are summarized in Table 1.
Subject Distribution Based on Demographic and Obstetric Characteristics (n = 34)
BPJS, government insurance.
BMI, body mass index.
Anatomical outcome after SSF procedure
Preoperative and postoperative C-point comparison
On preoperative POP-Q score measurement, C-point average of 3.62 ± 1.12 was obtained, with a median of 3.0, minimum value of −1, and maximum value of +9. In normality test, data distribution was not normally distributed (p = 0.03). C-point evaluation was obtained from POP-Q score from the patients' last visit to the outpatient clinic. An average of −4.56 ± 0.82 and median of −5.0 were obtained on postoperative C-point measurement, with a minimum value of −8 and maximum value of +4. Normality test on postoperative C-point shows that data were not normally distributed (p = 0.01). Data distribution is shown in Table 2.
Preoperative and Postoperative C-Point (Wilcoxon Signed-Rank Test on Variables with Data Not Normally Distributed)
POP-Q, pelvic organ prolapse-quantification.
Analysis of C-point difference before and after operation was conducted using the Wilcoxon signed-rank test. The result showed significant improvement in C-point before and after operation (p < 0.001) (Fig. 1).
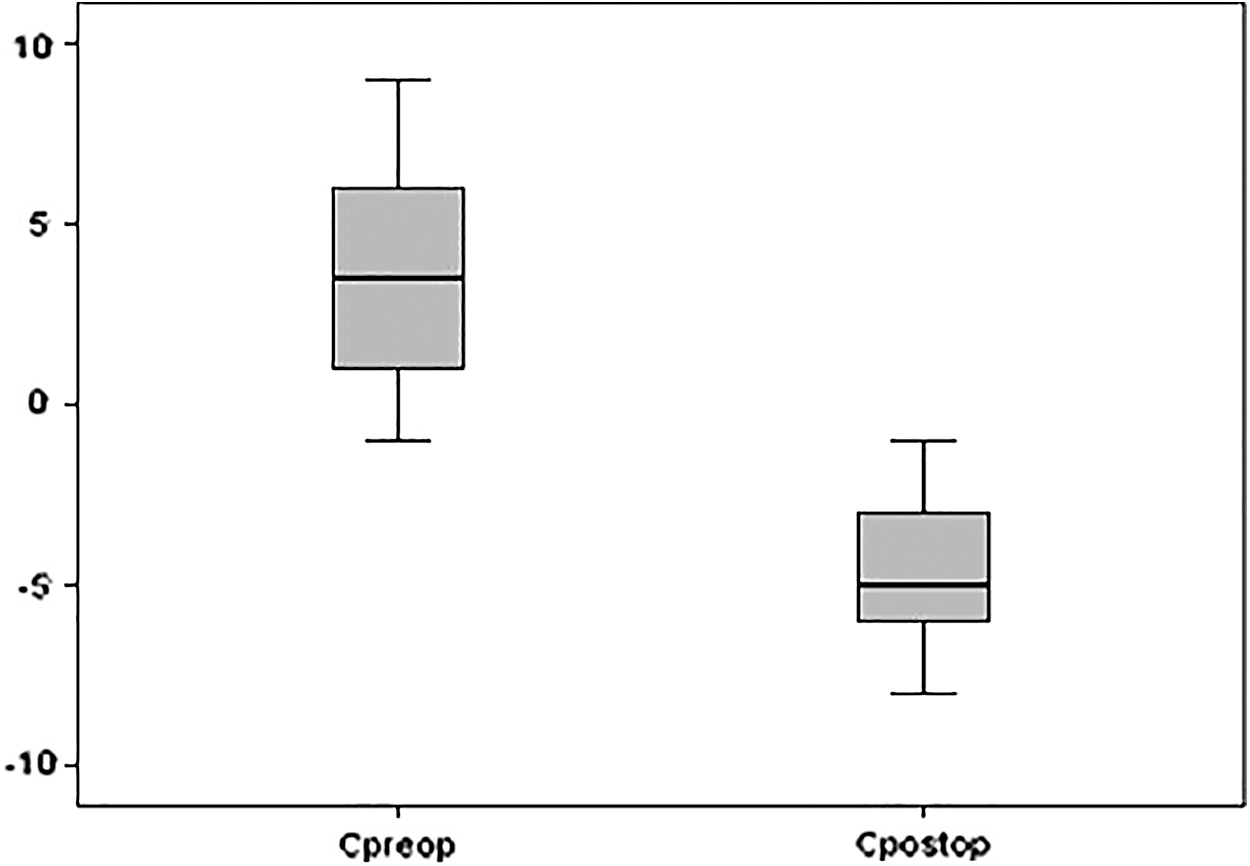
Pre-SSF and post-SSF C-point. SSF, sacrospinous fixation. Analysis of C-point difference between pre-operative and post-operative was conducted using Wilcoxon Signed Rank Test. The result showed significant improvement in C-point before and after operation (p < 0.001).
Postoperative C-point changes
In this study, there were 22 patients who came for follow-up at least twice. POP-Q score changes were taken when patients came on the 3rd, 6th, and 12th month after operation. Of the 22 patients who came for follow-up on the third month, two groups were divided based on the last time patients came for follow-up. The first group consists of patients who returned only on the 6th month (8 patients), whereas the second group consists of patients who returned on the 12th month (14 patients). Statistical test was conducted based on paired data (on the same subject) principle to obtain POP-Q score changes between the time the patients came for follow-up the first time and the second time in each subject group. The result of C-point measurement on the third month after operation and the 6th or 12th month after operation is shown in Table 3.
Changes in C-Point After Operation
Correlation test using paired t-test on variables with normal distribution.
Correlation test using the Wilcoxon signed-rank test on not normally distributed variables.
Statistical test on C-point measurement on the third month in group 2 (last visit 12 months ago) shows that there was significant difference with p = 0.01.
As shown in Figure 2, there is a decrease in C-point on subject group that came to outpatient clinic between third and sixth month (group 1), with an average of 0.62 cm (from −5.25 to −4.63 cm). Subjects who came to outpatient clinic between month 3 and month 12 had a decrease in C-point, with an average of 1.74 cm (from −5.71 to −3.93 cm).

Average decrease of C-point on subjects on 6th month
POP recurrence after SSF procedure
In total, 34 patients were followed-up in this study. There were 16 patients who came for follow-up at 12 months after operation. Postoperative recurrences were found in 2 of the 16 patients (12.5%). Of those two patients, one needed only observation, whereas the other one had grade 3 prolapse recurrence with +4 C-point. We performed reoperation on this patient 1 year after the initial operation. The illustration of the recurrence is shown in Figure 3.
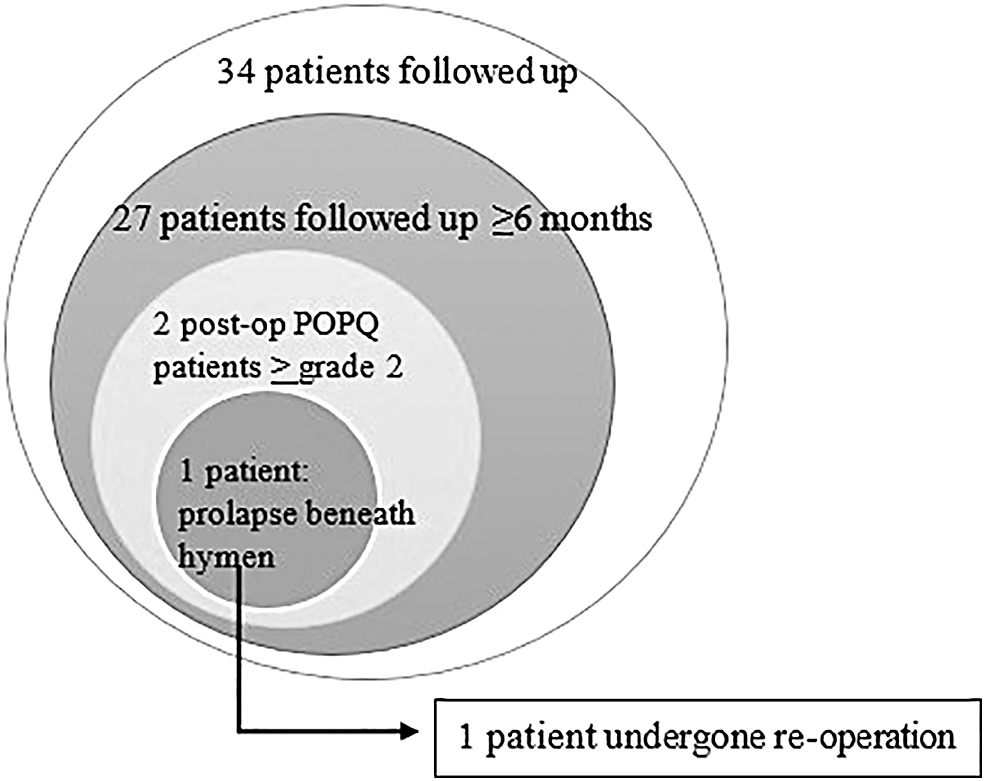
POP recurrence on post-SSF patients.
Characteristics between these two patients who had recurrences had some differences. The first patient had recurrent POP 12 months after operation, with parity history of six with spontaneous delivery. The biggest birth weight was 4200 g. Patient also had a history of hysterectomy due to large uterine fibroid and had grade 4 apical vaginal prolapse. The patient was 55 years old with normal BMI.
Conclusions
Sample characteristics
There were 28 patients who were excluded from this study. On further investigation, 21 patients were unreachable and 7 patients could not be followed-up for several reasons, such as living in a distant area, administrative problems, and 1 died from heart attack.
In this study, 70.5% (24/34 subjects) used national health insurance (BPJS), which obligates patient to obtain referral letter from primary health care to go to the next level of health care facility until they reach RSCM. This is a major problem for the patient as it requires a lot of time to get the referral letter. This becomes more problematic for geriatric patients.
Dropout subjects or subjects lost to follow-up are also a common risk for studies with cohort design. This condition is also found in a study in Nepal by Dangal et al., which has 95 subjects participating in the beginning, but only 38 showed up for follow-up after 6 months. 12
The average age of the subjects is 55.1 years. A study by Jelovsek et al., which had 138 patients who underwent SSF procedure, also has a quite similar average age, which is 56 years. Age is one of the risk factors for POP. 13 A meta-analysis by Vergeldt et al. showed that people aged 52 to 55 years have more risk of suffering from POP, compared with people aged 51 years with odds ratio (OR) of 1.5 (1.1–2.0). 14
The average BMI in 41.2% of subjects (14/34) in this study is 25.2 kg/m2. Similar finding is also found in a study by Rajan et al., in which the average BMI of subjects who underwent SSF is 25.5 kg/m2. 15 In this study, BMI of subjects is categorized into overweight (BMI 25–30 kg/m2). Excessive BMI is another important risk factor for POP. Chronic increase of intra-abdominal pressure is the mechanism of POP in obese people as this increase in the abdomen put stress on the pelvic floor. 16
In this study, 67.6% (23/34) of patients had severe prolapse (third to fourth degree). This finding is different, compared with a study in Spain where 57% of POP patients had first- to second-degree prolapse. It is suggested that women in developing countries are more likely to feel ashamed of their condition, which makes the severity of the prolapse become even more worrying. 17
Based on the obstetric history, in this study, 67.6% (23/34) of patient had multiparous history with 29.4% (10/34) had at least one child with over 4000 g in birth weight. Parity history is one of the most reliable predictors of POP. A study by Rodríguez-Mias et al. found that women with at least two children had a higher risk of having POP. The birth weight of the baby is also related to degree of pelvic floor compression. 18
In this study, the assessment of the POP-Q score, especially the postoperative C-point, showed a significant change when compared with the preoperative C-point. We can say that clinically, the surgical procedures performed are quite successful in improving the condition of POP in patients. Although the measurement of postoperative anatomical outcomes with POP-Q assessment takes a little bit longer time than normal gynecologic examinations, POP-Q has several advantages. With the experience of repeated measurements on the examiner, the time required in the examination decreases. In addition, POP-Q measurements are more objective. In other words, measurements by different examiners will produce the same score. 19
In the statistical test, there was a significant decrease in C-point between 3 months and 12 months postoperatively, with an average reduction of 1.7 cm. Although statistically there is a significant decrease, but it is not clinically significant. There is no change in the degree of postoperative prolapse in patients.
As shown in Table 4, when compared with other studies, the results vary in each study. This is due to the differences in the populations being studied, the method of surgery, differences in grouping of subjects, number of subjects, and duration of follow-up during the study. In this study, an evaluation of C-point was obtained at 3, 6, and 12 months postoperatively, with an average of −5.55, 4.63, and −3.93, respectively. These results are similar to the study by Halaska et al., which compared the operating outcomes between SSF and mesh application. 20 Meanwhile, in another study by Peterson et al., it was found that recurrence and anatomical failure are more common in recurrent prolapse than in primary prolapse. At 2 years of follow-up, POP-Q scores were found to worsen in both primary and recurrent prolapse. 21
Postoperative Pelvic Organ Prolapse-Quantification Score on Other Studies
In this study, recurrence was defined from patient's visit 12 months after the surgery, where apical recurrence was found in 2 of the 16 patients (12.5%). When viewed from subjective outcomes, failure (third-grade prolapse recurrence) occurred in one patient (6.25%), with success rate of 93.75%. In various literatures, it is mentioned that the success rate of SSF operations varies greatly from 67% to 99%, which may be caused by variation in the population, study design, number of subjects, or the definition of failure itself. 22 In this study, prolapse recurrences occurred in two patients. Both patients have inconsistent characteristics of risk factors, for example, BMI (excessive and obese) and the degree of preoperative prolapse (grade 2 primary prolapse and grade 4 vaginal peak prolapse). The similar factors between the two patients were multiparity and both were younger than 60 years. In both patients, other risk factors identified were history of transabdominal hysterectomy for uterine myoma, and the other patient had a chronic cough caused by tuberculosis and is currently on therapy. Complete subject characteristics are shown in Table 5.
Characteristics of Subjects with Recurrent Prolapse
SSF, sacrospinous fixation; SSH, sacrospinous histeropexy; TBC, tuberculosis.
Subject 1 characteristics
In this study, one subject who experienced recurrence had a diagnosis of preoperative grade 4 apical vaginal prolapse, whereas the other subject had grade 3 uterine prolapse. Both subjects who experienced recurrence had severe POP. In severe POP (third to fourth degree), it may indicate weakness of pelvic organ support tissue. Thus, it can affect the incidence of postoperative recurrence of prolapse.
In addition to the number of parities, another obstetric risk factor that plays major role in the failure of POP surgery is the largest baby birth weight. One of the subjects had a history of macrosomia delivery with a birth weight of 4200 g. This is consistent with the results of a study by Manodoro et al., which stated an increased risk of postoperative recurrence in subjects with a history of macrosomia (OR 2.7). 24 Similar results were also found in a study by Cam et al., where postoperative failure was more commonly found in subjects with a history of macrosomia (p = 0.001). 25
History of hysterectomy is another factor in recurrence of postoperative POP. Surgical procedures for apical vaginal prolapse are considered more difficult than primary uterine prolapse. However, studies that directly compare uterine prolapse and apical vaginal prolapse are still very rare.
Subject 2 characteristics
Subject 2 is 59 years old. Age factors can affect the incidence of postoperative POP recurrence. These results are consistent with research by Whiteside, 26 where women aged younger than 60 years had an increased risk of recurrence with an OR of 3.2 (1.6–6.4). Various literatures stated that women who experience POP at a young age will be at risk of suffering from postoperative recurrence, compared with older subjects. 27 This can be caused by genetic factors and connective tissue weakness, as well as nerve damage, muscle, and fascia. 28
Besides age, subjects with recurrent POP also had risk factors in the form of multiparity (five or more). Physiologically, vaginal delivery causes severe stretching of tissue at the base of the pelvis and does damage to the pudendal nerve, which in turn causes ligament weakness in the pelvic region.
In this subject, morbidity was found in the form of chronic cough (pulmonary TB on therapy). Chronic cough can cause repetitive rise of intra-abdominal pressure. This can result in weakening of the pelvic floor muscles and lead to POP and also increases the risk of reoperation. 29
From this study, there are three important points. First, there was a significant improvement in preoperative and postoperative C-point (p < 0.01). Second, there was a statistically significant decrease in C-point at the evaluation 3 and 12 months postoperatively (p = 0.01), but this was not clinically significant. Finally, the success rate of SSF in the 2013 to 2018 RSCM period was 14/16 (87.5%), with recurrence in two cases. Based on these findings, we can safely say that SSF has a good operating outcome, especially for the improvement of the apical compartment with successful rate of 14/16 (87.5%).
This study inevitably comes with limitations and weaknesses. One thing that needs improvement in future studies is the sample size. In this study, the sample sizes were not large enough. We hope that in the future, there is a similar study with sample size large enough to draw a more convincing conclusion. A considerable amount of dropouts was also a problem as many patients did not turn up for follow-up procedures. Another aspect that can be improved is the assessor for POP-Q evaluation after the procedure. In future studies, subjective bias would be reduced if the assessor for postsurgical POP-Q is not the surgeon who conducted the operation. Instead, a blinded assessor should be the one to evaluate the postsurgical POP-Q.
Footnotes
Acknowledgments
The authors want to express our deepest gratitude to all consultants and residents of Obstetrics and Gynecology Department of Cipto Mangunkusumo Hospital who have assisted in supporting this study. They are Budi Iman Santoso, PhD, Suskhan Djusad, PhD, Surahman Hakim, PhD, Fernandi Moegni, MD, Tyas Priyatini, MD, Achmad Kemal, MD, and Joedo Prihartono, MD.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.