
Abstract
Background:
Prolapse coexisting with carcinoma of the cervix is a rare occurrence. There is no standardized management for this rare combined entity.
Case:
A 72-year-old patient with procidentia had a suspicious-looking ulcer on her prolapsed uterus. Biopsy of the cervical lesion confirmed a well-differentiated squamous-cell carcinoma. She underwent an abdominal, modified radical hysterectomy with bilateral salpingo-oophorectomy, bilateral pelvic lymphadenectomy, and sacrocolpopexy. Postsurgery, she received concomitant radiotherapy and chemotherapy as adjuvants.
Results:
At her 6-month follow-up, her vault was healthy and well-suspended.
Conclusions:
This was a successful abdominal approach to carcinoma of the cervix coexisting with prolapse. Sacrocolpopexy was performed as a concomitant procedure that provided standardized management for cervical carcinoma due to feasibility of bilateral pelvic lymphadenectomy along with adequate access for targeted radiotherapy without inducing any visceral symptoms.
Introduction
Carcinoma of the cervix complicated with a complete prolapse as a combined condition is scarce. Management of such cases are even more sparsely covered in the surgical literature. Few case reports are available; those that exist describe mostly the vaginal route. An abdominal route with sacrocolpopexy has not yet been acknowledged. This approach not only provides relief from the prolapse but also provides adequate access for radiotherapy without inducing visceral symptoms due to sacrocolpopexy performed concomitantly.
Case
A 72-year-old woman (para 6, live 6), who was overweight and had diabetes, presented with a long-standing prolapse of 8 years with urinary symptoms. She had a history of hypertension and diabetes for the last 25 years.
On general physical examination, she was moderately built with a body mass index of 28. Bilateral examination of her breasts was insignificant for any problems. On the abdominal examination, it was noted that she had a tubal-ligation scar. Local examination showed that her cervix was lying well beyond the introitus with a huge cystocele and rectocele, implying stage IV of Pelvic Organ Prolapse–Quantification (POP-Q) classification (Procidentia Aa +3, Ba +6 Ap +3, C + 8, D -2, gh 4 cm, TVL 8 cm, pb 2 cm). There was a suspicious lesion of ∼4 × 2 cm at the level of the cervix going inside the os with puckered surrounding tissue (Fig. 1). The overlying mucosa of the vagina was atrophic and dry. The parametrium and rectum appeared to be free on a rectovaginal examination. Biopsy of the cervical lesion confirmed a well-differentiated squamous-cell carcinoma. She was staged clinically as Ib2 after the biopsy report. Magnetic resonance imaging of her abdomen and pelvis revealed a soft, lobulated tissue mass of 3.8 × 3.6 × 2.9 cm replacing the cervix, going 1 cm above the internal os, and involving the upper third of the vagina. No parametrial involvement nor any lymphadenopathy were seen.
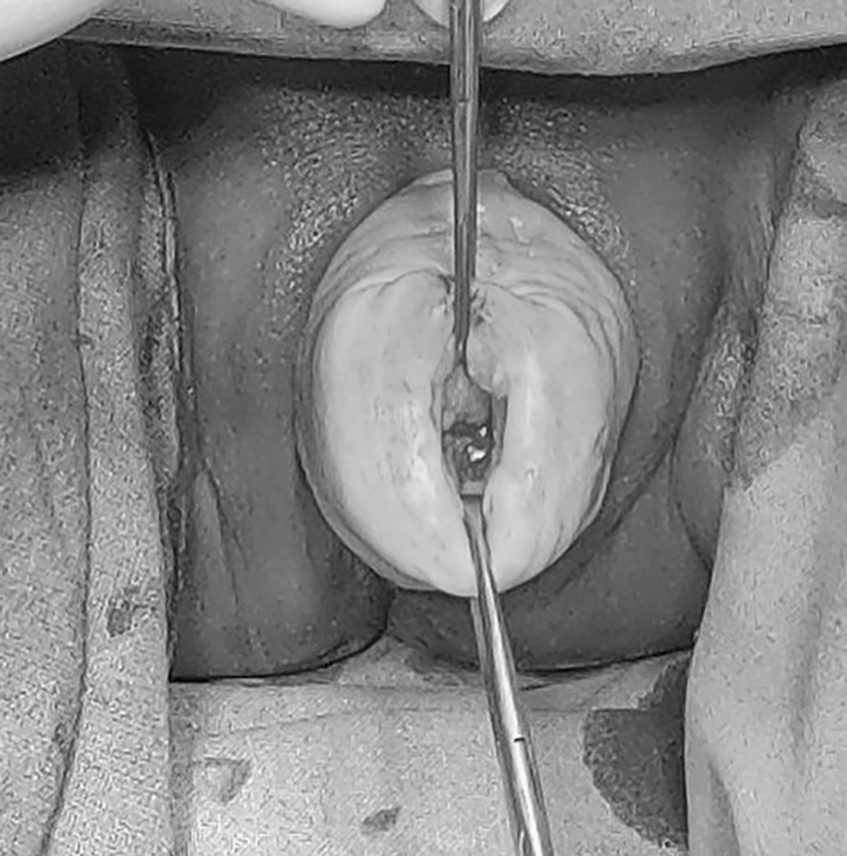
Preoperative view with growth replacing the posterior lip of the cervix with procidentia.
This patient underwent abdominal radical hysterectomy (Wertheim's) with a bilateral salpingo-oophorectomy, a pelvic lymphadenectomy, and concomitant sacrocolpopexy. Dissection of the presacral space was performed to expose the anterior longitudinal ligament at the S–2 and S–3 levels. The vault was then suspended with anterior longitudinal ligaments with nonabsorbable Prolene® Number 1 sutures. These 2 suspension sutures resulted in restoration of the apical prolapse to the level of point C drifted to −8 (according to POP-Q classification) (Fig. 2).

Postoperative image of the suspended vault.
Final histopathology was conclusive for nonkeratinizing, grade 2, moderately differentiated, squamous-cell carcinoma limited to the cervix with a tumor-free margin of 3 mm. (Fig. 3). Stromal invasion was 6 mm with lymphovascular invasion (LVI). The vagina, parametrium, and all 39 lymph nodes were free of the tumor, making the final staging as stage Ib2 (pT2a2, pN0). She received external-beam radiotherapy with 6 mV photons to a dose of 50 gray/25 fractions over 5 weeks, along with 3 cycles of concurrent weekly chemotherapy (100 mg of carboplatin) in view of the nearer free tumor margins and LVI. After completion, she also received vaginal brachytherapy 2 weeks later weekly for 2 doses with the ovoids (7.5 gray/single fraction) along with chemotherapy.

Resected cut section of surgical specimen of the uterus, tubes, ovaries, and parametrium with tumor filling and infiltrating the cervical stroma with a liberal tumor-free margin.
Results
This patient was followed for 6 months; at that time, her vault was healthy and well-suspended.
Discussion
Cervical cancer ranks as the second leading cause of female cancer deaths in India. About 96,922 new cervical cancer cases were diagnosed annually in India in 2019. 1 India alone accounts for one-quarter of the worldwide burden of cervical cancer. Most patients are in the 60–80-years age group, and procidentia has been present for 10 years or more in 60% of cases. 2
It has long been established clinically that a prolapsed uterus, although exposed to constant mechanical irritation, is remarkably free from the risk of cancer. This is explained by the assumption that the uterus' displacement removes it from the environment of the vagina, which is rendered harmful by exudates. 3
The reported incidence of patients with cervical cancer undergoing vaginal hysterectomy for prolapse was 0.3%–0.8% in a retrospective review. 4
Many treatment options have been discussed in the literature for prolapse complicating cervical cancer but no treatment has been standardized. Various modalities used include structured radiochemotherapy with obliterative vaginal surgery 4 ; vaginal hysterectomy with pelvic-node dissection, followed by chemoradiation therapy for stage IIIB cancer 5 ; laparoscopic radical hysterectomy 6 ; vaginal simple hysterectomy with upper vaginectomy 7 ; and pessary insertion with perineorrhaphy and concurrent chemoradiotherapy.8,9 Borges da Silva et al. reported 2 similar cases treated with radical vaginal hysterectomy, followed by external-beam radiation. 10 However, the vaginal route has a limitation of unavailability of lymph node status of the patients. Nevertheless, this can be overcome by combining it with a laparoscopic route through which lymph-node assessment and lymphadenectomy can be performed. At the same time, colpopexy can be performed vaginally (with sacrospinous fixation) or via a laparoscopic route (sacrocolpopexy). However, none of the case reports have described sacrocolpopexy along with radical hysterectomy for cervical carcinoma coexistent with procidentia.
Concomitant chemoradiotherapy has become the standard of care for high-risk, early stage, locally advanced cervical cancer over radical hysterectomy for cervix-confined bulky tumors (> 4 cm, IB2). However, this is not true when prolapse complicates the cervical cancer, due to disproportionately higher radiation to visceral organs associated, like the bladder and rectum. Thus, the best management in these cases appears to be removal of the bulk of the disease surgically (hysterectomy with pelvic lymph-node dissection) and sacrocolpopexy to avoid radiation-induced cystitis and proctitis in patients with cystoceles and rectoceles, respectively.
The vaginal route is the most-preferred route of hysterectomy in most case reports of combined problems; however, in patients without prolapse, an abdominal approach is preferred.
In a systematic review article by Matsuo et al., 11 which reviewed 78 case reports, of them only 10 of the articles reported that surgical repair was performed (12.8%), and 9 of the cases underwent concurrent prolapse repair with surgical treatment for cancer of the cervix. 2 Among the 9 articles, the most-common procedure for prolapse repair—by percentages—were anterior colporrhaphy (55.6%), perineorrhaphy (33.3%), posterior repair (11.1%), and colpocleisis (11.1%). These results suggested that surgical approach needs to be considered in women with cervical cancer complicated by complete uterine prolapse if the patient's condition and medical comorbidity are not limitations to the surgery.
Conclusions
Management of uterovaginal prolapse associated with carcinoma of the cervix is a long-standing problem due to unique difficulties in clinical staging, and surgical and radiotherapy planning due to the anatomy distortion caused by prolapse. Abdominal radical hysterectomy with sacrocolpopexy, followed by concurrent chemoradiation is a treatment strategy for carcinoma of the cervix. Treatment of apical prolapse surgically by sacrocolpopexy on the sacral area with nonabsorbable sutures confers an effective dose of radiotherapy at the desired points on the vaginal vault.
Footnotes
Acknowledgments
The authors acknowledge the continuous efforts of Amenda Ann Davis MD, senior resident, Department of Minimally Invasive Gynaecology, Paras Hospitals, Gurugram, India.
Author Disclosure Statement
No financial conflicts exist.
Funding Information
No funding received for this work.