
Abstract
Objective:
To determine clinical factors that are associated with an increased likelihood of having oophorectomy at the time of surgery in patients with suspected ovarian torsion (OT).
Design:
This is a retrospective cohort study.
Materials and Methods:
Women <50 years of age who presented to the Boston Medical Center ED, a racially diverse urban safety net hospital, between January 1, 2009, and July 31, 2014, with a diagnosis of OT who had surgery within 1 week of presentation were retrospectively identified by ICD-9 code. Patient data (age, race, gravidity, parity, BMI, history of tubal ligation and/or oophorectomy, and affected ovary size by imaging) as well as surgical data (time from presentation to surgery, work shift when surgery occurred, intraoperative findings, pathology findings, estimated blood loss, and subspecialty of surgeon) were collected and analyzed using Fisher exact test, t-test, and Mann–Whitney U tests.
Results:
Fifty-four patients with suspected OT who underwent surgery were identified, and 42 of 54 (78%) of the suspected torsion cases had OT diagnosed at surgery. Oophorectomy was not performed in any of the non-OT cases. In patients diagnosed with OT, 25 of 42 (60%) had an oophorectomy and 17 of 42 (40%) underwent ovarian cystectomy. Patient factors associated with a higher rate of oophorectomy among the OT cases were older age (p = 0.03), higher parity (p = 0.007), and larger size of the affected ovary on imaging (p = 0.02). Having a laparotomy (p = 0.04) and surgeon subspecialty were also significantly associated with performance of oophorectomy in OT cases. Gynecologic oncologists were the primary surgeons for 5 of 54 (9.3%) of the cases and were more likely than generalists and other subspecialists to remove the affected ovary (p = 0.009).
Conclusion:
Older age, higher parity, larger size of the affected ovary on imaging, having a laparotomy, and having a gynecologic oncologist perform the surgery were significantly associated with a higher likelihood of oophorectomy in OT cases. Awareness of these clinical factors may ultimately reduce unneeded oophorectomy and promote ovarian-conserving surgery. (J GYNECOL SURG 37:236)
Introduction
Torsion of the ovary, tube, or both constitutes 2.7% of all gynecologic emergencies. 1 It generally occurs in women of reproductive age, 2 and common presenting signs and symptoms include abdominal/pelvic pain, nausea/vomiting, tachycardia, fever, and/or abdominal tenderness to palpation. 3 The diagnosis is made clinically based on patient history, imaging, and physical examination. Accurate diagnosis is made preoperatively in 44%–60% of cases.4,5 Delay or misdiagnosis can lead to adnexal necrosis and loss, peritonitis, thrombophlebitis, and rarely death.6–9 Current clinical management involves emergent laparoscopy in suspected cases. If ovarian torsion (OT) is noted intraoperatively, the surgeon must decide whether to detorse the ovary or perform an oophorectomy. An oophorectomy is often performed when the torsed ovary appears dusky in color and there is concern that the ovary is necrotic with irreversible damage. Numerous studies have shown that surgeon ability to determine necrosis based on the physical appearance of the torsed ovary is inaccurate.2,10 Studies of OT have shown that even in necrotic-appearing ovaries, function is preserved in 83%–100% of cases if detorsion is performed, suggesting that oophorectomy may be avoided in the majority of cases.2,11–16 This is important to consider, especially in premenopausal women, where retaining ovarian function has many benefits including decreasing the risk of heart disease, colon cancer, and osteoporosis.17,18 Given these data, we sought to determine whether there are clinical factors that increase a patient's likelihood of having an oophorectomy at the time of surgery in cases of OT.
Materials and Methods
Institutional review board approval was obtained. We performed a retrospective chart review of all patients who presented to the Boston Medical Center ED between January 1, 2009, and July 31, 2014, with a diagnosis of suspected OT by ICD-9 code. We identified a total of 69 charts. All patients who did not present to the gynecology service directly from the emergency room, who were 50 years of age or older, or who did not have surgery within 1 week of presentation were excluded from the study. Based on these criteria, we excluded 15 of the 69 patient charts obtained.
We collected both patient and surgical data from the remaining 54 charts. Patient data collected included age, race, gravidity, parity, BMI, history of tubal ligation and/or oophorectomy, and affected ovary size by imaging. Surgical data collected included time from presentation to surgery, surgical method employed, work shift when surgery occurred, intraoperative findings, pathology findings, estimated blood loss, and subspecialty of surgeon performing the case.
Odds ratios (ORs) and confidence intervals (95% CIs) were calculated for oophorectomy under various conditions. Statistical analysis using Fisher exact test (for discrete categorical data), t-test (for normally distributed continuous data), and Mann–Whitney U test (for continuous data that were not normally distributed) was performed to identify factors that were significantly associated (p < 0.05) with having oophorectomy at the time of surgery.
Results
Fifty-four charts of patients who presented to Boston Medical Center with a diagnosis of suspected OT were identified. Ninety-one percent (49 of 54) of patients underwent a laparoscopic procedure. Of the laparoscopic procedures, the primary surgeon converted from laparoscopy to an open procedure in two cases. The mean size of the affected ovary in the converted cases was 8.3 cm, and in the laparoscopic-only cases, it was 8.1 cm. The two laparoscopic cases were converted to laparotomy secondary to adhesions in both and bleeding in one case. Another 9% of patients (5 of 54) proceeded directly to an open abdominal procedure. The mean affected ovary size in the five primary laparotomy cases was larger at 13.6 cm (p = 0.003).
Overall, OT was identified in 78% (42 of 54) of cases of suspected OT, and 60% (25 of 42) of the patients with OT underwent oophorectomy. The remaining patients, 17 of 42 (40%), underwent ovarian cystectomy. The OR of having an oophorectomy in the setting of OT was 36.0 (CI 2.02–656.45; p = 0.0002). None of the 12 patients who did not have OT at the time of surgery had an oophorectomy. Table 1 gives the characteristics that were statistically associated with an increased likelihood of having an oophorectomy at the time of surgery. Older age (p = 0.03) was associated with a higher likelihood of oophorectomy. Patient ages ranged from 13 to 48 years in our study. The mean age of patients undergoing oophorectomy was 32 years, compared with 27 years in patients who did not undergo oophorectomy. A higher mean parity of 1.7 (p = 0.007) and larger mean size of the affected ovary on imaging of 9.7 cm (p = 0.02) were also associated with a higher likelihood of having oophorectomy at the time of surgery. If the surgery was completed laparoscopically, there was a lower likelihood of oophorectomy than primary laparotomy or laparoscopic converted to laparotomy (p = 0.04; OR 0.11 [CI 0.01–1.02]). There was a trend toward significance with a p-value of 0.18 of higher BMI patients (mean BMI of 29 kg/m2) undergoing oophorectomy compared with those who did not undergo oophorectomy (mean BMI 26 kg/m2). Longer time from ED presentation to surgery in patients who underwent oophorectomy (15 hours vs. 9 hours) also showed a trend toward significance with a p-value of 0.11. There was no difference in oophorectomy occurrence by race (p = 0.68), gravidity (p = 0.29), work shift when surgery occurred (p = 0.99), history of tubal ligation/oophorectomy (p = 0.66), or estimated blood loss (p = 0.73).
Characteristics of Patients with Ovarian Torsion Undergoing Surgical Management
OR, odds ratios.
Surgeon subspecialty of the primary surgeon was significantly associated with performance of oophorectomy in OT cases (p = 0.009). As shown in Figure 1, generalists performed the majority of OT cases. The oophorectomy rate was the highest among gynecologic oncologists (100%) and the lowest among family planning subspecialists (17%), as noted in Figure 2. All of the patients who underwent an oophorectomy had benign findings on pathology, with the majority being teratomas (36%) as shown in Figure 3. Interestingly, only 20% of the ovaries removed were noted to be necrotic on pathology.
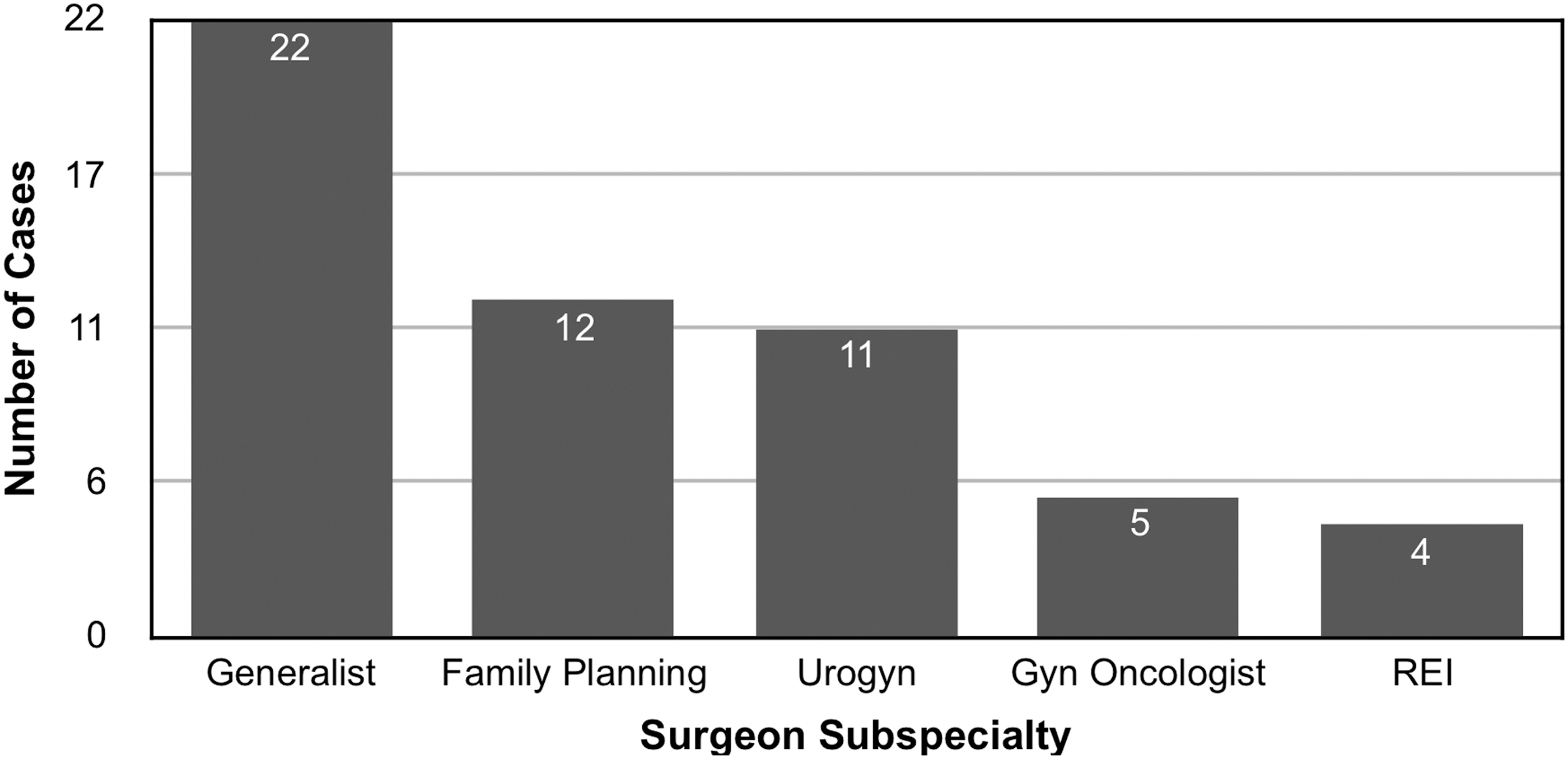
Torsion cases by surgeon subspecialty.

Percentage oophorectomies performed by surgeon subspecialty *p = 0.009.
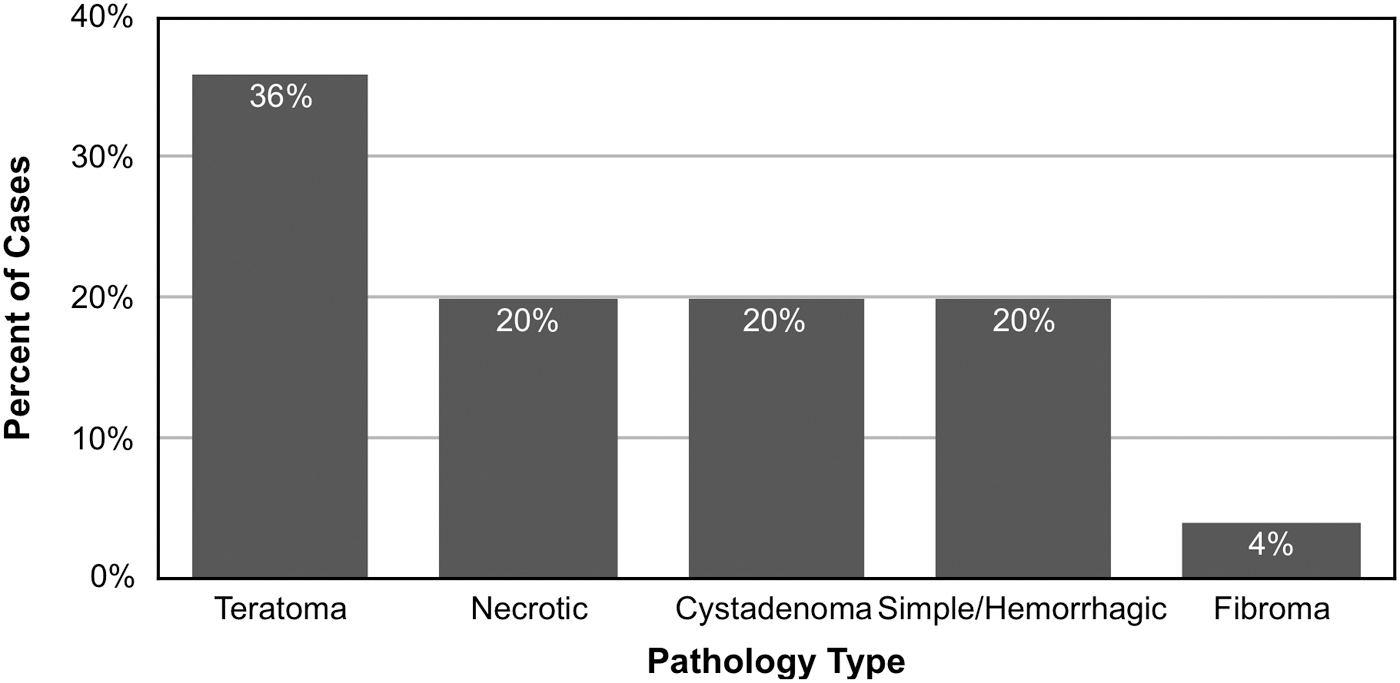
Pathology results in oophorectomy.
Discussion
We performed a retrospective study to determine clinical factors increasing the likelihood of oophorectomy at the time of surgery in patients with suspected OT. In our study, the accuracy of 78% in diagnosing OT preoperatively at our institution was better than in previous studies reporting rates of 44%–60%.4,5 The majority of suspected OT cases underwent laparoscopy (91%). Those who underwent open abdominal surgery had a significantly larger affected ovary on imaging (p = 0.003). Among the laparoscopic cases, there were only two conversions to laparotomy (4% or 2 of 49) secondary to adhesions and bleeding. Older patient age, higher parity, larger size of the affected ovary on imaging, having an abdominal procedure, and a gynecologic oncologist as primary surgeon were significantly associated with a higher likelihood of oophorectomy in our study. Race was not significantly associated with a higher likelihood of oophorectomy. This finding contrasts with a previous study by Mahal et al. that found that Hispanic and black race were associated with increased odds of inappropriate oophorectomy at the time of benign hysterectomy. 19 Our oophorectomy rate among OT cases was 60% compared with 53% reported in a pediatric OT study by Aziz et al. 11 As our study primarily comprised adult women, we would expect that the oophorectomy rate would be higher than in a pediatric study.
As noted in the pathology findings, only 20% of the ovaries removed were actually necrotic, consistent with the results of the Oelsner and Shashar study 2 that found that ovarian function is preserved in 88% to 100% of all OT cases. This suggests that surgeon ability to diagnose ovarian necrosis based on appearance of the ovary as the indication for oophorectomy is poor. Previous studies in pediatric patients with OT have shown that ovaries determined to be necrotic in appearance (“blue-black”) by the surgeon regained follicular function on postoperative ultrasonographs after detorsion.12,13 Studies of adult women who underwent detorsion also showed recovery of ovarian function with dominant follicles seen on ultrasonographs 15 as well as spontaneous pregnancies and successful IVF pregnancies from oocytes retrieved from previously detorsed ovaries. 16 Thus, there is a need to increase awareness that ovarian preservation in premenopausal women is an option in OT cases wherein the ovary appears dusky and loss of function is suspected. Also, retaining ovarian function has other nonreproductive benefits, including decreasing the risk of heart disease, colon cancer, and osteoporosis.17,18 In cases wherein oophorectomy is not performed, there may be an inclination to perform ovarian cystectomy. We found a rate of ovarian cystectomy of 40% (17 of 42) in our patient sample. However, the study by Oelsner and Shashar suggested avoiding cystectomy at the time of emergent surgery because the affected ovary may be edematous and friable, leading to bleeding at the time of cystectomy and possible unintended oophorectomy, and often the cyst is functional. 2 Their recommendation was to perform a cystectomy 4–6 weeks later if the cyst persists.
The strengths of our study include the racial diversity of our patient population, making our findings widely applicable, as well as our analysis of surgical factors external to the patient (time to surgery, subspecialty of primary surgeon). As with all chart review studies, the retrospective nature of our study increases the propensity for bias. Performing a multicenter prospective study with a larger number of patients may help to decrease some of these inherent biases.
In this study of oophorectomy in OT cases, we identified several patient and surgical factors significantly associated with increased performance of oophorectomy in the absence of ovarian neoplasia, including older patient age, higher parity, larger size of the affected ovary on imaging, having a laparotomy, and having a gynecologic oncologist perform the surgery. In conclusion, awareness of the clinical factors associated with a higher likelihood of oophorectomy in OT cases may help to reduce unnecessary oophorectomies in the future and thus improve the fertility and overall health of premenopausal women.
Footnotes
Author Disclosure Statement
W.K. serves as a research consultant for Abbvie; other authors have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this article.
Funding Information
No funding was received for this work.