
Abstract

Editor: Abdominal wound dehiscence is a major cause of morbidity after cesarean section or hysterectomy. In the literature, we found that the overall incidence rate of wound dehiscence of all obstetrics and gynecology laparotomies has been variously reported as 3.6%–29%. 1 There are many risk factors; first of all, obesity, but also diabetes, length and type of surgery (emergency), no short-term prophylaxis, smoking, advanced age, anemia, malnourishment, immunosuppression, chorioamnionitis, poor hemostasis, and tissue traumata.
Obesity and diabetes are the highest risk factors for wound complications, probably because the vascular supply and tissue oxygen levels of subcutaneous fat in these cases are poor and altered. Moreover, in obese women, other factors might predispose these patients to surgical-site necrosis and infection such as high intraabdominal pressure; higher risk of seroma, hematoma, and tissue edema; persistent skin moisture; higher prevalence of diabetes; lower tissue concentrations of prophylactic antibiotics; and longer operations and tractions on the abdominal wall. 2 Wound dehiscence increases morbidity, mortality, and, also, the cost of care in this population, with a lower quality of life.
We found literature, showing that management of wound dehiscence after gynecologic incisions, especially in obese and/or diabetic patients, includes spontaneous healing and superficial wound closure. However, in obese and diabetic patients, it is often not possible to proceed with direct closure of wound disruption because the tissue is devitalized or infected.2,3 Moreover, most of these women do not willingly accept an immediate reoperation or long-term use of medications. However, evidence-based guidelines for management are insufficient; so, clinical studies are necessary to assess optimal management strategies.
We propose a management protocol that was successfully applied to 13 obese patients (body mass indices >30 kg/m2) with severe wound dehiscence (Fig. 1):
Extensive debridement of devitalized tissue (using a Versajet® (Smith & Nephew, Watford, United Kingdom) system Tissue biopsy for cultural examinations and eventual specific systemic antibiotic therapy Negative-pressure wound therapy (NPWT), using a VAC Instill® system, (Kinetic Concepts, Inc. [KCI], San Antonio, USA; black foam, 20 minutes of local antiseptic fluid washing, 120 minutes of continuous suction at 125 mm Hg for 1 week) Reevaluation of wound and eventual new debridement and tissue samples for microbiologic evaluation New cycles of NPWT (after at least 2 negative microbiologic evaluations, the VAC Instill system is changed to a VAC® system), until we observe adequate granulation tissue that is ready to spontaneously re-epithelize, or have direct suturing or skin grafting.
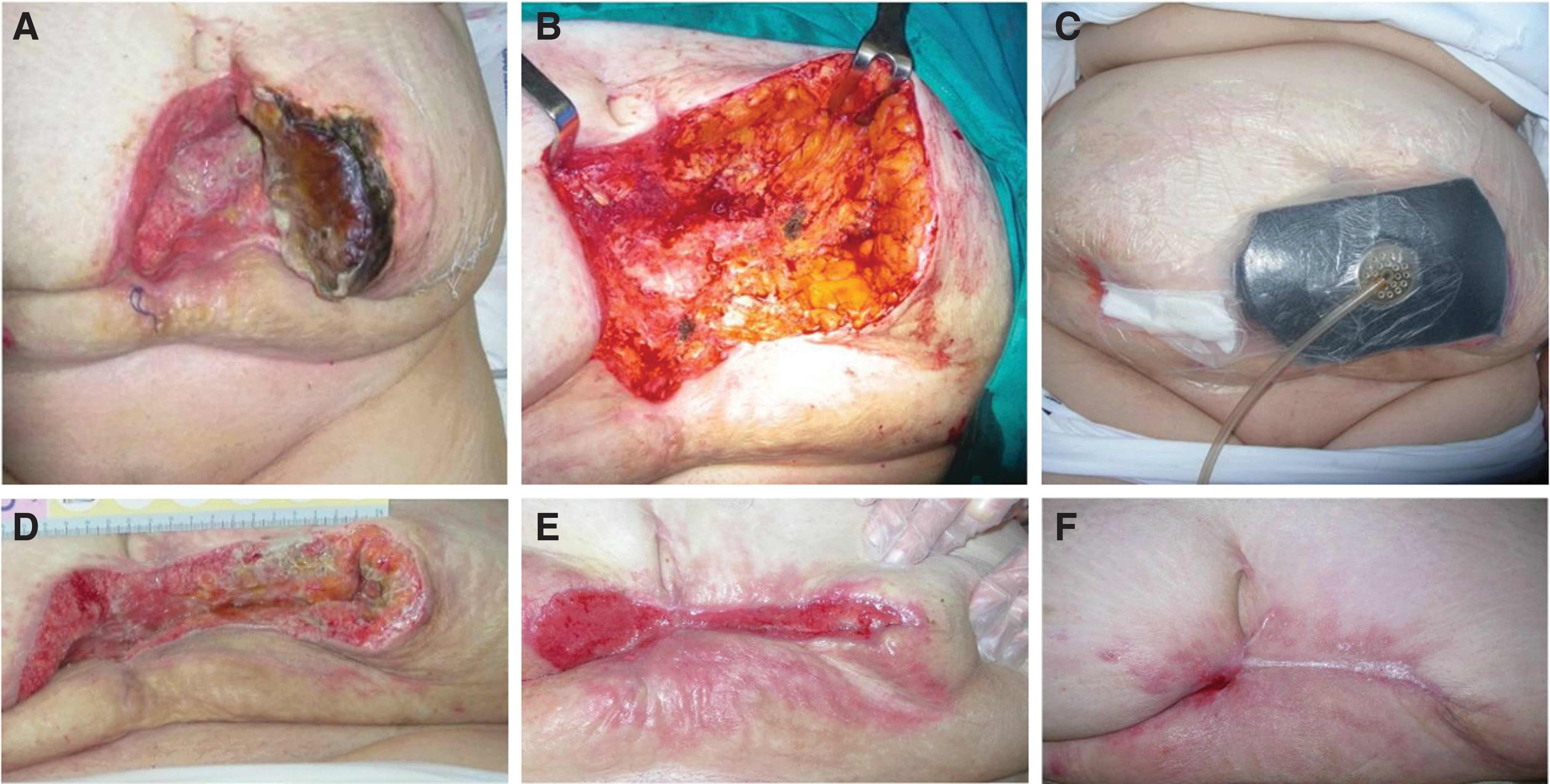
Management protocol of a wide abdominal dehisced wound posthystectomy in an obese woman (57 years' old, body mass index: 39.3 kg/m2; diabetic; smoker):
NPWT is used to treat a variety of wounds; it acts through various mechanisms: management of exudate and edema; decrement of bacterial colonization; and increment of tissue perfusion and local oxygen levels, of cellular replication and granulation-tissue growth, and of wound contraction. 4
A review of all our cases suggested that NPWT is a valuable alternative in selected cases of wide dehiscence of abdominal wounds in obese women after hysterectomy or cesarean section, especially when a surgical closure is not indicated or not desired by a patient. The management protocol presented here is safe, simple, cost-effective, and well-accepted by patients.