
Abstract
Background:
Uterine volvulus is a rare occurrence, especially in non-gravid uteri. Uterine volvulus can lead to ischemia and necrosis when left undetected.
Case:
A 73-year-old woman with acute abdominal pain and known history of fibroid uterus underwent an exploratory laparotomy showing a uterine volvulus, which resulted in uterine and adnexal necrosis.
Results:
The patient's pain, which was secondary to torsion of her uterus, resolved after hysterectomy and bilateral salpingo-oophorectomy.
Conclusion:
Uterine volvulus, although rare, is a gynecological emergency that should be detected quickly to prevent severe morbidity and to conserve fertility in reproductive-age women.
Introduction
The term volvulus is used to refer to the abnormal twisting of an organ on itself, generally referring to the intestines; however, this term can also be applied to the abnormal twisting, or torsion of the uterus. The definition of uterine torsion, or volvulus, has generally been accepted as the rotation of the uterus on its long axis of at least 45° and the most common anatomic site for this to occur is at the uterine isthmus.1,2 Volvulus of any organ can lead to impaired blood flow and subsequent necrosis of that organ, making it important to make a timely diagnosis. Uterine volvulus is part of a spectrum of gynecological emergencies; if diagnosis is not made quickly and treatment is delayed, severe consequences such as infertility, loss of one's uterus, and even life-threatening complications can arise. 3 Thus, uterine volvulus, or torsion, should be included in the differential in women who present with severe abdominal pain, large uterine fibroids, or cessation of menstruation in pre-menopausal women. 2
Uterine torsion is rare overall, with the first case being reported in 1909; until 1992, only a total of 212 cases had been reported in the literature with less than a quarter of those cases taking place in a non-gravid uterus.2–4 The reason it is rare is because the uterus is generally fixed in place in the pelvis secondary to its ligamentous attachments. 2 When uterine volvulus does occur, it is most commonly seen in pregnancy (especially when fetal malpresentation is present); however, other important predisposing factors include large uterine fibroids, congenital uterine anomalies (most commonly bicornuate uterus), pelvic adhesions, and adnexal masses.2,3,5–7 It has been quoted that abnormal fetal presentation causes 23% of uterine torsions and uterine fibroids cause 21%. 1 The following is a case presentation of a uterine volvulus diagnosed intraoperatively due to a large non-gravid fibroid uterus.
Case Description
This is a 73-year-old, gravida zero, postmenopausal woman with a past medical history significant for chronic lymphocytic leukemia, B cell lymphoma, heart failure with preserved ejection fraction, and gastric arteriovenous malformations who presented to the emergency room with a complaint of acute onset abdominal pain, constipation, and urinary retention. In the emergency room, the patient was noted to have a hemoglobin of 6.0 g/dL and a transfusion of 2 U of packed red blood cells was initiated. The patient underwent portable abdominal X-ray, which was significant for dilated loops of bowel, possible ileus versus obstruction, and a fibroid obscuring the left lower quadrant. She then underwent a computed tomography (CT) abdomen and pelvis with contrast, which was significant for no bowel obstruction; retroperitoneal lymphadenopathy, which was improved compared with a prior study; mild right hydronephrosis, which was new compared with a prior study; distended gallbladder; an enlarged uterus that contained multiple enlarged and calcified fibroids; and a small amount of ascites. The patient was admitted to the internal medicine service for the management of her anemia, constipation, and pain. On hospital day 2, the patient underwent consultation with the gastroenterology service who recommended continued bowel regimen for constipation with plan to do a colonoscopy. The patient's abdominal pain did not improve despite pain medication and on hospital day 3 the general surgery service was consulted and their recommendation was to contact the gynecological team for evaluation of her fibroid uterus.
On the evening of hospital day 3, the gynecological service was consulted and examination of the patient was significant for a diffusely tender abdomen to palpation with voluntary guarding but no rebound tenderness and a palpable 30-week-sized fibroid uterus. The patient was also noted to have worsening urinary retention, which was suspected to be secondary to mass effect from her enlarged fibroid uterus; a foley catheter was inserted at this time which drained clear urine. Surgical management via exploratory laparotomy and hysterectomy was discussed with the patient secondary to her uncontrolled pain despite oral medications and urinary retention and she expressed desire for this definitive plan of management. On hospital day 4, the patient was taken to the operating room for an exploratory laparotomy. The abdomen was entered via a Maylard incision. On entering the abdominal cavity, a large calcified pedunculated and necrotic fundal fibroid was identified and a 360-degree volvulus of the uterus was noted on its sagittal axis. The uterus was detorsed to restore anatomy (Fig. 2). The uterus was edematous and had multiple calcified and necrotic fibroids; the adnexa were edematous and necrotic bilaterally. Total abdominal hysterectomy and bilateral salpingo-oophorectomy was completed in the normal fashion, and specimens were sent to pathology. Due to the edematous and distorted nature of the patient's anatomy, the ureters could not be definitely identified and so flexible cystoscopy was performed, which showed normal appearing bladder mucosa and bilateral ureteral jets. The patient's abdomen was then closed in the normal fashion. The patient did well postoperatively and was discharged home on postoperative day 4. Surgical pathology was significant for the uterus that weighed 1864 g and “leiomyoma, subserosal and intramural, extensively calcified; Unremarkable endocervix (exocervix not identified), necrotic and hemorrhagic structure suggestive of a fallopian tube, and adherent fibroadipose tissue with fibrosis and fat necrosis in the region of the adnexa.”
Discussion
The literature has demonstrated that a large fibroid, especially a subserosal fundal fibroid, can rotate and cause traction on the uterus, subsequently causing torsion. 2 Torsion of the uterus can be either acute or chronic; chronic torsion more commonly causes longstanding abdominal pain, whereas acute torsion causes new-onset severe abdominal pain. 2 Our patient presented to the emergency room with new onset abdominal pain, likely pointing to a more acute onset volvulus of the uterus. Uterine volvulus can have many different clinical presentations ranging from acute or chronic abdominal pain to shock and hemorrhage; other findings associated with this diagnosis are vaginal spotting or bleeding, uterine tenderness, vaginal tenderness, or cranial traction of the cervix and twisting of the vaginal canal on pelvic exam. 5 Our patient denied episodes of vaginal bleeding or spotting but she did have exquisite tenderness when a vaginal exam was attempted initially; however, the exam in the operating room under anesthesia did not reveal a twisted vaginal canal.
Increased cervical length can cause distortion of the uterine isthmus and increase the risk for uterine torsion; a study using magnetic resonance imaging (MRI) in women who underwent cesarean deliveries showed that poor healing of the uterine isthmus was related to abnormal cervical lengths, which can result in an elongated cervix with structural weakness and angulation in the isthmic region and may predispose to torsion of the uterus. 8 Although our patient had never been pregnant nor undergone any cesarean deliveries, we suspect that the weight of the enlarged calcified fibroid uterus caused tension on and weakening of the uterine isthmus and stretching of the cervix, which collectively predisposed her to uterine volvulus.
One of the most important factors in diagnosing a uterine volvulus quickly is that if the blood supply is compromised eventual infarction and necrosis cannot be avoided. Since this diagnosis is rarely made, it is not well documented in the literature of what the time period or degree of rotation is in which ischemic changes become irreversible. 6 In the pediatric population, it has been shown that torsion >60° causes irreversible ischemia of the uterus. 9 This concern is especially important in women of reproductive age who desire fertility. The mainstay of treatment is surgery for this condition. Our patient underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy; however, in women who desire future fertility, myomectomy and detorsion of the uterus can be considered if the uterus and adnexa are still deemed to be viable. 3 It has also been suggested that an option in fertility-sparing approaches with detorsion and myomectomy when necrosis is not evident is bilateral plication of the round or uterosacral ligaments to prevent recurrence of uterine torsion. 6
Since the goal of treatment is to avoid ischemia and necrosis of the uterus, diagnosis needs to be made quickly. There is a role for diagnosis on imaging, especially CT, since this is the most common imaging modality used when a patient presents to the emergency department with symptoms of acute abdominal pain.3,10 It has been well documented that on CT imaging volvulus, or uterine torsion, can present as a whorled structure representing the twisted uterine cervix, similar to having evidence of a “whirlpool sign” that is commonly seen on imaging of a bowel volvulus.1,3,5,6
Before taking our patient to the operating room, the diagnosis was not suspected based on imaging but when retrospectively viewing her CT scan there were possible “whorled” images of the uterus and cervix that could have helped make the diagnosis pre-operatively (Fig. 1C). Another possible diagnostic clue on imaging, on either CT scan or plain radiographs, is gas in the uterine cavity that can represent necrosis of the uterine wall secondary to ischemia caused by prolonged rotation. 11 If a pelvic ultrasound is done during initial workup, torsion of a myomatous uterus may be suspected if fibroids noted on previous ultrasound scans are seen to have changed position. 11 The diagnosis can also be suspected if MRI is able to be used and shows the presence of an X-shaped configuration of the vagina, because usually the vagina appears H shaped on MRI. 12
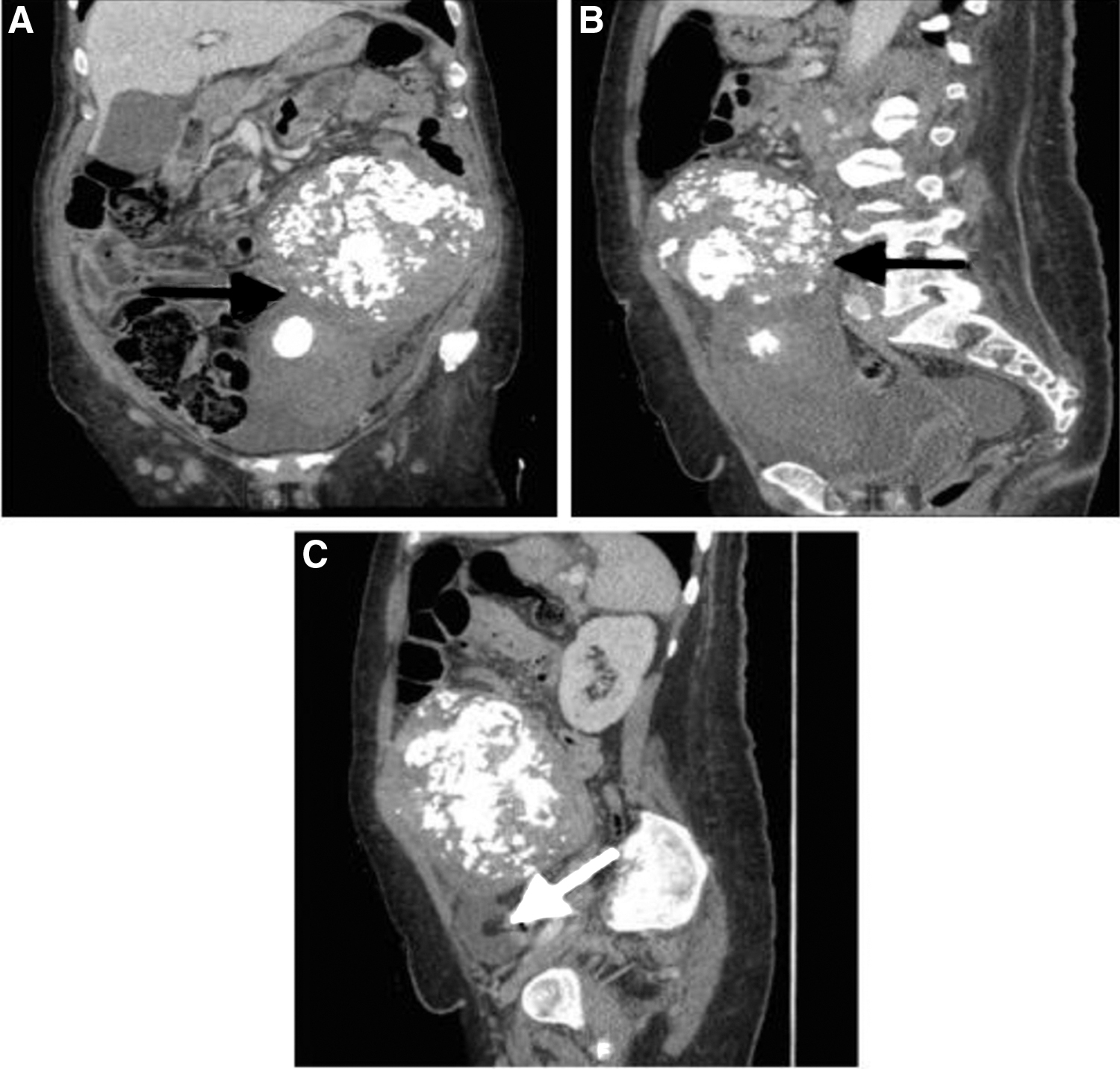
Computed tomography abdomen and pelvis with contrast.

Intraoperative images.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.