
Abstract
Background:
Interstitial ectopic pregnancy comprises 1%–2% of all ectopic gestations but carries 7 times more mortality than other ectopic pregnancies. An interstitial pregnancy has the potential to cause massive hemorrhaging at any time during early pregnancy, making early recognition and treatment crucial.
Case:
A 41-year-old parous woman had a pan mural calcified fibroid in close proximity to an ectopic pregnancy; she desired to have future fertility after treatment. Laparoscopic linear cornuostomy, followed by a right salpingectomy and a myomectomy, was performed.
Results:
Various etiologies have been described in the literature, including previous, ectopic in-vitro fertilization; pelvic inflammatory disease; and previous ipsilateral salpingectomy, but in the current case, the presence of the pan mural fibroid in close proximity to the tubal ostium was considered to be the plausible cause for this interstitial ectopic pregnancy, per histopathologic examination of the specimens. This patient's ß–human chorionic gonadotropin level became negative at 3 weeks post surgery.
Conclusions:
Compared to a cornuectomy, a laparoscopic cornuostomy, with a salpingectomy and a concurrent myomectomy, is a safe and feasible option, considering a patient's desire for future fertility and her lower risk of uterine rupture.
Introduction
Interstitial ectopic pregnancy comprises 1%–2% of all ectopic gestations but causes 7 times more mortality than other ectopic pregnancies. 1 An interstitial pregnancy can potentially cause massive hemorrhaging at any time during early pregnancy. Thus, early recognition and treatment crucial.
Case
A 41-year-old woman (gravida 4, para 1, live 1, abortions 2) was referred to a gynecology emergency department at 7 + 1 weeks' period of gestation (POG). She had an ultrasound (US) report that she had a right interstitial ectopic pregnancy. She had irregular bleeding intermittently that had started 1 month prior. She had history of 1 cesarean section 13 years ago, followed by 2 abortions, which required dilatation and curettage. A general physical examination showed that this patient was hemodynamically stable with no pallor, and her vitals were stable, with a pulse of 88 beats/minute and a blood pressure of 110/70 mm Hg. An abdominal examination revealed that her uterus was just palpable. A bimanual examination revealed a nulliparous os with a uterus size of 14 weeks.
The US report that she brought with her showed that there was an echogenic lesion measuring 36 × 36 mm, with high vascularity bulging from the right lateral wall with an overlying thin myometrium. This was suggestive of a right interstitial ectopic pregnancy. The cavity was empty, with an old calcified fibroid, of size 45 × 38 mm, in the right lateral wall (Fig. 1).

A transvaginal scan of the pelvis revealed an echogenic lesion, measuring 36 × 36 mm bulging from right the right lateral uterine wall with an overlying thin myometrium. This was suggestive of a right interstitial ectopic pregnancy. The cavity was empty with an old calcified fibroid, of size 45 × 38 mm, in the right lateral wall. On color doppler, the increased vascularity was visualized. Color images are available online.
Her ß–human chorionic gonadotropin (ß-hCG) on admission was >10,000 international units/mL. The management options were explained to her, and she chose the surgical route. She was admitted to the hospital and evaluated with detailed magnetic resonance imaging (MRI) of her pelvis; this MRI revealed a round heterogeneous T1, hyperintense lesion, measuring 3.5 × 4.7 × 3.3 cm, with a T2 hyperintense, vascular peripheral rim and central cystic area. This appearance was suggestive of a right interstitial ectopic pregnancy with an overlying thin myometrium. (Fig. 2). No fetal pole was visualized. There was also a 4.5 × 3.9 × 3.7–cm intramural fibroid, with peripheral calcification, in the right antero-lateral uterine wall, inferior to the ectopic pregnancy. Her routine blood investigations yielded normal results, with a hemoglobin level of 10.8 g/dL.
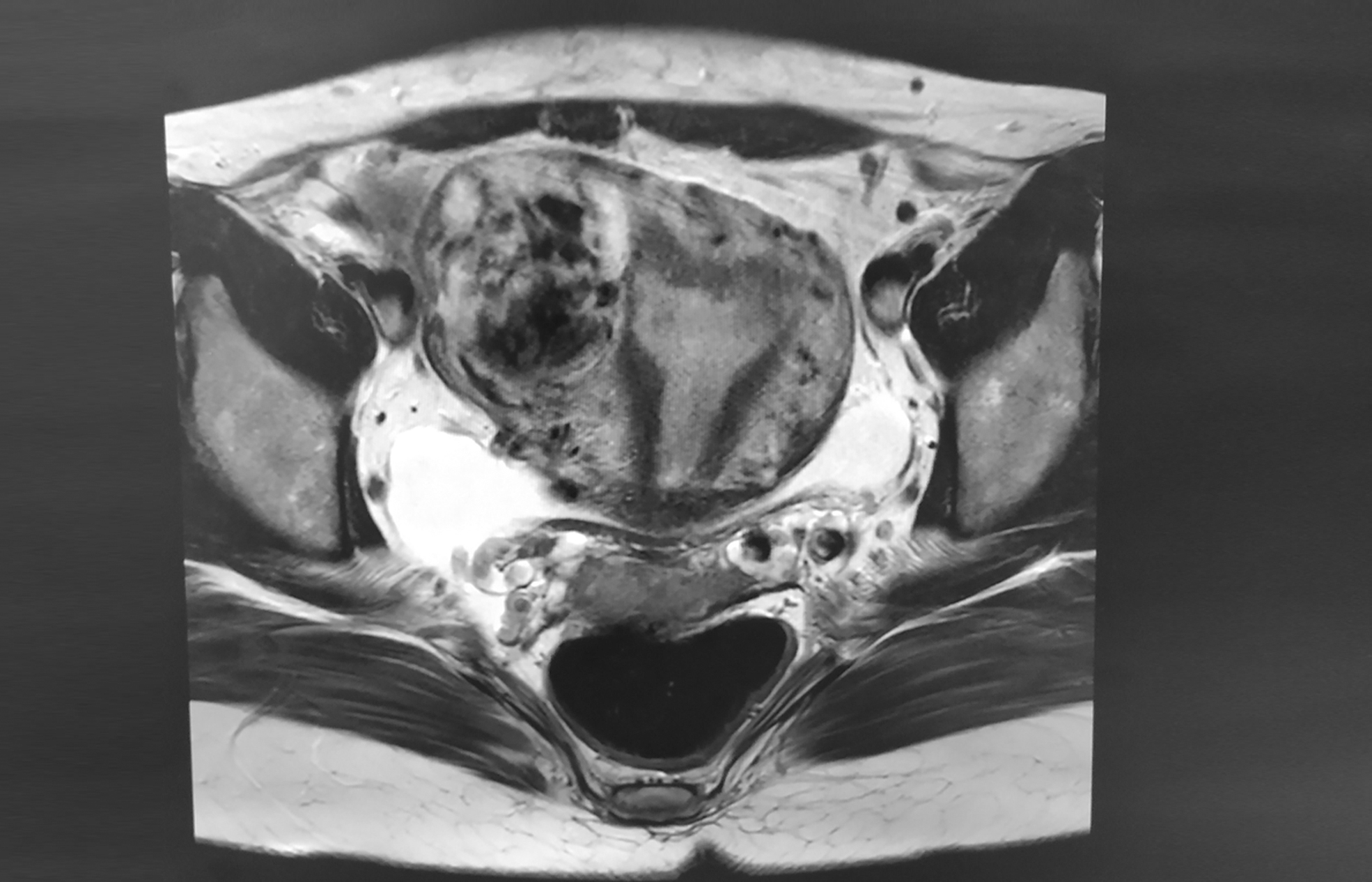
Magnetic resonance imaging with a T1-weighted view of the transverse section. This section shows a distinctly empty endometrial cavity with a round heterogeneously T1-hypertense peripheral rim and central cystic area, suggestive of a right interstitial ectopic pregnancy with an overlying thin myometrium.
Given her thin overlying myometrium, with her high ß-hCG level, laparoscopic treatment of her right interstitial ectopic pregnancy with a myomectomy was planned. A diagnostic hysteroscopy showed a normal endometrial cavity with distended right ostia, filled with products of conception, and a normal left ostia. Four-port laparoscopy (Karl Storz Image S1, Tuttlingen, Germany) was performed with a 10-mm supraumblical optical port and 3 lateral 5-mm ports. On inspecting the abdominal cavity, her uterus was 12 weeks' size with a bluish, bulging, rounded mass that was 4 × 4 cm at the right interstitial area (lateral to the round ligament) with a type 2–5 pan mural fibroid, measuring 5 × 5 cm, adjacent in the right anterolateral area (Fig. 3). The fallopian tubes and ovaries were normal.

Laparoscopic preoperative image defining the anatomy and close relationship of a right anterolateral pan mural fibroid (M) with an interstitial ectopic pregnancy (E). Color images are available online.
Vasopressin was inserted at the intersection of the uterus and the ectopic pregnancy in a dilution of 10 units in 200 mL of fluid. The base of the ectopic pregnancy was coagulated with bipolar forceps (RoBitm Karl Storz Grasping Forceps, Tuttlingen, Germany). A right salpingectomy was initiated from the fimbrial end of the tube with a LigaSure,tm 5-mm sealer and divider (Medtronic Laparoscopic Medtronic, Dublin, Ireland) up to the base of the right cornua. An oblique linear incision was made over the most-bulging part of the ectopic pregnancy. The products of conception were isolated all around from the uterine musculature with a suction cannula and a Harmonic (shear) Scalpel® (Ethicon Endo-Surgery, Somerville, New Jersey, United States). A right cornuostomy was performed with the Harmonic Scalpel to excise all the products of conception and detach the right tube from the uterus (Fig. 4).
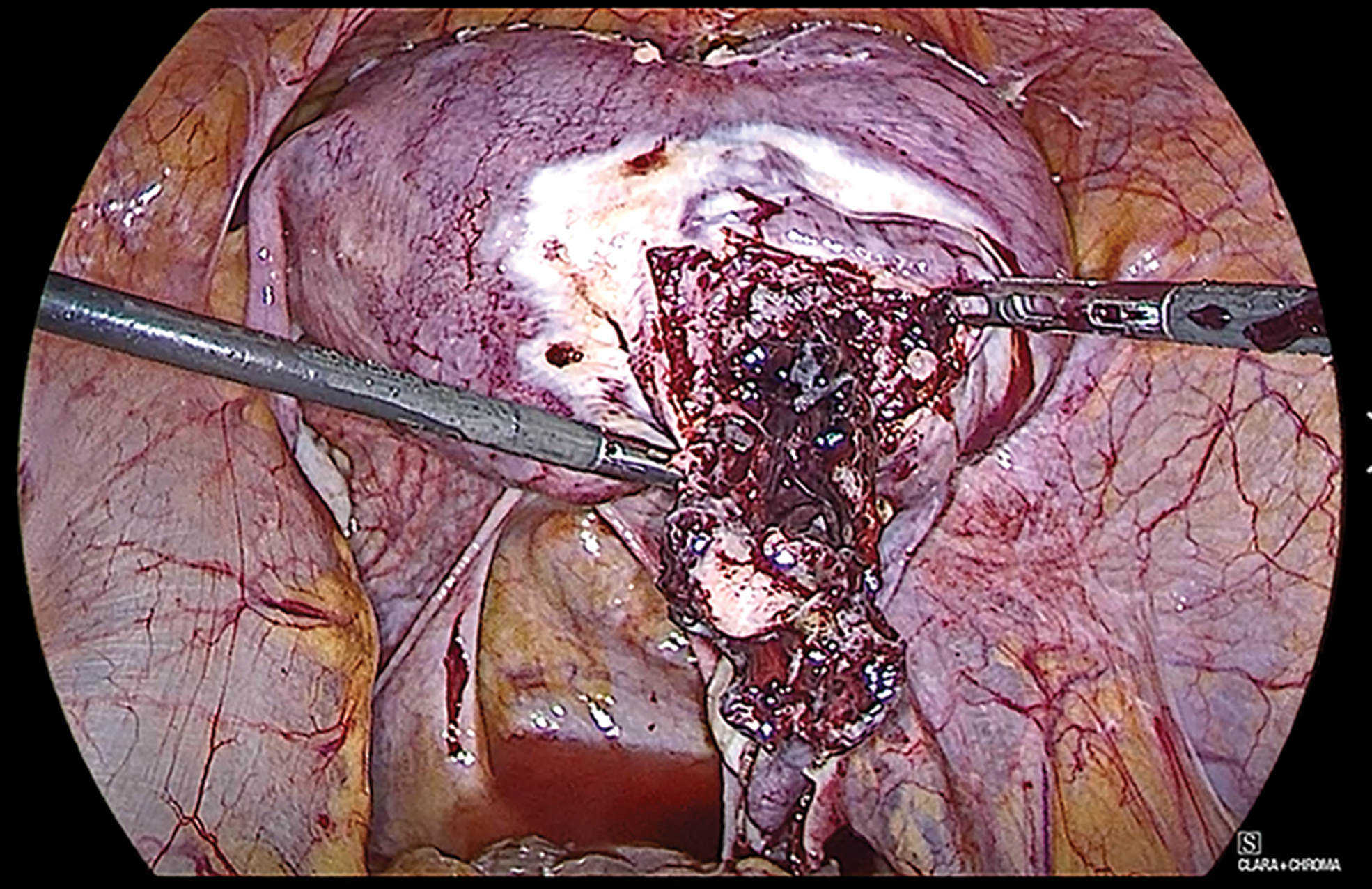
Laparoscopic view during removal of ectopic contents after linear cornuostomy incision, and left salpingectomy of the ectopic pregnancy with hanging contents and fibroid at the base of the ectopic pregnancy. Color images are available online.
Post excision of these products, at the base of the ectopic pregnancy, the fibroid was visualized. Given that the fibroid could hinder suturing the myometrial defect, it was decided to also remove the fibroid. Vasopressin was inserted into the fibroid at the subcapsular level. A separate oblique incision was made over the bulge of the fibroid, which was subsequently removed, using the Harmonic Scalpel, with traction and countertraction. The consistency and planes of the fibroid were hard-calcified and ill-defined, respectively. The residual myometrial defect was repaired in multiple layers with a barbed V-Loctm 1-0 barbed suture (Medtronic, Dublin, Ireland) till hemostasis was ensured. An indigenous endobag (made with a Transurethral Resection of the Prostate set cover) was used for specimen extraction. A Rotocut G1–12-mm power morcellator (Karl Storz) was inserted through the lower left port. The fibroid was morcellated into the endobag and the rest of the products were removed, contained in the endobag. Rectus sheath closures of the ports were performed. The operative time was 60 minutes with an average blood loss.
Results
The patient had a smooth recovery and was discharged the following day. Histopathologic examination of the specimens was consistent with products of conception with a calcified fibroid. ß-hCG-level monitoring was done at 48 hours, 1 week, and then weekly post surgery. Her ß-hCG level became negative at 3 weeks post surgery.
Discussion
Interstitial ectopic pregnancies comprise 2%–4% of ectopic pregnancies. The small (1 cm) and narrow (0.7 cm diameter) medial-most part of the fallopian tube opens into the uterus. Surrounding myometrium makes this a relatively thick portion of the tube, allowing greater distensibility, compared to its distal lateral segment. 1 Hence, rupture of an ectopic pregnancy in this interstitial area occurs later (> 12 weeks) than a tubal ectopic pregnancy (∼ 6weeks). However, the mortality is 7 times higher (2.5%), compared to pregnancies in other ectopic locations, largely due to the hemorrhaging that occurs when the pregnancy is in an interstitial location. Predisposing factors for an interstitial pregnancy include a history of previous ectopic pregnancy, in-vitro fertilization, and an ipsilateral salpingectomy. 2
Despite technical advances, the diagnosis of an interstitial ectopic pregnancy remains difficult and might be confused with an intrauterine pregnancy (an angular pregnancy). Ultrasound diagnosis was suggested by Rizk et al. by using three pointers to use when diagnosing an interstitial pregnancy
3
:
An empty uterine cavity A chorionic sac seen separately 1 cm from the most lateral edge of the uterine cavity A thin myometrial layer surrounding the chorionic sac.
3
MRI criteria are identical to US criteria. MRI can be used to make the diagnosis when the results of a US scan are inconclusive. The current case met 2 (first and third) of the criteria, stated in the above-listed points, in an MRI of her pelvis.
There is no consensus in the literature on how to best manage an interstitial pregnancy. Cornual resection has been advocated by some researchers, but it carries an increased risk of uterine rupture in a subsequent pregnancy. Methotrexate, especially in unruptured cases, has also been suggested, but this might be associated with an unpredictable risk of rupture and bleeding, requiring emergency surgery. A minimally invasive approach—including laparoscopic cornuostomy, salpingostomy, and cornual resection—has been described in few case reports.
Cornuostomy involves making a linear incision at the bulge after vasopressin instillation and removing the products of conception with blunt or sharp dissection, followed by closure with an absorbable suture. Cornual resection has been recommended in advanced interstitial pregnancies >3–4 cm, which entails making a circumferential incision above the pregnancy, along with performing an ipsilateral salpingectomy, followed by closure of redundant myometrium and serosa. 4 Chen et al., in 2019, recommended laparoscopic cornuostomy as a better surgical approach, compared to wedge resection. 5 The former approach has a shorter operating time and also promotes a better future pregnancy outcome. For the current case, surgical management was performed due to the patient's high ß-hCG load and thin myometrium. Laparoscopic cornuostomy was also performed, because of the patient's desire for future fertility.
The possible etiology of the fibroid responsible for this patient's interstitial ectopic pregnancy can be possibly: (1) the pressure of the fibroid on the ostium; (2) disturbed fallopian tube peristalsis resulting in stasis and implantation of embryo; and (3) defective uterine contractility.
There is a paucity of literature described for laparoscopic management of fibroids with interstitial ectopic pregnancies. However, 1 case study was somewhat similar to the current case. Al-Kharusi et al. attempted laparoscopy and converted later to laparotomy for a right cornual ectopic pregnancy in proximity to a 8-cm subserosal fibroid. 6 That patient was a 25-year-old primigravida who presented at 7 weeks' POC with failed medical management and a live ectopic pregnancy. The surgeons performed a myomectomy first and, then, were able to identify the pregnancy at the base of the myoma bed. The ectopic pregnancy was removed by wedge resection without entering the endometrial cavity. In contrast to this case, it was necessary to remove the fibroid after performing a cornuostomy, as the fibroid was hindering closure of the myometrial defect.
Conclusions
Interstitial ectopic pregnancy, although a rare kind of ectopic pregnancy, is the most minacious kind of ectopic gestation, with the potential to hemorrhage and result in significant mortality. Timely diagnosis by either a three-dimensional US scan or MRI of the pelvis is of utmost importance. Surgical management, with laparoscopic cornuostomy and salpingectomy, is appropriate, keeping in mind a patient's desire for future fertility. Presence of a pan mural fibroid might be considered as an influence in the development of this kind of ectopic pregnancy; such a fibroid should be simultaneously extracted if it is encountered during surgical management.
Footnotes
Acknowledgments
The authors would like to acknowledge the continuous efforts of Dr. Kunal Chandra (MBBS), and Dr. Arti Chitkara (MBBS, MD).
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this article.