
Abstract
Background:
A tubo-ovarian abscess is a potential late complication after hymenectomy for imperforate hymen, especially when complicated with hematosalpinx. Laparoendoscopic single-site (LESS) surgery for management of tubo-ovarian abscess after hymenectomy has never been reported.
Case:
A 17-year-old virgin girl without a menarchal flow was referred due to a large pelvic cystic mass. With a diagnosis of an imperforate hymen with right hematosalpinx, an uneventful hymenectomy was performed for this patient. Six weeks later, she presented with lower-abdominal pain and febrile morbidity.
Results:
Antibiotics administration was initiated with the diagnosis of a right tubo-ovarian abscess. After failed medical management, LESS surgery was performed. Under laparoscopic observation, a severe pelvic adhesion around swollen right adnexal tissue was noted. After extensive adhesiolysis, a right salpingo-oophorectomy was performed, and the patient's postoperative course was uneventful.
Conclusions:
After hymenectomy for imperforate hymen with hematosalpinx, careful follow-up should be done to detect any secondary ascending pelvic infection leading to a tubo-ovarian abscess. LESS surgery may be a feasible minimally invasive option for managing a tubo-ovarian abscess with potential cosmetic benefits.
Introduction
Imperforate hymen is the most common cause of obstructed genital outflow in women. 1 The accumulation of blood behind a closed hymen may form hematocolpos, potentially followed by hematometra and hematosalpinx. The typical presentation in adolescence is cyclical abdominopelvic pain and no external menstrual bleeding. 1
To create a patent tract for menstrual outflow, the procedure of choice generally involves either hymenotomy or hymenectomy.1,2 However, surgical opening of the hymenal tissue can permit bacteria newly introduced into the vagina to ascend the genital tract, leading to serious pelvic infections. 3
The initial conservative measure for this secondary infection after hymenal opening is antibiotics' administration. 3 However, if the infection is refractory to medical management, earlier interventions should be considered. 3
Laparoendoscopic single-site (LESS) surgery performed through an umbilical incision is now being increasingly applied in various gynecologic surgeries, including pediatric and adolescent surgeries, because of the potential cosmetic benefits. 4
However, the feasibility of this minimally invasive approach for the management of a tubo-ovarian abscess after hymenectomy for imperforate hymen had never been reported when the current authors performed a systematic English-literature search in Google Scholar and PubMed from 2009 to 2019, utilizing the search terms
This article herein reports on successful management of a tubo-ovarian abscess in a patient after a hymenectomy for an imperforate hymen with hematosalpinx by LESS surgery.
Case
A 17-year-old virgin girl without menstrual flow was referred due to a large abdominal cystic mass after consultation because of a worsening of her cyclic abdominopelvic pain lasting for more than 1 year. At initial presentation, her white blood–cell (WBC) count was 9000/μL and her C-reactive protein (CRP) value was 0.34 mg/dL.
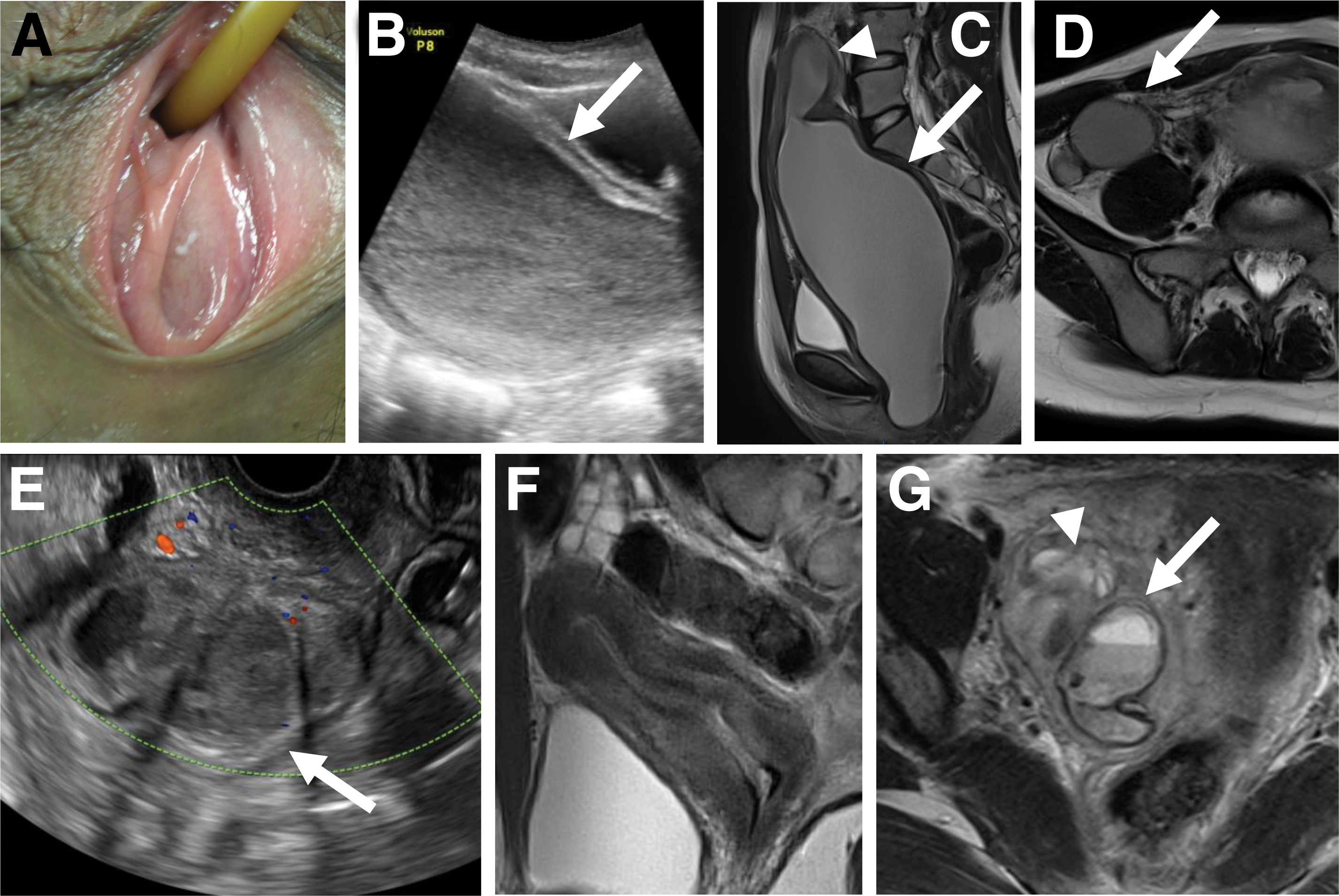
On a vulvar inspection, an imperforate hymen with a central bulge was identified (Fig. 1A). On ultrasonographic (USG) examination, a large cystic mass containing high-echoic fluid material was identified in her lower abdomen (Fig. 1B, arrow). On magnetic resonance imaging (MRI), prominent hematometra (Fig. 1C, arrowhead), hematocolpos (Fig. 1C, arrow), and right hematosalpinx (Fig. 1D, arrow) were identified.
With a diagnosis of an imperforate hymen, a hymenectomy was performed under spinal anesthesia. An initial cruciate incision was made using sharp dissection and needlepoint cautery, resulting in the flow of 600 mL of old blood that had accumulated in the vagina and uterine cavity. The redundant hymenal mucosa was excised, and the mucosal edges were reapproximated in an interrupted fashion. The early course after hymenectomy was uneventful. She was discharged from the hospital on postoperative day 3.
Her first menstrual flow occurred 4 weeks after the hymenectomy. Six weeks after the hymenectomy, however, she presented with febrile morbidity and severe right lower-abdominal pain. Blood testing revealed elevations in her CRP level (10.5 mg/dL) and WBC count (17,700/μL). Purulent vaginal discharge was identified.
On transvaginal USG, the uterus showed a normal appearance and multiple cystic lesions were noted in the right adnexal area (Fig.1E, arrow). On MRI, the uterine corpus showed normal architecture (Fig. 1F). In addition to a swollen ovary (Fig. 1G, arrowhead), the thickened wall of the luminal structure and fluid–fluid level change in the luminal contents indicated the presence of a tubo-ovarian abscess (Fig. 1G, arrow).
After admission, cefmetazole (3 g/day) was initially administered for 3 days. After identification of variety of gram-positive bacilli and cocci, and gram-negative bacilli in a vaginal culture, the antibiotic administration was changed to tazobactam/piperacillin (13.5 g/day), which was continued for another 7 days.
However, on the eighth day of her hospitalization, this patient's intermittent fever and right abdominal pain persisted. Then, urgent interventional management was planned. The patient and her parents were counseled about the treatment options. Informed consent was obtained to perform LESS surgery, 4 with possible conversion to multiport laparoscopy or laparotomy if the LESS approach failed.
Results
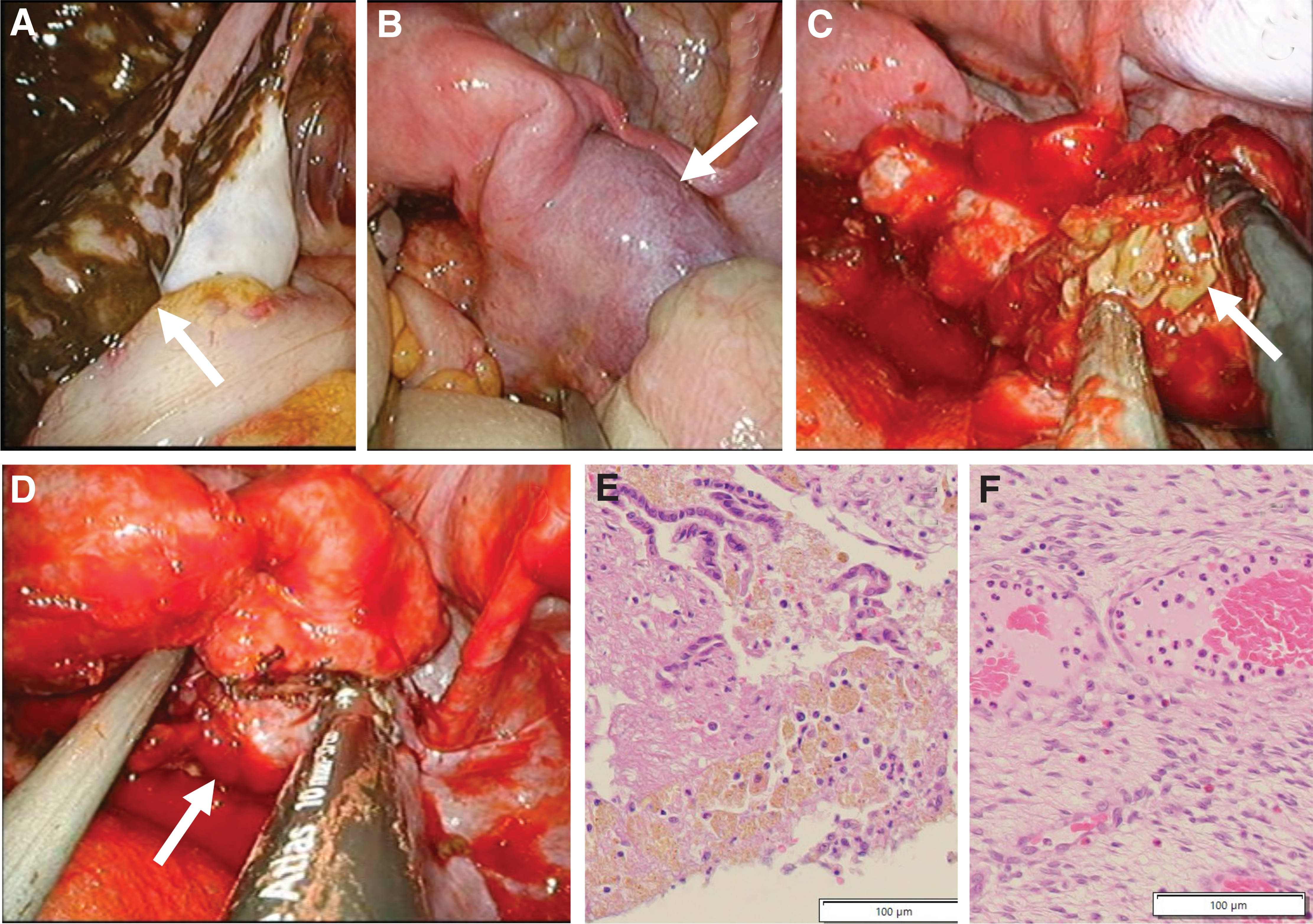
Under general anesthesia, LESS surgery was performed as previously described. 4 Under a laparoscopic view, a diffuse hemosiderin deposit on the peritoneal surface was noted. This hemosiderin deposit was more prominent on the left side (Fig. 2A, arrow) than on the right side (Fig. 2B). Marked swelling of the right fallopian tube was noted (Fig. 2B, arrow), and the right ovary was found to be involved in a severe adhesion (Fig. 2B).
Laparoendoscopic single-site surgery for right tubo-ovarian abscess after hymenotomy for imperforate hymen with hematosalpinx.
After blunt and sharp dissection of the adhesion around the right adnexal tissue, tubal contents containing yellowish pus were drained from the right tubal fimbriae (Fig. 2C, arrow). Due to severe inflammatory changes involving the adjacent ovarian tissue (Fig. 2D, arrow), the right adnexal tissue appeared to be difficult to preserve and was excised by sealing and cutting with a Ligasure Atlastm device (Covidien Japan, Tokyo, Japan; Fig. 2D). The excised tissue weight was 52 g, the surgical duration was 85 minutes, and the intraoperative blood loss was 200 mL. A bacterial culture of the drained pus did not yield any growth of bacteria. Pathologic examination of the fallopian tube (Fig. 2E) and ovary (Fig. 2F) showed severe inflammatory changes.
The patient's postoperative course was uneventful, and she was discharged from the hospital 7 days after this second surgery on confirming a decline in the inflammatory parameters. A regular menstrual flow was maintained, and neither recurrence of hymenal obstruction nor pelvic infection was noted 1 year after surgery.
Discussion
If imperforate hymen remains undetected and spontaneous opening of a closed hymen does not occur at pubertal estrogenization, 2 menarche can trigger significant problems.1–3,5 Retained menstrual blood initially accumulates in the vagina, causing a gradual dilatation from the hymen to the cervix; thereafter, hematometra develops, 1 and hematosalpinx can also be formed as a sequela of this process. 1
In the present case, hematosalpinx was observed only on the right side at the initial presentation. Under a laparoscopic view, an extensive hemosiderin deposit that was thought to be derived from retrograde backflow of the menstrual blood was observed around the left fallopian tube, although the deposit was less prominent on the right side.
This might have been because the right fallopian tube, which was suspected of being obstructed due to fimbrial adhesion sometime in the past, had accumulated refluxed menstrual blood inside the tubal cavity over a substantial period of time, eventually forming hematosalpinx only on the right side.
The definitive treatment with a favorable outcome for imperforate hymen is hymenotomy or hymenectomy.1,2 During the procedure, appropriate hemostasis and strict aseptic conditions are required, as Doederlein flora, which prevents ascending genital tract infection, are absent in vagina at this stage, and the retained blood can act as a good culture medium for pathogenic organisms. 2
Either hymenotomy or hymenectomy is a procedure with a sufficient safety record with a low rate of complications.1,2 However, even in cases in which procedures are performed carefully, intractable pelvic infection can occur unexpectedly after opening of the imperforate hymen on rare occasions. 3 Furthermore, especially in cases complicated with hematosalpinx, while a severe pelvic infection after hymenotomy can develop in the early postoperative period, 3 one should watch for a potential later development. This was found in the current case, in which a tubo-ovarian abscess occurred despite a careful check-up after the surgery.
Diagnostic and therapeutic procedures for tubo-ovarian abscesses in nonsexually active adolescent females5,6 are similar to those for common tubo-ovarian abscesses occurring in sexually active adult women. As shown in the present case, the initial imaging modality used to diagnose a tubo-ovarian abscess is USG, 6 which can identify masses involving an ovary and fallopian tube immediately.
In addition, in the current case, MRI played a significant role in diagnosing the tubo-ovarian abscess by providing information on the structure of the pelvic organs with superior resolution of the soft-tissue components.
In cases of tubo-ovarian abscesses in virgin adolescent girls,5–7 antibiotic therapy is a mainstay of initial treatment. However, if this medical management shows limited efficacy for reducing infectious morbidities, interventional managements—such as image-guided drainage,3,5,6 laparotomy, or laparoscopy 7 —are recommended, depending on the treating physician's experience with the procedures and the severity of the tubo-ovarian abscesses.
Laparotomy has conventionally been used to manage tubo-ovarian abscesses.6,7 However, with the recent development of surgical equipment and techniques, a laparoscopic approach has become a feasible option in selected cases. 5 Compared with conventional laparotomy, laparoscopic treatment has several advantages, including reduced postoperative pain, minimal trauma, and early postoperative recovery, especially in young girls. 8 In the conventional approach by laparoscopy, 8 multiple abdominal incisions are still required to place trocar ports for the insertion of surgical devices.
To provide the benefits of a minimally invasive approach by laparoscopy to young girls, LESS surgery, in which a single umbilical incision is used for surgical manipulation, has been introduced into clinical practice. 4 LESS surgery in pediatric and adolescent patients can have advantages over laparoscopy performed through multiple working ports. 4 For example, trauma to the abdominal wall can be minimized by reducing the number of ports, and a single incision that is eventually concealed in the umbilicus is a potential cosmetic benefit for young patients. 4
Conclusions
Imperforate hymen is commonly managed by hymenotomy or hymenectomy; however, careful postoperative observation is mandatory for the early detection of any secondary ascending pelvic infection, especially when complicated with hematosalpinx. LESS surgery may be a feasible minimally invasive option with potential cosmetic benefits for treating a tubo-ovarian abscess.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for preparation of this article.