
Abstract
Background:
Dysmenorrhea can be primary or secondary. The causes of secondary dysmenorrhea are uterine and vaginal anomalies, menstrual outflow obstructions, endometriosis, adenomyosis and uterine myomas. This article reports on a patient who had a rare but new entity—an accessory and cavitatory uterine mass (ACUM). A review of literature is also provided. The review was performed through a Medline® for accessory cavitated uterine malformations, juvenile cystic adenomyomas, and uterine-like masses.
Case:
A 30-year-old female presented with chief complaints of chronic pelvic pain and severe dysmenorrhea. She was diagnosed as having rare but new entity known as an accessory and cavitatory uterine mass (ACUM). The mass was removed surgically.
Results:
Case: Histopathology testing of the excised mass revealed that it had a cavity lined with endometrium and surrounded by a muscular layer. The patient's postoperative period was uneventful and her general physical and abdominal condition was normal on discharge. She became totally asymptomatic per close follow-ups for 3 months. Literature search: Sixty-eight cases, including the current case, met inclusion criteria for ACUMs associated with otherwise normal uteri. The average age of women was 25.4 years (range: 14–51 years). The majority had dysmenorrhea or chronic pelvic pain treated elsewhere for many years. All of these patients has their masses excised, and histopathology testing revealed showed that they were cavities lined by endometria and surrounded by muscular layers. Thirty three (48.5%) masses were on the right lateral walls of the uteri adjacent to the round ligaments, 22 (32.3%) were near the attachments of the left round ligaments, 5 (7.3%) were in the broad-ligaments away from the uteri, 3 (4.4%) were subserosal, 2 (2.9%) were in the posterior aspect of the uteri just above the cervices, 1 (1.4%) was on left inguinal subserosal tissue, 1 (1.4%) was on the left anterior wall of the uterus near the uterine artery, and 1 (1.4%) was on the colonic submucosa at the appendiceal foramen.
Conclusions:
ACUM, a rare Müllerian anomaly related to dysfunction of the gubernaculum, should be considered in the differential diagnosis of severe dysmenorrhea and chronic pelvic pain. Magnetic resonance imaging showing an accessory mass, near the attachment of the round ligament, in an otherwise normal uterus with bilateral cornua suggests the diagnosis of ACUM. Excision of the mass is the treatment of choice. ACUM should be considered a newer entity among Müllerian anomalies.
Introduction
Dysmenorrhea is reported in ∼60% females of reproductive age. This condition can be primary (when it is not associated with any pelvic pathology) or secondary (when the condition is associated with uterine and vaginal pathology). Uterine and vaginal anomalies menstrual outflow obstruction, endometriosis, adenomyosis, and uterine myomas are considered in differential diagnoses of secondary dysmenorrhea. 1 An accessory and cavitated uterine mass (ACUM) is a rare, newly recognized, Müllerian anomaly with a cavity lined with functional endometrium in addition to the normal uterine cavity. 2 Most published cases of ACUM, juvenile cystic adenomyoma (JCA), and uterine-like mass (ULM) are actually the same pathology representing new types of Müllerian anomalies. This article reports on a case of a 30-year-old female who presented with chief complaints of chronic pelvic pain and severe dysmenorrhea. She was diagnosed with a rare but new entity—an ACUM. A review of similar cases is included in this article with the goal of increasing awareness of this new entity so it can be diagnosed properly.
The objectives of this report are to:
Raise awareness of ACUM as a new Müllerian anomaly Review the literature from 1912 up to and including the current case in 2020 Emphasize the importance of diagnostic modalities for detecting ACUMs to determine the best surgical treatment Prove that ACUM, JCAs, and ULMs are actually the same pathology, representing new types of Müllerian anomalies Advocate including ACUM among the Müllerian anomalies.
Case and Literature Search
Case
A 30-year-old multiparous female presented with chief complaints of pain in her lower abdomen for 8 years. This pain was confined to the left iliac fossa; and was spasmodic, nonradiating, and was sometimes associated with vomiting. The pain would recur at the completion of her menstruation, lasted for 2–3 days, and gradually increased in intensity and duration. This patient was diagnosed with endometria on the basis of previous investigations. She had been treated at many hospitals with analgesics and oral contraceptives, but her pain was not relieved.
This patient had already undergone magnetic resonance imaging (MRI) that revealed a well-defined, rounded lesion of 2 cm in diameter. The lesion had a hyperdense center with peripheral enhancement that invaded the body of the uterus on the left side. The uterine cavity was deviated to the right side. There was no evidence of any intrauterine lesions. The bilateral adnexa and ovaries appeared to be normal (Fig 1). These findings were suggestive of either endometria, a rudimentary horn, or a degenerated fibroid. On the basis of these findings and the fact that this patient had not obtained relief of her chronic pelvic pain, she underwent surgery.
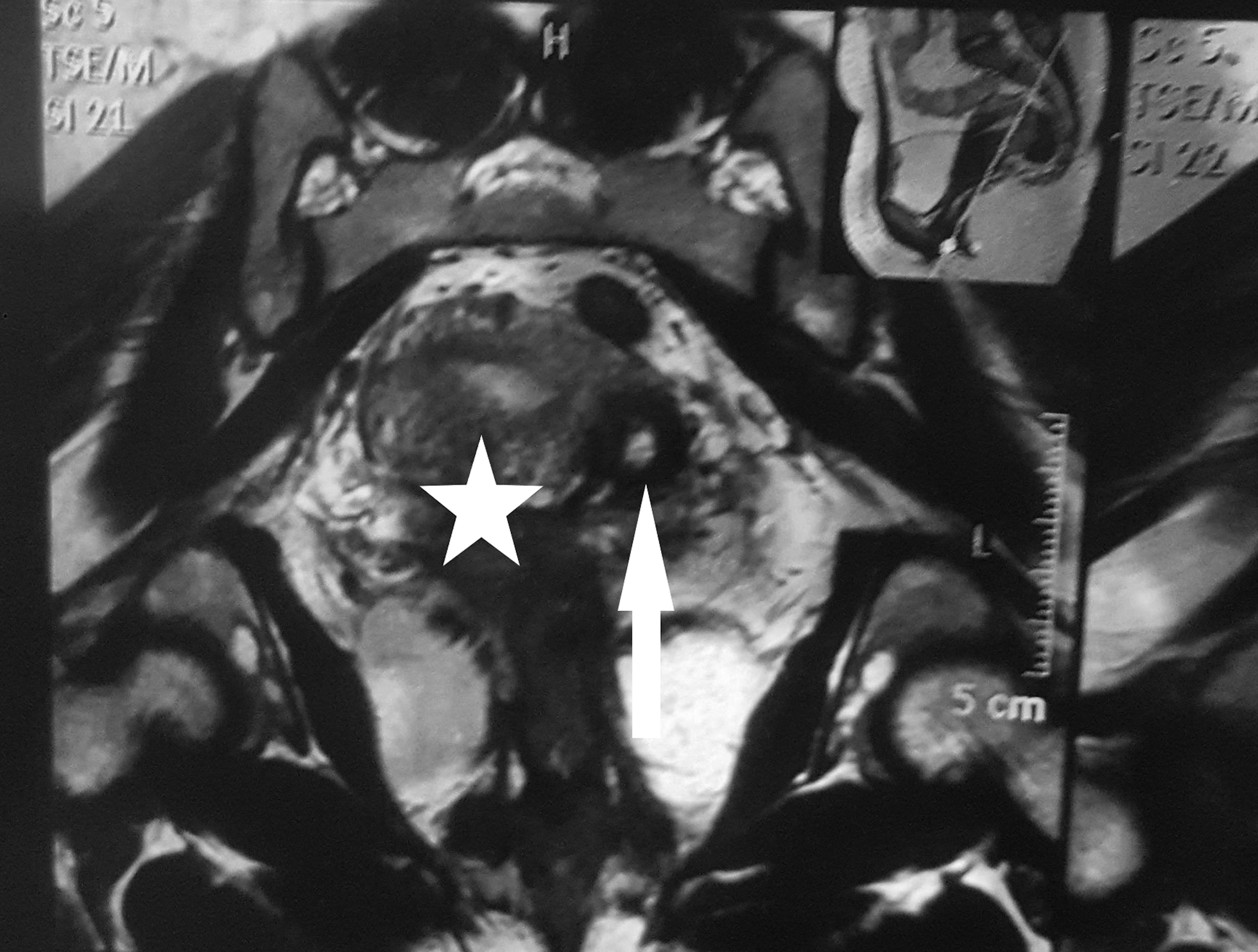
Magnetic resonance imaging reveals accessory cavitated mass (arrow) adjacent to a normal uterus showing two cornu (star).
On laparoscopy, a rounded lesion of 3 × 3 cm was seen near the left cornu of the uterus just below and lateral to the attachment of the round ligament. The uterus was slightly deviated to the right side. The bilateral tubes and ovaries were normal. There was no evidence of any sign of endometriosis.
On hysteroscopy, both ostia were simultaneously visible. Thus, the existence of a rudimentary horn was ruled out. She underwent a laparotomy with a differential diagnosis of a degenerated fibroid and endometrioma. Vasopressin was injected over the lesion. Enucleation of the mass was performed with dead space obliteration (Figs. 2 and 3). A cut section of the mass showed a cavitatory lesion containing chocolate-colored fluid (Fig. 4). The excised mass was sent for histopathologic examination.

Excision of cavitated mass.

Obliteration of dead space after excision.

Cut section of excised mass.
Literature search
A review of the literature was performed through a Medline® search looking for accessory cavitated uterine malformations, juvenile cystic adenomyomas, and uterine-like masses. Table 1 lists enumerates the cases published in the literature.2–34 The current case is also included in the table.
Published Cases of ACUM, JCA, and ULM
ACUM, accessory and cavitated uterine mass; JCA, juvenile cystic adenomyoma, ULM, uterine-like masses; yrs, years.
The criteria used to include a case were:
Isolated accessory cavitated mass, usually located under the round ligament Normal uterus, fallopian tubes, and ovaries Surgery performed with pathologic examination of the excised mass Accessory cavity lined by endometrial epithelium with glands and stroma Chocolate–brown-colored fluid contents No adenomyosis in the uterus (if resected), although sometimes tiny foci of adenomysis in the myometrium of accessory cavity can be present.
3
Results
Case results
This patient's postoperative period was uneventful. Her general physical and abdominal condition was normal at the time of her discharge. She became totally asymptomatic as noted by close follow-ups for 3 months.
Histopathologic examination of the excised tissue revealed that it was a cavitated mass lined by functional endometrium with irregularly arranged smooth-muscle cells (Fig. 5).

Photomicrograph showing a cavity lined by endometrial glands and smooth-muscle cells.
Literature search results
As shown in Table 1,2–34 there were 68 reported cases—including the 1 case reported in this article—that met the inclusion criteria listed for ACUMs associated with otherwise normal uteri. The average age of these women was 25.4 years (range: ages 14–51). The youngest was age 14 and the eldest was age 51. The majority of these women had presented with dysmenorrhea or chronic pelvic pain that had been treated elsewhere for many years. All of these patients underwent surgery and histopathology testing in each case revealed a cystic adenoma-like mass with a cavity lined by endometrium and surrounded by a muscular layer.
These cases were reported as being congenital or adenomyotic cysts of the uteri or ULMs located at various sites in the pelvis, attached or not to the uterus. Thirty-three masses (48.5%) were found on the right lateral walls of the uteri adjacent to the round ligaments, 22 (32.3%) were found near the attachments of the left round ligaments, 5 (7.3%) were found in the broad ligaments away from the uteri, 3 (4.4%) were subserosal, 2 (2.9%) were found in the posterior aspects of the uteri just above the cervices, 1 (1.4%) was found on left inguinal subserosal tissue, 1 (1.4%) was found on the left anterior wall of the uterus near the uterine artery, and 1 (1.4%) was found on colonic submucosa at the appendiceal foramen.
Discussion
An ACUM is a rare newly recognized, Müllerian anomaly. It is an accessory cavity lined with functional endometrium in addition to a normal uterine cavity. An ACUM is a cavitated mass confined to the myometrium; is encapsulated; and has uterus-like histologic organization. 2 The ACUM is lined by endometrial glands and stroma, and is surrounded by irregularly arranged smooth-muscle cells that show positivity for estrogen receptors and progesterone receptors, resembling myometrium. 3 The ACUM has both a macroscopic and microscopic resemblance to the uterus and can arise anywhere and beyond the uterus in a patient of any age. Associations with genitourinary and gastrointestinal anomalies have been described. The most-common extrauterine sites are the ovary, broad ligament, bowel mesentery, appendix, colon, conus medullaris, and uterosacral ligament.
There are three theories explaining the development of ACUM: (1) congenital anomaly; (2) heterotopias; and (3) metaplasia. Most of the authors of the reports considered ACUM to be a congenital anomaly. The proposed mechanism is that ACUM might be possibly related to gubernaculum dysfunction. 35 An accessory mass could be caused by duplication of a ductal Müllerian mass in a critical area at the level of attachment of the round ligament.
As described in the current case report and analysis of published cases shown in Table 1,2–34 ACUMs, JCAs, and ULMs have same pathology. The condition usually presents in young women with chronic pelvic pain, severe dysmenorrhea, and abdominal cramps that are resistant to medication. In this review, the majority of the women presented with these symptoms. The youngest female in the review was 14, described by Acien et al., 3 presented with severe dysmenorrhea. Liu et al. described a case of an ULM in a 51-year-old female with a lesion measuring 6 × 7 in the right broad ligament. 32
To fulfill the criteria for ACUM, a normal uterus, and normal fallopian tubes and ovaries must be present. Acién et al. 3 and Ahmed et al. 36 each described 1 case of ACUM that had an additional rudimentary fallopian tube attached to the ACUM. Acien et al. described a case of ULM that presented with a rudimentary horn with a third fallopian tube and the characteristics of a duplication of a right Müllerian duct. 3
Repich et al. reported a pregnancy in an accessory uterine cavity in 32-year-old married female who presented with a 4-year history of cystic pain not relieved with oral contraceptive pills. 26 She was diagnosed with that accessory cavity on sonography and a hysterosalpingogram. There was hemorrhagic content in the accessory cavity and this patient's β-human chorionic gonadotropin level was raised. Excision of the accessory cavity was performed, and, on histopathology testing, chorionic villi were seen implanted in a muscular wall. Repich et al. concluded that microcommunication might have existed between the two cavities. 26
Alkhateeb and Yaseen described a missed pregnancy of 13 weeks in an ACUM located on the right side of the uterus. 28 There were three unsuccessful attempts of curettage noted on sonography after evacuation. Iatrogenic perforation occurred on the third attempt and immediate exploration revealed the perforation, which was stitched, and the ACUM carrying the missed sac was removed.
Na et al. 24 reported an ULM located in the colonic submucosa in a 39-year-old female presenting with continuous abdominal pain. She had undergone hysterectomy 2 years prior. Computed tomography of her abdomen and pelvis showed a dumbbell-shaped luminal mass in the caecum. She was managed with a cecoctomy and left hemicolectomy and her case was proven to be an ACUM on histopathology and immunohistochemistry testing.
Kaufman and Lam reported a pelvic ULM in a female 20 years after a hysterectomy and bilateral salpingo-opherectomy. 37
Rougier et al. 38 and Sharma et al. 39 reported ULMs in the spinal cords of patients with spina bifida. These authors suggested that heterotopic Müllerian tissue within a neural tube can result in an ULM.
For diagnosis, sonography is the initial modality that can identify a mass as a solid isoechoic mass resembling endometrium arising within the uterus and ovaries, and visualized separately from the ovaries, when a patient presents with dysmenorrhea. Hysterosalpingography will reveals a normal uterine cavity and fallopian tubes, thus, ruling out a Müllerian anomaly. MRI is the investigation of choice. It shows pelvic anatomy clearly, a cavitated mass with hemorrhagic contents, the uterus, and the myometrial and endometrial interface. Great experience is required to diagnose the condition. In the current patient, too, the initial diagnosis was endometria and a rudimentary horn which were ruled out after surgery.
Peyron et al. described MRI features of an ACUM and correlated them with surgical findings in haemen. 33 All 7 lesions were well-correlated with surgical findings, lateralized (7 were left sided), and located under the horns and round-ligament insertions. Nine were located within external myometrium, bulging into the broad ligaments. Two were extrauterine, entirely located within the broad ligaments. The author concluded that MRI facilitates timely diagnosis and appropriate fertility-sparing laparoscopic resection. 33
He et al. reported a lesion in a 43-year-old female presenting with acute lower abdominal pain. 40 Sonography revealed a 7 × 4–cm irregular mass on the left side of the uterus. The mass was removed via laparotomy, based on a preoperative diagnosis of ovarian torsion. The excised mass revealed features of an ULM that was confirmed by the positioning of estrogen and progesterone receptors.
The best therapeutic approach is tumorectomy, which can be performed laparoscopically. However, laparotomy is preferred especially when the mass is located on the lateral wall of the uterus. An appropriate site for making the incision should be chosen to excise the lesion completely.
Hysterectomy may even be a choice for patients who have completed their families.
Conclusions
The diagnosis of ACUM should always be considered in clinical suspicious case of dysmenorrhea. Transvaginal sonography and MRI are helpful for making the correct diagnosis. Early surgical treatment via laparoscopy or laparotomy will prevent typical suffering in these women. ACUM should be included as newer entity among Müllerian-anomaly classifications.
Footnotes
Acknowledgments
Dr. Malhotra operated on the patient and played a crucial role in writing this article. Dr. Dahiya collected data, Drs. Nanda and Chauhan edited the article, and Dr. Bhuria edited the figures.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this article.