
Abstract
Background:
Accessory cavitated uterine mass (ACUM) is a rare congenital anomaly of Mullerian ducts that presents with severe dysmenorrhea in young women. It responds poorly to medication and requires surgical management for resolution of symptoms.
Case:
We report the cases of two young women who presented with medically refractory dysmenorrhea. They were initially diagnosed with subserosal fibroid and rudimentary uterine horn, respectively. After failure of all forms of medical treatment for dysmenorrhea, they underwent laparoscopy. Intraoperatively, we diagnosed them with ACUMs, and successfully performed complete laparoscopic excision and repair.
Results:
Histopathological evaluation in both cases confirmed the presence of endometrial glands and stroma in surrounding hyperplastic myometrium. Both of the patients experienced immediate and complete relief from dysmenorrhea postoperatively.
Conclusions:
Dysmenorrhea is a significant cause of loss of productivity and reduced quality of life in women. The usual algorithm of management in young women involves a variety of medical regimens, reserving surgery for only for severe unrelenting cases. Accessory cavitating uterine mass is a congenital anomaly that may present at any age, may be misdiagnosed, and is unresponsive to medical therapy. It requires a high degree of suspicion, proper evaluation with preoperative imaging, and first line surgical management for prompt relief.
Background
Dysmenorrhea, pelvic pain is one of the leading causes of absenteeism from school or work, with a prevalence ranging from 16% to 91% in women of reproductive age. The prevalence of severe dysmenorrhea may be 2%–9%. 1 Primary dysmenorrhea, which begins a few months after menarche, is most often physiological. The well-known causes of secondary dysmenorrhea, which has an anatomic basis, include leiomyomas, adenomyosis, pelvic inflammatory disease, and endometriosis. 2
Accessory cavitated uterine mass (ACUM), which represents a congenital malformation caused by a defect in Mullerian duct development, is a rare, misdiagnosed, and under-recognized cause of medically unresponsive dysmenorrhea. We present two cases of ACUMs that were misdiagnosed on imaging. Surgical intervention led to correct diagnosis and treatment.
Case
Case 1
Our first patient was a 22-year-old nulliparous nonsexually active lady who presented with severe progressively worsening dysmenorrhea since 3 years, with a visual analogue scale (VAS) score of 10. She had attained menarche at the age of 14 years, and had regular menstrual cycles. She received multiple classes of medication, including mefenamic acid, oral contraceptive pills, and oral dienogest, but she had minimal pain relief, even with parenteral analgesics.
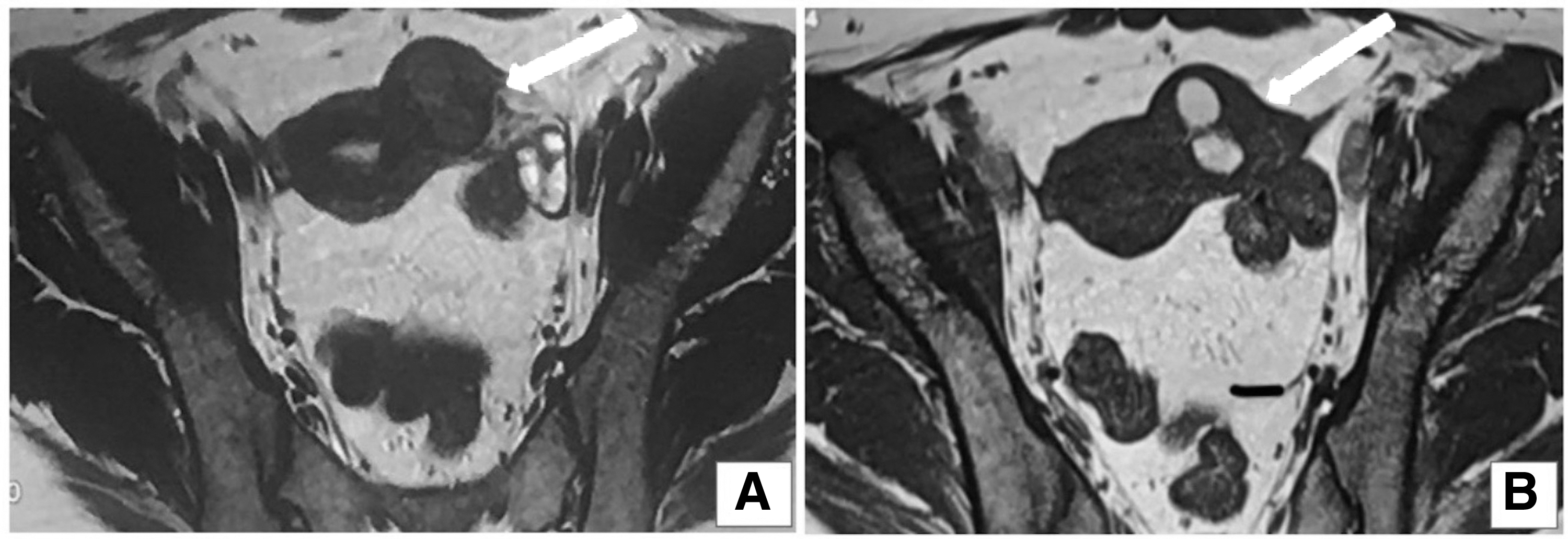
We further evaluated her with magnetic resonance imaging (MRI) of the pelvis, which showed a T1/T2 hypointense mass lesion of 4.4 × 3.6 × 3.2 cm, seen contiguous with the left lateral aspect of uterine fundus. Two cystic areas were seen within the lesion that appeared hypointense on T2 (Fig. 1A) and hyperintense on T1 (Fig. 1B), suggesting hemorrhagical contents. Uterine cavity and both ovaries were normal. With this appearance, our preoperative diagnosis was subserosal fibroid with hemorrhage, with the differential diagnoses of rudimentary horn and ACUM. She was planned for laparoscopic management, taking consent for myomectomy.
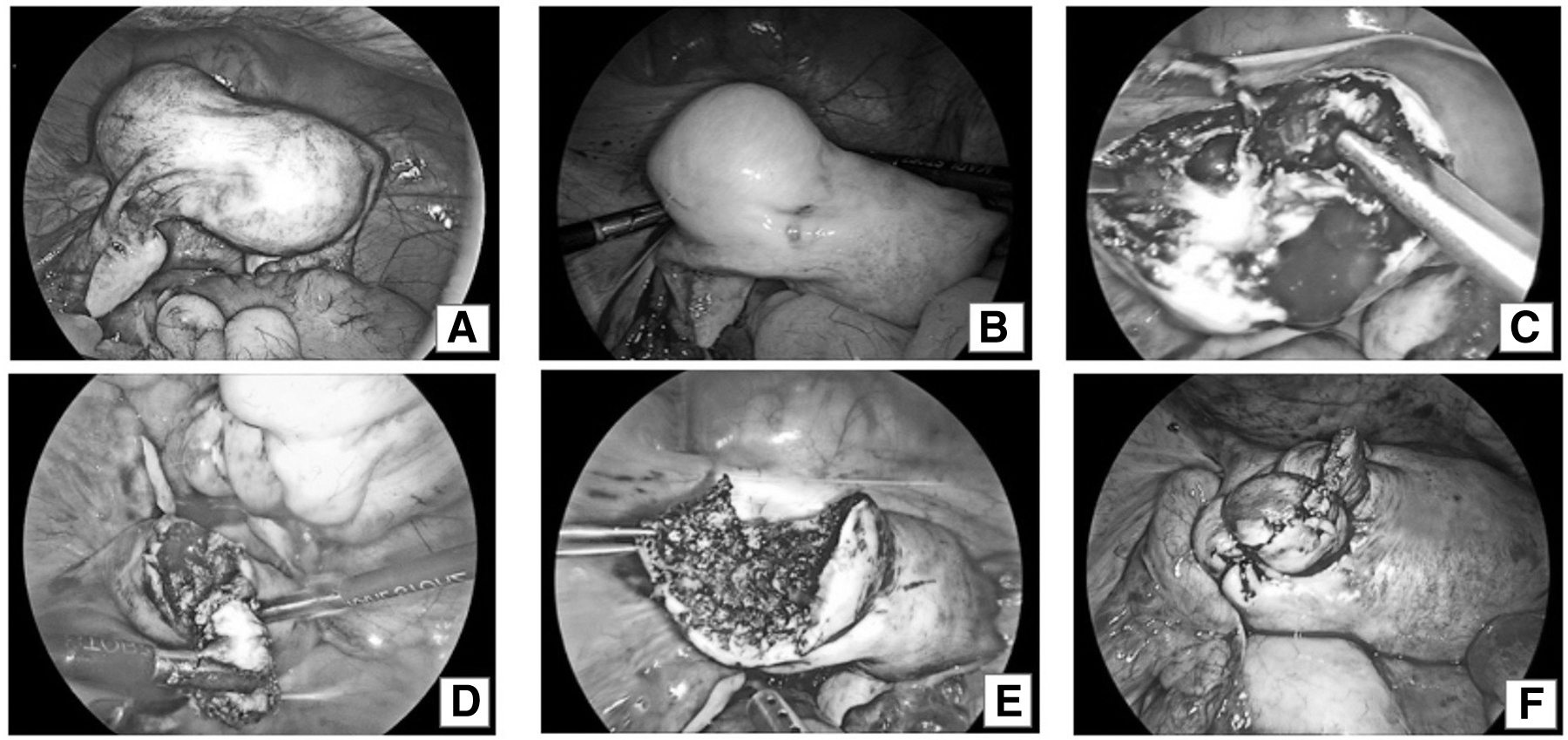
On laparoscopy, the uterus showed a visible anterior swelling 4 × 4 cm below the insertion of left round ligament (Fig. 2A). Both tubes and ovaries were healthy. Dilute vasopressin (20 IU in 200 mL) was instilled at the base of the nodule (Fig. 2B). Oblique incision was given over the cystic mass with Harmonic Ace scalpel (Ethicon Endo-surgery, Cincinnati, OH) till a cavity (2 × 2 cm) was reached (Fig. 2C). Chocolate colored thick content was drained. On further probing, a similar deeper cavity (1.5 × 1.5 cm) was encountered (Fig. 2D). The lesion was dissected all around from the surrounding normal myometrium. Endometrial cavity remained intact. The residual myometrial defect after excision of the nodule (Fig. 2E) was closed in two layers with barbed V-loc suture (Covidien) (Fig. 2F). The specimen was extracted by a 12 mm morcellator (Rotocut, Karl Storz). On diagnostic hysteroscopy, the uterine cavity was normal in shape with normally located ostia. The operating time was 62 minutes with 50 mL blood loss. There was no intraoperative or postoperative complications.
Case 2
The second case was a 29-year-old para 1 with worsening dysmenorrhea (VAS score 9) over the past 3 years. She had undergone one cesarean section 2 years ago, but her intraoperative findings were reported as normal. She received multiple modalities of medical treatment, but with minimal relief. MRI of pelvis was suggestive of unicornuate uterus with noncommunicating cavitory right-sided horn 3.4 × 3.1 × 3.5, with internal hemorrhagical content (Fig. 3). She was planned for laparoscopic excision of right horn with diagnostic hysteroscopy. On laparoscopy, a 3 × 3 cm bulge was seen anterior to the insertion of the right round ligament of the uterus. On incision, thick chocolate colored contents were drained from a single cavity. The nodule was dissected all around from the surrounding myometrium and extracted by morcellation. There was no communication of the mass with the endometrial cavity. The myometrial defect was sutured in layers with V-loc barbed suture. The operating time was 68 minutes, with minimal intraoperative blood loss. Her hysteroscopy findings were normal.

MRI pelvis of the second case suggested unicornuate uterus with noncommunicating cavitatory right-sided horn 3.4 × 3.1 × 3.5 cm with internal cavity 1.8 × 1.4 cm showing internal hemorrhagical content.
Results
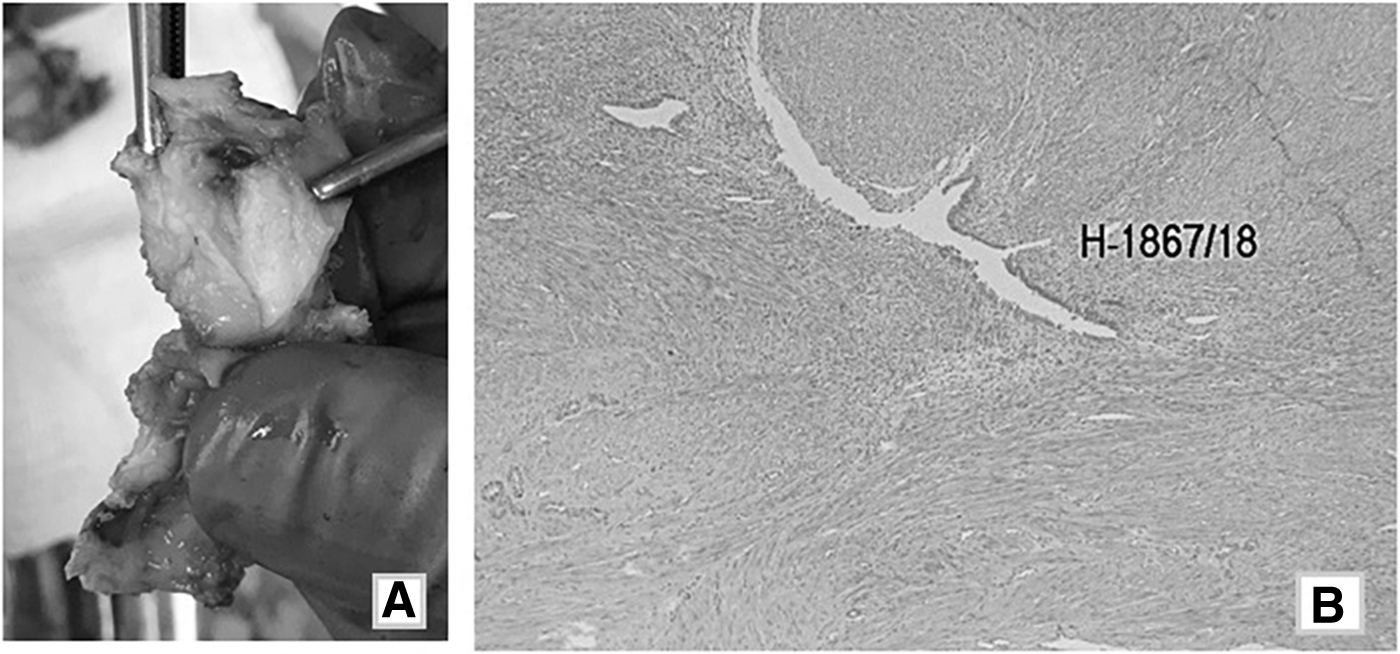
Gross histopathological examination of the first patient revealed two individual chocolate filled cavities encased in the myometrium (Fig. 4A). Microscopic evaluation showed the intrusion of endometrium glands in the surrounding myometrium (Fig. 4B). Similarly, in the second case, histopathology confirmed the presence of a cavity lined by endometrium and glands with invasion into the surrounding hypertrophied myometrium. These were consistent with the description of ACUM.
Both the patients were discharged on the second postoperative day. The first patient was followed up for 10 months postoperatively. She had immediate and persistent relief of dysmenorrhea, with a VAS score of only 2 during subsequent menses. The second patient was followed postoperatively for a duration of 6 months and also reports a drastic improvement in dysmenorrhea.
Discussion
Dysmenorrhea is one of the leading contributors to loss of disability-adjusted life years in women. Accessory cavitating uterine masses are an ill-recognized cause of dysmenorrhea in young women, leading to frequent hospital referrals, which ultimately requires surgical treatment in expert hands.
Accessory cavitating uterine mass refers to a uterine like cavity with endometrial lining, surrounded by myometrium, with no connection to the actual endometrial cavity. 3 A similar pathology, juvenile cystic adenomyoma, was defined by Takeuchi et al. 4 as a “solitary myometrial cyst measuring >/−1 cm that is surrounded by hypertrophic endometrium, independent of the uterine lumen, and presents in women <30 years of age in association with severe dysmenorrhea.” These authors felt that this was a variant of cystic adenomyosis rather than a congenital anomaly. Acién et al. hypothesized that what was earlier described as juvenile cystic adenomyosis was the same entity as accessory cavitating uterine mass. 5
The embryological origin of an ACUM could be displaced endometrial tissue, related to dysfunction of the gubernaculum. 6 Acién et al. have gone further to state that ACUM is a separate class of uterine anomaly and should be considered as a unique type of Mullerian anomaly. 7 The diagnostic criteria proposed by Acién et al. 6 are (1) an isolated accessory cavitated mass usually located under round ligament; (2) normal uterus, fallopian tubes, and ovaries; (3) pathological confirmation of excised mass; (4) an accessory cavity lined by endometrial epithelium with glands and stroma; (5) chocolate brown colored fluid contents; (6) no adenomyosis in the uterus (if resected).
Both of our cases are in line with the mentioned diagnostic criteria, adding two cases to the literature of <50 cases reported, some of them under the moniker of juvenile cystic adenomyosis.8–12 The second patient had undergone cesarean section, which reported normal findings, indicating that the original uterine cavity was completely normal. Regardless of the name of the lesion and embryological origin, the clinicians should be aware of its pathophysiology and approach to management.
ACUM should be suspected in young women (<30 years) presenting with severe gradually progressive dysmenorrhea. They have no relief with medical management, with a single case report describing satisfactory response to oral contraceptive pills. 13 It may present soon after menarche, several years after menarche, or even after childbirth. Alkhateeb and Yaseen described an intriguing case of twin pregnancy in the ACUM, in which the diagnosis was prompted by miscarriage and failed curettage. 14 We are unsure why these cases present with so much variability in onset.
Ultrasonography is the first diagnostic modality, which may suggest heteroechoic cystic masses arising within the uterus, separate from the cavity. 15 One is initially led to think of the more common causes of dysmenorrhea, such as adenomyosis, fibroid with degeneration, endometriomas, or unicornuate uterus with noncommunicating rudimentary horn. 16 As second line of modality, hysterosalpingography, could be performed, which could help differentiate a unicornuate uterus, but MRI is superior and noninvasive.
Being a relatively new entity, there is still a lack of criteria to diagnose ACUMs on MRI. Most of the studies have misdiagnosed ACUMs as another pathology, and very few focus on the features of MRI. Jain and Verma have described how they were able to distinguish ACUMs from obstructed rudimentary horn: both will show cavitated masses lined by endometrium with hemorrhagical contents within, but contralateral tilt of the uterus, banana-shaped small uterine cavity, and a single cornua favors obstructed horn.
15
Acién et al.
7
described the MRI findings as a T1 hyperintense lesion in the left myometrial wall, with a T2 hypointense ring suggestive of hemosiderin deposits. Most recently, Peyron et al.
17
have correlated MRI features with surgicopathological findings in 11 women. Some of the conclusions that can be drawn from this study are:
ACUM is lateralized to the left or right of the uterine cavity, with generally regular borders, generally located under the insertion of round ligament. If categorized according to the FIGO Leiomyoma classification, most of them would be type 5 or 6. The ACUM has a central cavity that is hyperintense on T1. The cavity is surrounded by a ring that has low T1 and T2 signal, which may correspond to the normal junctional zone. Uterine cavity and adnexa are normal.
These points may be useful to standardize the diagnostic criteria of ACUMs, although we may need larger correlation studies. It is important that radiologists, as well as gynecologists be familiar with this condition, to prevent delay in surgical treatment and unnecessary prolongation of the patient's suffering.
Conclusions
Accessory cavitating uterine masses present with severe medically unresponsive dysmenorrhea in young women. All clinicians should be aware of this entity so it can be timely diagnosed and effectively treated by surgical resection and uterine reconstruction.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.