
Abstract
Objective:
The purpose of this study is to present a case series of surgeries performed for patients with distorted cervical anatomy and suspected cervical and/or endometrial pathology. Currently, there are no guidelines for management of these patients.
Design:
This study is a retrospective case series reviewing patients at Moffitt Cancer Center from September 1, 2016, to January 31, 2020.
Materials and Methods:
Patients with distorted cervical anatomy who underwent surgery for suspected cervical or endometrial pathology were identified. Data were collected for each patient including demographics, preoperative clinical examination, intraoperative characteristics, postoperative complications, and final pathology.
Results:
In this study, 21 patients were included and 20 of them were managed with hysterectomy. On final pathology, three patients (14%) were diagnosed with malignancy. Nine patients (43%) were found to have noninvasive disease on final pathology.
Conclusion:
In patients with distorted cervical anatomy and potential pathology, hysterectomy should be considered.
Introduction
Distorted cervical anatomy including stenosis, scarring, or obliteration limits cervical and endometrial evaluation in patients with a history of cervical dysplasia or concern for cervical or endometrial pathology. The distorted anatomy may be secondary to a prior cervical procedure, infection, diethylstilbestrol exposure, or atrophic menopausal changes.1–6
Anatomic changes may lead to inadequate colposcopy 7 and/or the inability to perform an endocervical curettage, or endometrial sampling. Given that most cervical neoplasia is located within the transformation zone, cervical scarring, cervical stenosis, and inadequate colposcopy can result in unrecognized lesions. 8 Cervical stenosis is also a common factor associated with failed endometrial sampling. 9 The true incidence of cervical stenosis is unknown, but in one series of 31,052 office hysteroscopies, cervical stenosis was found in 32.7% of patients.1,4 Distorted cervical anatomy poses challenges in the diagnosis of both cervical and endometrial neoplasia as described, and limits options for management of cervical neoplasia. The safety of clinical and cytological surveillance in this specific population of patients is unknown.
Currently, there are no recommendations or guidelines for management of patients with distorted cervical anatomy and potential cervical or endometrial pathology. In the gynecology oncology department at Moffitt Cancer Center, we see patients who have been referred specifically because their cervix and/or endometrium could not be adequately evaluated due to distorted cervical anatomy.
The purpose of this study is to present a case series of surgeries performed for the management of patients with suspected cervical or endometrial neoplasia complicated by a distorted and inevaluable cervix.
Design, Materials, and Methods
This study is a retrospective case series reviewing patients at Moffitt Cancer Center from September 1, 2016, to January 31, 2020. The Institutional Review Board at Moffitt Cancer Center approved this study. Patients were selected if they underwent surgery at Moffitt Cancer Center for a suspicion of cervical or endometrial neoplasia complicated by distorted cervical anatomy. We were unable to identify the cohort of patients referred with a distorted cervix who did not undergo subsequent surgery.
We define severe cervical stenosis as the inability to pass a Cytobrush (Cooper Surgical) beyond the external os. Obliteration of the os was similarly defined but included lack of any visible opening. An otherwise distorted cervix was defined subjectively as complete or almost complete lack of identifiable exocervix.
Data abstracted from electronic chart review included patient demographics and medical history. Prior treatment for cervical dysplasia, surgical history, the results of recent cervical cytology, the results of any imaging of concern (thickened endometrium, etc.), and attempts at diagnosis of cervical or endometrial neoplasia were recorded. Physical examination findings specifically related to the patient's cervical anatomy were noted. Information on the surgery performed, operative time, estimated blood loss (EBL), postoperative complications, and final pathology were included.
Results
There were 21 patients with a distorted cervix who underwent surgical management. Two other such patients planned for surgery were lost to follow-up before operation. Patient demographics are noted in Table 1. The mean age of the patients was 55.8 years (range: 38–69). Eighty-one percent of patients were postmenopausal and 10% were perimenopausal. The mean body mass index (BMI) was 31.7 kg/m2 (range: 20–47). The mean parity was 1.52 and 24% of patients were nulliparous. Twenty-nine percent of patients had underlying major medical comorbidities, including coronary artery disease, chronic obstructive sleep apnea, congestive heart failure, diabetes, hypertension, and rheumatoid arthritis.
History and Perioperative Outcomes of Patients Undergoing Surgery with Distorted Cervix
BS, bilateral salpingectomy; BSO, bilateral salpingo-oophorectomy; BTL, bilateral tubal ligation; Bx, biopsy; CAD, coronary artery disease; CIN, cervical intraepithelial neoplasia; CKC, cold knife conization; D&C, dilation and curettage; EBL, estimated blood loss; ECC, endocervical curettage; HGSIL, high-grade squamous epithelial lesion; LEEP, loop electrosurgical excision procedure; LGSIL, low-grade squamous epithelial lesion; LOS, length of stay; PLND, pelvic lymph node dissection; PMB, postmenopausal bleeding; PPLND, pelvic and para-aortic lymph node dissection; RA, robotic assisted; TLH, total laparoscopic hysterectomy; TVH, total vaginal hysterectomy.
Fifteen of 21 patients underwent prior cervical procedures including cold knife conization, loop electrosurgical excisional procedure, and cervical cryotherapy and 38% of patients underwent more than one prior procedure. Findings on cervical examination are noted in Table 2, and included severe cervical stenosis, obliterated or nonvisible cervical os, small or absent exocervix, and fornices flush with the vagina.
Cervical Examination Findings
In this study, 20 of the 21 patients were managed with hysterectomy. One patient previously underwent supracervical hysterectomy, and a robotically assisted trachelectomy was performed. Routes of hysterectomy were vaginal (13), laparoscopic (5), and robotic (2). Intra-operative and post-operative findings are noted in Table 3. The mean operative time for the 13 vaginal hysterectomies was 57.1 minutes (range: 40–90 minutes) and that for laparoscopic hysterectomy was 125 minutes (range: 90–180 minutes). EBL for all cases ranged from minimal to 100 mL. The complication rate was 14% (3 out of 21 patients). Two patients had intraoperative urinary tract injuries (one cystotomy and one left ureteral transection), both of which were detected and repaired at the time of the initial surgery. One patient subsequently developed a vesicovaginal fistula. Average length of stay was 0.29 days. Fifteen out of 21 patients were discharged home on the day of surgery.
Intraoperative and Postoperative Findings
OR, operating room; TLH, total laparoscopic hysterectomy; TVH, total vaginal hysterectomy.
Before definitive surgical management, 43% of patients had biopsy-proven neoplasia (of these, 81% had an unsatisfactory colposcopy and 71% were unable to undergo endocervical curettage due to stenosis). On final pathology, three patients (14%) were diagnosed with malignancy (Fig. 1). Three patients had endometrial cancer (stage 1A, FIGO grade 1, stage 1A, FIGO grade 2, and one patient had at least stage 1B, FIGO grade 2). Nine patients (43%) were found to have noninvasive disease on final pathology (Fig. 2). Five patients had CIN 1, three patients had CIN 2/3, and one patient had complex endometrial hyperplasia without atypia. Nine patients (43%) had no evidence of neoplasia (Table 4). Figures 3–5 are intra-operative photos from one case included in this case series.
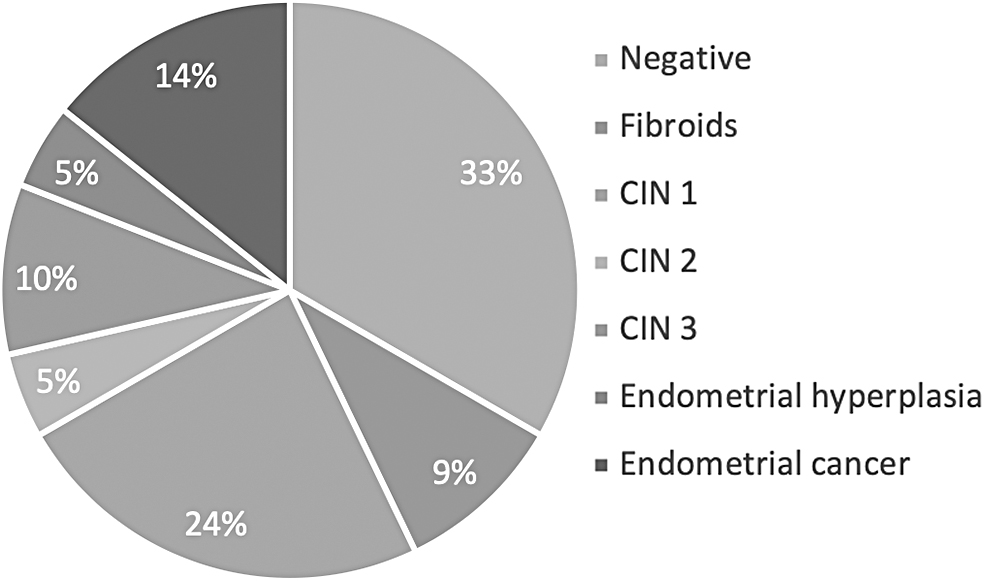
Final pathology in patients undergoing hysterectomy with distorted cervical anatomy.
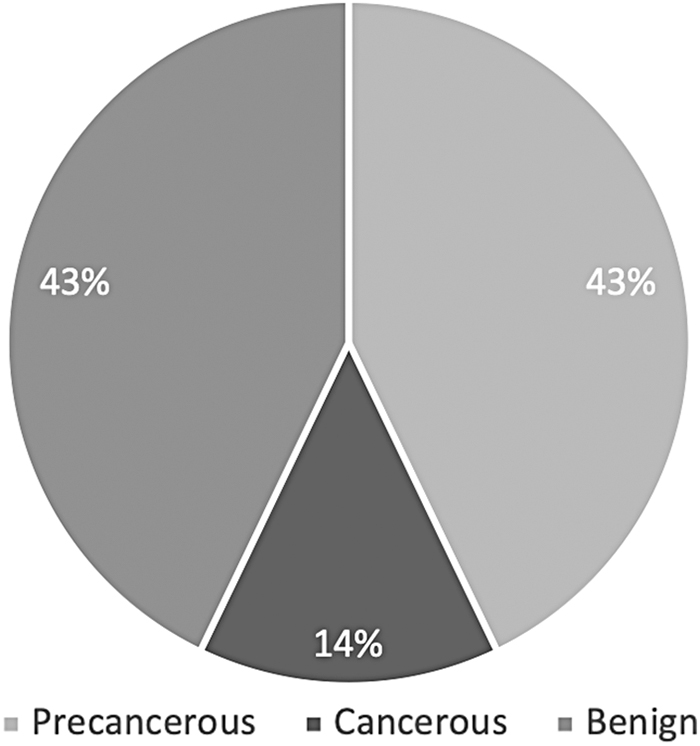
Percentage of patients with precancerous, cancerous, and benign pathology.
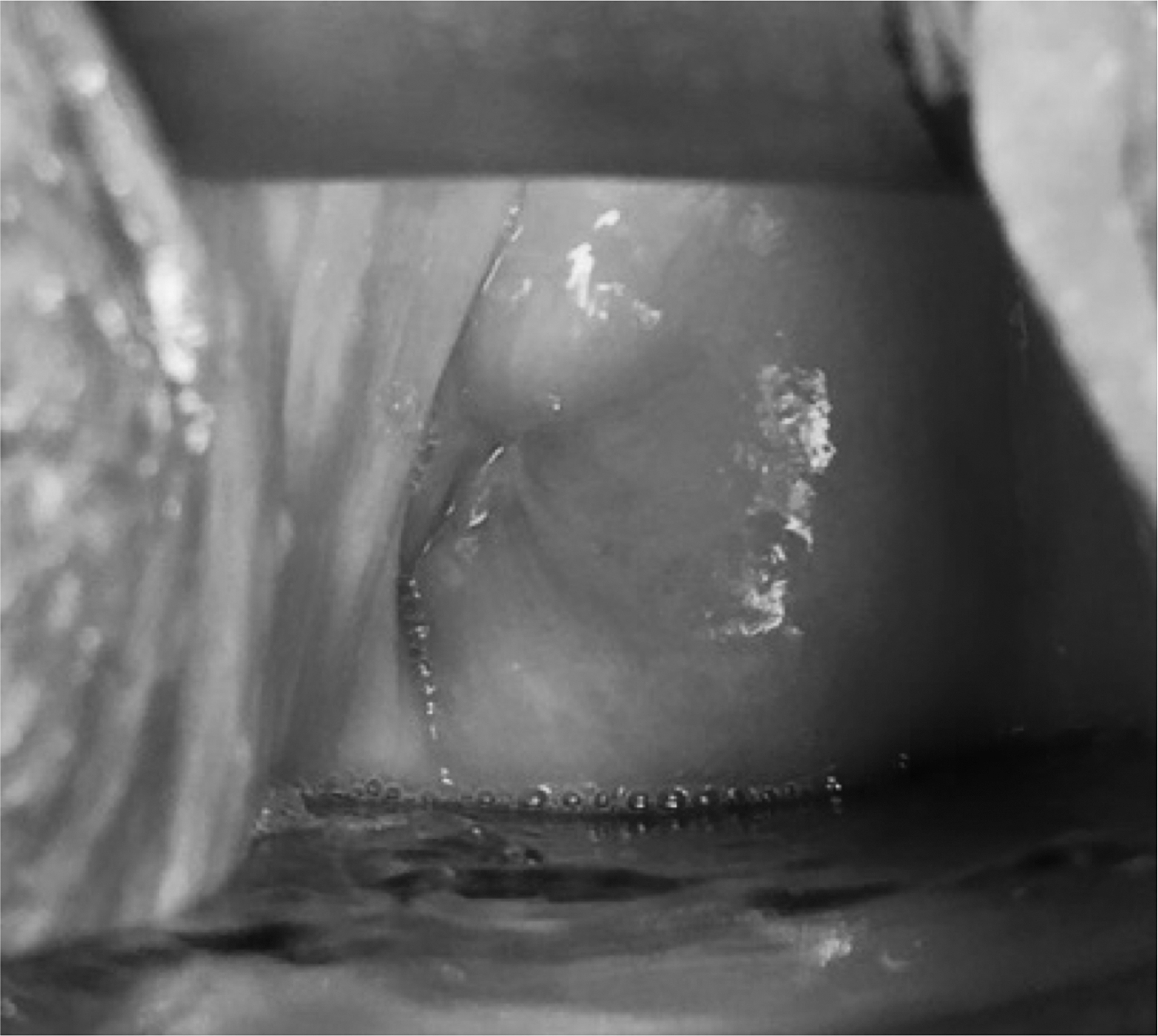
Exocervix with cervical stenosis.

Uterus and distorted cervix status posthysterectomy.

External cervical os.
Final Pathology
CIN, cervical intraepithelial neoplasia.
Conclusion
The vast majority of women who fall within the guidelines for routine cervical screening are adequately sampled with an Ayer's spatula and endocervical brush (or similar devices). However, in the presence of marked cervical distortion and, especially, severe stenosis or obliteration of the canal, sampling error is a distinct possibility. This is of particular concern in women with a history or even current evidence of cervical neoplasia. Further attempts at sampling or even resolving stenosis have been described, but they are not definitive and may be impractical or limited by anatomy.1,2 Our management of choice in such patients who are fit for surgery is, therefore, hysterectomy. The pathological findings in this study support this approach. Concerns with proceeding directly to hysterectomy included the possibility of occult invasive cervical cancer and complications of surgery. Surgical challenges in these women include loss of some anatomic landmarks when proceeding vaginally and placement of a uterine manipulator. The high rate of urinary tract injury in the present series is likely a consequence, and raises a note of caution when proceeding to hysterectomy in such patients.
The vast majority of women who have findings suspicious for endometrial neoplasia (postmenopausal bleeding and thickened endometrium) will be adequately evaluated with office or operating room endometrial sampling. Cervical stenosis in such patients is generally easily surmounted in the operating room (if not the office).1,4 However, if sampling is not anatomically possible for the reasons described, hysterectomy is a reasonable consideration for operable women. The current series supports this contention. The vaginal route was deemed appropriate given a combination of factors, including a less invasive procedure relative to the lack of a definitive diagnosis and comorbidities (including BMI). 10
In conclusion, for women with suspected cervical or endometrial neoplasia and the inability to undergo adequate evaluation due to cervical distortion as described, hysterectomy should be considered. Such cases may be associated with an elevated operative risk of urinary tract injury.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.