
Abstract
Background:
Tuberculosis (TB) is seldom thought of as a differential diagnosis although being the leading cause of death from infectious disease worldwide. It is estimated that abdominal TB (in the gastrointestinal tract, peritoneum, lymph nodes, or solid viscera) accounts for 1%–15% of extrapulmonary TB and for 1%–3% of all TB cases, being confused with carcinomatosis.
Case:
A 17-year-old female patient was transferred to the current authors' hospital due to fever, abdominal pain, ascites, and a previous laparoscopy showing carcinomatosis and ovarian lesions. Her serum cancer antigen–125 was 1529.8 U/mL and her lactate dehydrogenase was 2353 U/mL. Abdominal magnetic resonance imaging showed lesions with expansive aspects in the adnexal regions, suggesting a neoplastic process. Thoracic computed tomography was suggestive of an active granulomatous infectious process. Her previous laparoscopic biopsy was reexamined, showing active chronic salpingitis with necrotic granulomas and an absence of acid-fast bacilli. Laparoscopy with peritoneal biopsies was performed.
Results:
Pathology analysis of the newer specimens did show acid-fast bacilli, compatible with mycobacteriosis. This latter culture examination was compatible with Mycobacterium tuberculosis. She was treated with rifampin, isoniazid, pyrazinamide, and ethambutol for 2 months, followed by 4 months of maintenance treatment with rifampin and isoniazid. At 8 months after the end of treatment, she was asymptomatic.
Conclusions:
Tuberculosis should be considered as a differential diagnosis of ovarian cancer, especially in endemic areas. Imaging findings can be misdiagnosed as advanced ovarian malignancy, pelvic inflammatory disease, and other pathologies, being that peritoneal biopsy with pathologic examination is the only method to exclude malignant disease. Diagnosing this can be difficult but the importance of differential diagnoses for malignant conditions is important to avoid unnecessary extensive surgery.
Introduction
Tuberculosis (TB) is currently the leading cause of death from infectious disease worldwide, with 22 countries (including Brazil) accounting for 87% of the world's TB burden.1,2 In 1744, JB Morgagni was the first to report a case of TB in the female genital tract. 3 It is estimated that abdominal TB (which may involve the gastrointestinal tract, peritoneum, lymph nodes, or solid viscera) accounts for 1%–15% of extrapulmonary TB2,4–6 and accounts for 1%–3% of all TB cases. 7 This article describes an unusual presentation of TB that simulated ovarian cancer.
Case
A 17-year-old female was transferred to the Hospital Nossa Senhora da Conceição (in Porto Alegre, RS, Brazil) for fever, abdominal pain, ascites, and a previous laparoscopy that showed carcinomatosis and ovarian lesions. This previous laparoscopy had been performed 1 week earlier in a medium-complexity hospital by a general surgeon. This patient's serum cancer antigen (CA)–125 was 1529.8 U/mL (reference value: <35 U/mL) and her lactate dehydrogenase was 2353 U/L (reference range: 240–480 U/L). Test results for other tumor markers, such as α-fetoprotein, carcinoembryonic antigen, and human chorionic gonadotropin, were unremarkable. Human immunodeficiency virus (HIV) serology was negative. The pathologic finding of the laparoscopic biopsy was salpingitis, without carcinoma or any evidence of tuberculosis. The previous laparoscopy specimens were reexamined by the current hospital's pathologists, showing active chronic salpingitis with necrotic granulomas and an absence of acid-fast bacilli.
Abdominal computerized tomography (CT) showed heterogeneous expansive formations in both adnexal regions (4.5 × 3.9 cm on the right and 4.8 × 2.7 on the left) and some nodular images associated with a greater density of mesenteric fat and major omentum. Abdominal magnetic resonance imaging (MRI) showed lesions with expansive aspects in the adnexal regions (4.7 × 3.0 cm on the right and 5.2 × 2.8 cm on the left) creating an intermediate signal in T1 and T2 enhanced MRI images, and in areas of contrast enhancement and water-diffusion restriction, suggesting a neoplastic process (Fig. 1). There was no ascites. A thoracic CT showed centrilobular nodules, some branched, in both upper lobes of the lungs, especially the left lobe, as well as adjacent to the left oblique sissure, suggestive of an active granulomatous infectious process. Her uncle had died a year ago from TB and her cousin was being treated for a pulmonary TB infection.

T2 contrast enhanced magnetic resonance images on axial plane.
Fibrobronchoscopy with bronchoalveolar lavage of the anterior segment of the left upper lobe of the lung was performed. Cytology testing showed 65 cells/μL and 5 erythrocytes/mL, with differentials of 1% neutrophils, 49% lymphocytes, and 50% macrophages. The cytology testing was negative for fungi, acid-fast bacilli, or malignant cells.
A laparoscopy with peritoneal biopsies was performed, but intense pelvic adhesions prevented evaluation of the ovaries (Fig. 2). Pathology analysis did show that there were acid-fast bacilli, compatible with mycobacteriosis.
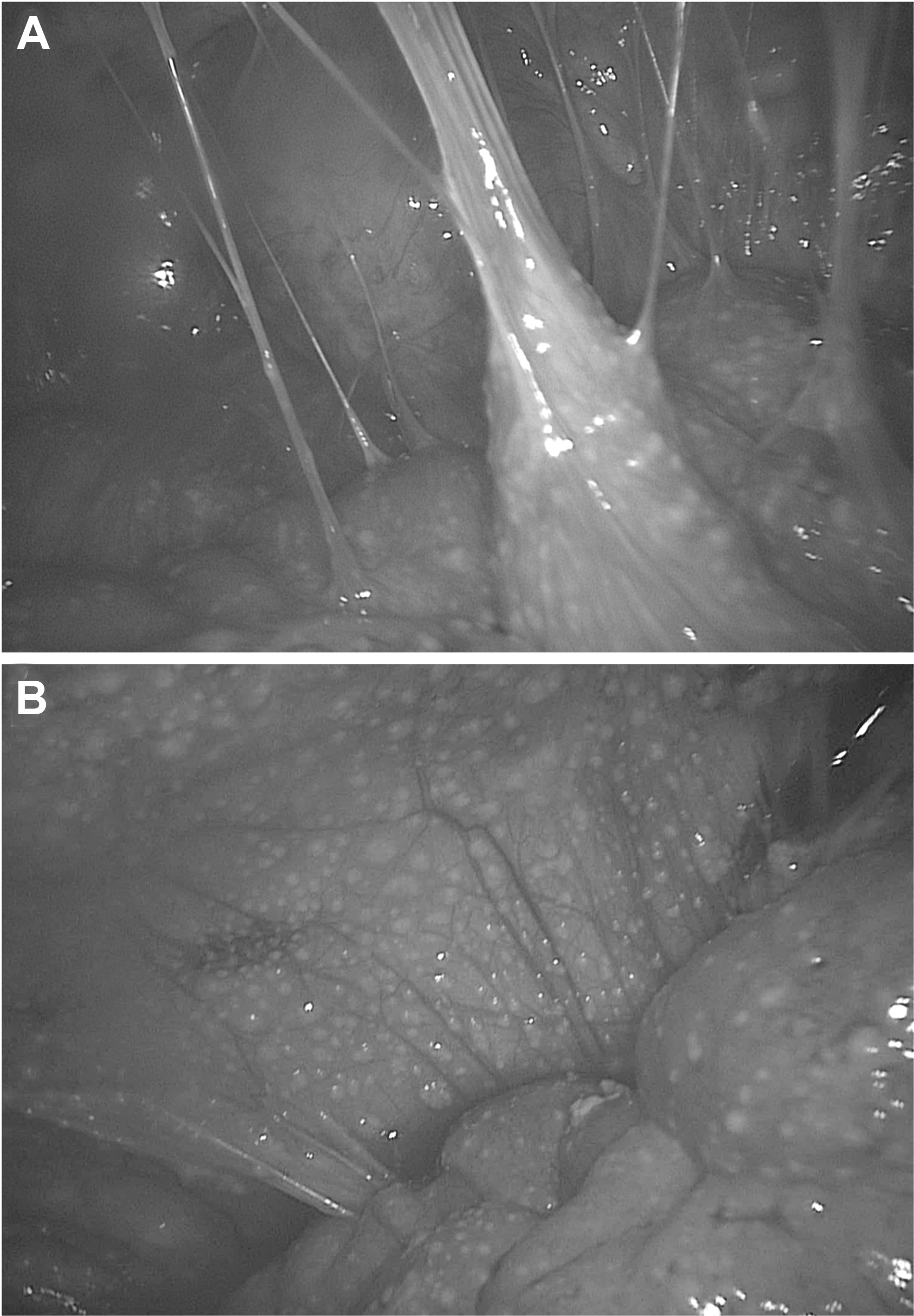
Surgical laparoscopic findings of abdominal cavity.
This patient was treated with rifampin, isoniazid, pyrazinamide, and ethambutol for 2 months, followed by 4 months of maintenance treatment with rifampin and isoniazid. A late culture examination was compatible with Mycobacterium tuberculosis.
Results
Laparoscopy with peritoneal biopsy was a successful way to confirm the diagnostic hypothesis of peritoneal TB. This patient was treated successfully with rifampin, isoniazid, pyrazinamide, and ethambutol. Eight months after the end of her treatment, she was asymptomatic; her serum CA-125 was 11.3 U/mL and her abdominal MRI (Fig. 1B) and chest CT results were unremarkable.
Discussion
Cancer is becoming the major cause of death worldwide, 8 always being one of the main diagnostic hypotheses when evaluating abdominal masses. TB can simulate different cancer sites9–12 but are seldom remembered during the investigation. Female pelvic TB mostly affects reproductive-age women and is common in developing and undeveloped countries.13–15 In females with genital TB, the fallopian tubes are affected in 94%, and salpingitis caused by hematogenous dissemination is almost always bilateral.12,16,17 Some researchers have theorized that tuberculous peritonitis results from reactivation of latent tuberculous foci in the peritoneum or from the hematogenous spread from a primary infection in the lungs, and that the absence of clinical and radiologic pulmonary evidence is related to the complete healing of these original lesions.18,19 The current patient had an active granulomatous lung infectious process on noted on her thoracic CT that was suggestive of pulmonary TB. However, sputum and bronchoalveolar lavage were negative for acid-fast bacilli.
In general, clinical manifestations of abdominal TB depend on the form of the disease and can include fever, weight loss, abdominal pain, abdominal distension, ascites, hepatomegaly, diarrhea, and an abdominal mass.13,18 Patients often have a family history of TB, which can contribute to the diagnosis. Our patient did not present with fever during the hospitalization in our unit, and a history of family pulmonary TB diagnosis is ordinary in Brazil. The acute condition may be similar to pelvic inflammatory disease (PID), including ovarian–tube abscesses. 20 Infertility generally occurs due to tubal factors, which can include total tubal blockage and an increased risk of ectopic gestation.12,20
In a retrospective study with 711 patients previously treated with different anti-TB treatment protocols to address abdominal TB (none with the current advised treatment), there were 95 pregnancies, 31 of which were ectopic. 3 In countries with a high incidence of pelvic–peritoneal TB, up to 10% of cases can cause infertility. 21
In TB-endemic areas, pure protein derived (PPD) status is useful only as a negative predictive value in immunocompetent patients. Serum concentrations of cancer antigen (CA)–125 might be elevated in peritoneal TB, ovarian cancer, endometriosis, PID, and other pathologies.5,10,13,14,17,18,22 After TB treatment, CA-125 levels usually return to normal values.13,14,23 The current patient also presented with high CA-125 levels that normalized after her anti-TB treatment. The possibility of epithelial ovarian cancer was decreased in this patient because of her age. Ovarian tumors in younger patients are usually nonepithelial ovarian cancers (germ-cell or sex-cord stromal tumors) that usually raise other tumor markers than CA-125.
Because abdominal TB has an insidious evolution with nonspecific signs, symptoms, and laboratory abnormalities, radiologic investigation (preferably CT or MRI) is advised when the disease is suspected (especially in TB-endemic areas). Abdominal CT findings, such as ascites with mesenteric or omental stranding, enlarged retroperitoneal lymph nodes, and adnexal masses can be related to peritoneal TB. 24 Unfortunately, imaging findings can be misdiagnosed as advanced ovarian malignancies or PID.5,25 Peritoneal biopsy with pathologic examination of the specimen is the only way to exclude the presence of malignant disease. A definitive diagnosis of peritoneal TB also requires biopsy material with detection of tuberculous granulomas as shown by caseation necrosis and epithelioid giant cells with acid-fast bacilli noted on staining and culture. 26 Peritoneal biopsies are performed preferably by laparoscopy, although some researchers have reported technical difficulties due to intense disease adhesions and unnecessary extensive cytoreduction surgeries.5,18 A retrospective cohort in one study had peritoneal adhesions in 55.6% of the patients. 5 Extrapulmonary TB is often paucibacillary, making the definitive diagnosis even more difficult.
Chronic granulomatous reactions and inflammations are common findings noted on pathologic evaluations but these phenomena not sufficient to establish the diagnosis of extrapulmonary abdominal TB.18,21 A definitive diagnosis of abdominal TB can be established by identifying M. tuberculosis in peritoneal fluid or by histologic biopsy, mycobacterial culture, or a protein-chain reaction.18,27,28 Direct screening (Ziehl–Neelsen staining) of the acid-fast bacilli in ascites fluid is positive in only 3% of cases; culture of the ascitic fluid can be positive in 3%–20% of cases and requires several weeks.13,19,26,29 The accuracy of culturing and protein-chain reactions (amplification of genome sequences [i.e., the IS6110 sequence]) for M. tuberculosis varies, according to some literature.18,19,29–35 Determining the level of adenosine deaminase in ascites fluid may also be helpful for making the diagnosis. A cutoff above 33 U/L for the diagnosis of abdominal TB was shown to have a sensitivity and specificity of 100% and 95%, respectively. 23 Use of GeneXpert has been suggested to raise diagnostic accuracy of clinically suspected pulmonary lesions. 36
Risk factors for the development of abdominal TB include HIV infection, cirrhosis, malnutrition, diabetes mellitus, underlying malignancy, immunosuppressive therapy, and peritoneal dialysis.1,37 None of these risk factors were present in the current patient.
Patients with abdominal TB should be treated with anti-TB therapy. In Brazil, the treatment in done in 2 phases: 2 months of rifampicin, isoniazid, pyrazinamide, and ethambutol, followed by 4 months of rifampicin and isoniazid. 38 The therapeutic response is noted by symptom reductions and decreases in levels of serum CA-125 after 2 months of treatment. 22
Conclusions
Peritoneal TB should be considered in patients with adnexal masses, ascites, and CA-125 elevations, especially in patients with previous contact histories, or who are residents in TB-endemic areas. Clinical suspicion of the condition can be difficult but differential diagnosis with malignant conditions is vital to avoid unnecessary treatments. Although an algorithm for investigation has not yet been determined, examinations, such as biopsy-directed laparoscopy, allow conclusive diagnoses and early introduction of appropriate therapies.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this article.