
Abstract
Background:
Primary presentation of endometriosis with spontaneous hemoperitoneum is rare. We report a 22-year-old woman presenting with endometriosis with spontaneous hemoperitoneum.
Case:
A 22-year-old woman was referred with history of abdominal distension and pain along with loss of appetite for 2 months and melena for 2 days. There was marked abdominal distension with fluid thrill and guarding for which abdominal tuberculosis was suspected but ruled out by cartridge based nucleic acid amplification test (CBNAAT) and culture. Ultrasonography of abdomen showed a cystic lesion of size 42 × 35 mm in right adnexa with internal echoes and presence of significant septate peritoneal fluid with low level echoes. Review of history with us revealed severe dysmenorrhea for the past 10 years. Magnetic resonance imaging was carried out that showed mildly enlarged bilateral ovaries containing cysts of varying signal intensities, with significant peritoneal fluid collection with septations, suggestive of endometrioma with hemoperitoneum.
Results:
Diagnostic laparoscopy was performed, which was converted to laparotomy due to technical difficulty. Intraoperatively, 2 L of thick coffee-colored fluid was drained. Endometrial implants were noted on the peritoneal surfaces, with sigmoid colon being densely adherent to the Pouch of Douglas. Adhesiolysis along with right ovarian cystectomy was done. Histopathology confirmed the diagnosis. She was treated with injection goserelin postoperatively, and was asymptomatic at 3 months and 1 year follow-ups.
Conclusions:
Primary presentation of endometriosis with spontaneous hemoperitoneum is rare. Endometriosis should be kept in the differential diagnosis of a woman in the reproductive age presenting with spontaneous hemoperitoneum.
Introduction
Endometriosis, defined as the presence of functional endometrial glands and stroma outside the normal endometrial canal, is a common cause of pelvic pain and subfertility. 1 Primary presentation with spontaneous hemoperitoneum is rare. We report a case of endometriosis presenting with spontaneous hemoperitoneum in a 22-year-old sexually naive woman, and discuss the challenges in diagnosis and management.
Case
A 22-year-old woman was referred to us for further evaluation from the department of gastroenterology. She had presented with history of abdominal distension and pain along with loss of appetite for 2 months and melena for 2 days. There was no history of fever, cough, or any chronic illnesses. She had been evaluated at her local hospital for malignancy, and cancer antigen 125 (CA125) was found to be mildly raised (49.39 U/mL), carbohydrate antigen19-9 (CA19-9) and carcinoembryonic antigen (CEA) were normal, and lactate dehydrogenase (LDH) was markedly increased (2173 U/L). She was afebrile, thin built, with moderate pallor, stable vitals, and no pedal edema or jaundice. There was marked abdominal distension with fluid thrill and guarding for which abdominal tuberculosis was suspected clinically and the patient was further worked up. Tuberculin test was negative. Her hemoglobin was 11.2 g/dL. Ultrasonography (USG) of abdomen showed a cystic lesion of size 42 × 35 mm in the right adnexa with internal echoes, suggestive of hemorrhagic cyst (Fig. 1A). There was also significant peritoneal fluid with low level echoes and few septations (Fig. 1B). Ultrasound-guided paracentesis was performed by the radiologist. The ascitic fluid was hemorrhagic (coffee colored) and negative for acid fast bacilli by cartridge based nucleic acid amplification test (CBNAAT) and culture, but adenosine deaminase was elevated (89 IU/mL). Coagulation profile was normal.
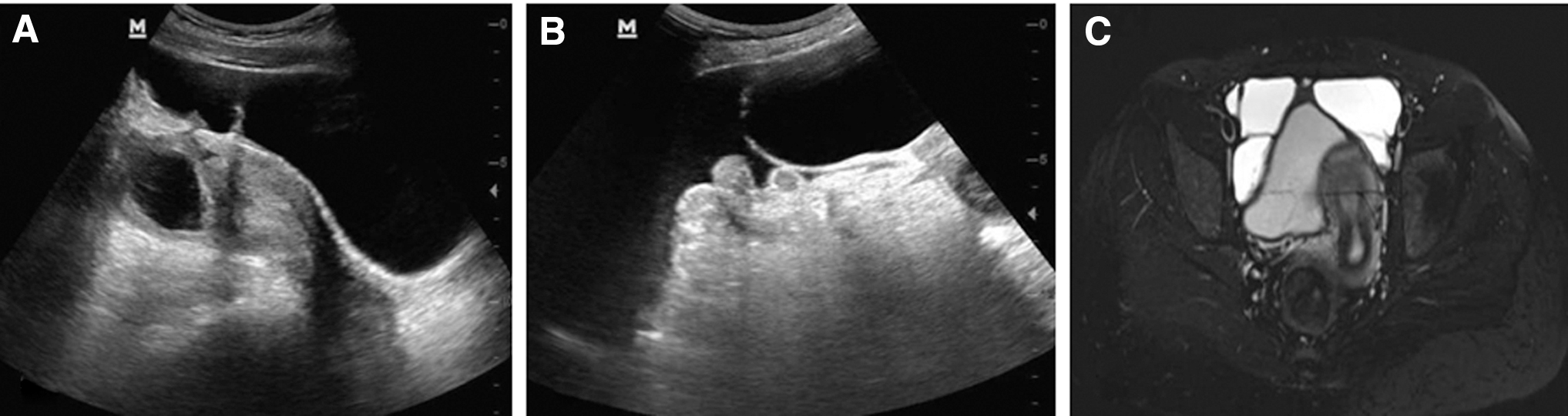
Two-dimensional USG showing
Review of history with us revealed severe dysmenorrhea for the past 10 years. Urine pregnancy test was negative. Magnetic resonance imaging (MRI) was carried out for further evaluation and to rule out malignancy. MRI showed mildly enlarged bilateral ovaries containing cysts of varying signal intensities, with T2 layering in the left ovarian cyst favoring endometrioma. Significant peritoneal fluid collection with septations was noted that appeared hyperintense on both T1 weighted image (WI) and T2WI suggesting hemorrhagic content (Fig. 1C).
Results
In view of hemoperitoneum due to endometriosis with symptoms, and having ruled out malignancy, ruptured ectopic pregnancy, ruptured corpus luteum, and abdominal tuberculosis, diagnostic laparoscopy was performed. This was converted to laparotomy due to technical difficulty. Her hemoglobin on the day of surgery was 9.6 g/dL. Intraoperatively, endometrial implants were noted on the peritoneal surfaces, with sigmoid colon being densely adherent to the Pouch of Douglas (Fig. 2A). Two liters of thick hemorrhagic coffee-colored fluid was drained (Fig. 2B). Adhesiolysis along with right ovarian cystectomy, multiple biopsies from peritoneal sites, and fulguration of the endometriotic implants was done. She was administered one unit of packed cell transfusion intraoperatively. Postoperative period was uneventful and she was discharged on the sixth postoperative day.

Diagnostic laparoscopy showing
Histopathology from the peritoneal sites showed fibrocollagenous tissue with blood vessels. Right ovarian cyst wall had fibrocollagenous tissue with blood vessels, endometrial glands, and stroma. Final diagnosis of left ovarian endometrioma with superficial peritoneal endometriosis, deep infiltrating endometriosis, and spontaneous massive hemoperitoneum was made. She was given two doses of injection goserelin 3.6 mg subcutaneously 3 months apart. The patient was asymptomatic at 3 months (Fig. 2C) and doing well at 1 year follow-up.
Discussion
Endometriosis is a common cause of pelvic pain and infertility, affecting 10% of women in the reproductive age group. 1 Mean age of diagnosis is 25–29 years. 2 Patients commonly present with chronic pelvic pain, dysmenorrhea, subfertility, and less commonly with dyspareunia, low backache, and dysuria. Common locations for endometriotic deposits are retrocervical/uterosacral, ovaries, rectosigmoid colon, bladder, vagina, round ligaments, and ureters, with cesarean section scar, deep subperitoneal tissues, gastrointestinal tract, urinary bladder, chest, and subcutaneous tissues being less common. 3
Three different manifestation of endometriosis are ovarian endometriomas, superficial peritoneal implants, and deep infiltrating endometriosis. 4 Patients with peritoneal endometriosis can be asymptomatic. Deep pelvic endometriosis commonly present with pelvic pain, dysmenorrhea, dyspareunia, and infertility and rarely melena, hematochezia, hemothorax, and urinary tract symptoms depending on location of deposit. 5 Cyclical pain favors the diagnosis of endometriosis, but may not be always present.
Hemoperitoneum is a rare presentation of endometriosis. 6 Pathophysiology is supposed to be due to irritation of serosal surfaces by free blood released from ruptured chocolate cysts. 7 Melena in endometriosis is usually secondary to intestinal penetration or rectovaginal deposition or appendiceal implants causing chronic bleeding. Melena in our case was probably due to gastrointestinal bleed with sigmoid colon involvement, just like she had spontaneous hemoperitoneum from endometrioma/peritoneal deposit. Recent evidence is growing regarding the role of platelet and platelet-derived factors in the promotion of endometriosis. 8 Melena in the present case could also be explained by this theory.
USG is highly sensitive for diagnosis of ovarian endometrioma. In USG, endometriomas are seen as unilocular or multilocular cystic adnexal lesions with low level internal echoes without any internal vascularity. MRI has greater specificity for the diagnosis of endometriosis or endometriomas. MRI findings in endometriosis are multiple T1 hyperintense adnexal cysts that suggest endometrioma. The lower T2 signal intensity of endometriomas compared with that of functional or simple ovarian cysts has been described as “T2 shading.” 9 A close differential is a functional hemorrhagic cyst. But more T1 hyperintensity, T2 shading sign, and bilaterality favora diagnosis of endometrioma. 10 In addition to T1 and T2 hyperintense adnexal cysts and T2 shading in left adnexal cyst in our patient, the pelvic fluid had loculations with slightly different signal intensity that could be due to hemorrhage of different stages. This finding again favors a diagnosis of endometriosis.
Direct visualization by laparoscopy is the gold standard for diagnosis and also has therapeutic advantage. In some cases, biopsy may be necessary to confirm the disease.
First-line treatment is medical therapy that includes progestogens favoring a pseudopregnancy state or Danazol/GnRH agonist that produces pseudomenopausal state and stop cyclical bleeding. Surgical treatment is indicated in patients with failed medical therapy or with extensive endometriosis.
The present case is a young woman presented with abdominal distension and melena and clinically thought to be abdominal tuberculosis that is endemic in our country. On investigation, there was hemoperitoneum. The common causes of hemoperitoneum in the reproductive age group are ruptured ectopic pregnancy, ruptured corpus luteum, and malignancy, which were ruled out in our case. USG and MRI findings were suggestive of endometriosis with hemoperitoneum, which was present intraoperatively and confirmed by histopathology. In fact, endometriosis is a major risk factor for spontaneous hemoperitoneum in pregnancy, responsible for over half of all cases in pregnancy.11,12 It has also been reported as a rare cause of hemoperitoneum in the nonpregnant woman, like in our case.6,13,14 Recently, the presence of hemoperitoneum has been described as a precursor for deep infiltrating endometriosis. 15 Hence, it is imperative that clinically significant hemoperitoneum be drained, and the cause addressed.
To conclude, endometriosis is a common gynecologic condition presenting with chronic pelvic pain and infertility. However, it should be kept in the differential diagnosis of spontaneous hemoperitoneum in females of reproductive age group as a rare cause.
Footnotes
Authors' Contributions
S.S., P.S., and M.K.P. were involved in the management of the case. S.N. provided critical imaging inputs. All authors helped in data collection and preparation of the final article to be submitted. The article has been read and approved by all the authors, the requirements for authorship as stated earlier in this document have been met, and each author believes that the article represents honest work. Written informed consent was obtained from the patient.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.