
Abstract
Background:
Performing dissection of para-aortic lymph nodes (LNs) during radical hysterectomy is still optional and must be individualized. The clinical benefits of performing lymphadenectomy are not only for detection of occult metastases but it could positively affect the survival of patients.
Aim of the Study:
To assess the predictive clinical and pathologic parameters of occurrence of para-aortic LNs metastasis in early stage cervical cancer patients (stages I and II) in addition to evaluate of the effect of the extent of lymphadenectomy on patients' survival.
Patients and Methods:
We included 60 patients with cancer cervix stages I–II, we randomly divided them into the following: first group was managed by radical hysterectomy, dissection of both pelvic and para-aortic LNs and second group underwent radical hysterectomy with dissection of only pelvic LNs.
Results:
We found that presence of deep stromal and uterine body invasion, ovarian spread, presence of pelvic LN metastasis, and presence of gross enlargement of para-aortic LN were related to positive para-aortic LNs (p < 0.001). Patients with para-aortic LNs metastases have unfavorable disease-free survival (DFS) and unfavorable overall survival (OS) rates (p < 0.001). DFS and OS rates were more favorable in patients who underwent para-aortic lymphadenectomy than the other group who underwent only pelvic lymphadenectomy.
Conclusions:
Predictive factors for para-aortic LNs metastases in patients with early stage cervical cancer are presence of lympovascular invasion and pelvic LNs spread. Additionally performing para-aortic lymphadenectomy has survival benefits mainly in high-risk patients with higher stage and widespread pelvic LNs metastases. Clinical Registration Number, NCT03361730. (J GYNECOL SURG 37:205)
Introduction
Evaluation of the status of para-aortic lymph nodes (LNs) is important, as it is considered an important prognostic parameter for cervical cancer, particularly if it is clinically diagnosed in an early stage. 1 Pelvic lymphadenectomy has now become accepted as an essential procedure for the surgical management of cervical cancer patient stage IB1 to stage IIA1, whereas performing dissection of para-aortic LNs during radical hysterectomy is still optional and must be individualized, 2 this is because there is a wide variation in the incidence of para-aortic LNs metastasis in patients with cervical cancer who underwent radical hysterectomy with dissection of para-aortic LNs widely varies from 1.5% to 25%.3–5 The presence of para-aortic LNs invasion is a poor prognostic sign that negatively affects the survival of patients, but adjuvant chemotherapy and extended-field radiation are indicated that improves patients' prognosis. 1 Para-aortic LN involvement generally occurs as a consequence of widespread pelvic LN metastases. 4 In the recent modification of the International Federation of Gynecology and Obstetrics (FIGO) cervical cancer staging system, patients with metastases to para-aortic LNs that are radiologically or histopathologically proved are now considered to have stage IIIC2. 6 Although radiology could assess the status of para-aortic LN status to a high degree, 7 histopathologic confirmation of metastases to the LNs is the gold standard for evaluation, so a thorough lymphadenectomy with dissection of a huge number of LNs is needed for detection of apparent and occult metastatic disease accurately.8,9 The clinical benefits of performing lymphadenectomy are not only for detection of occult metastases, but it could also positively affect the survival of patients even in case of node-negative cases, which was previously found in many patients who underwent lymphadenectomy as a part of management of several cancers.10–12
To date, few data exist regarding analysis of predictive parameters of para-aortic LNs invasion in cervical cancer patients and that described advantages of routinely performing para-aortic lymphadenectomy in cervical cancer of early stage.
In this study, we aimed to assess the predictive clinical and pathologic parameters of occurrence of para-aortic LNs metastasis in early stage cervical cancer patients (stages I–II) who underwent radical hysterectomy with dissection of both pelvic and para-aortic LNs in addition to evaluation of the effect of the extent of lymphadenectomy on patients' survival in early stage cervical cancer patients by comparing the survival outcomes of patients who underwent radical hysterectomy, dissection of both pelvic and para-aortic LNs with patients who underwent radical hysterectomy with dissection of only pelvic LNs.
Patients and Methods
Patients
After receiving approval from the institutional review board of faculty of medicine, Zagazig University, we identified all patients with operable cancer cervix who underwent surgical management in the gynecology and obstetrics department and general surgery department faculty of medicine, Zagazig University. Cases were managed with radical hysterectomy pelvic lymphadenectomy with or without para-aortic lymphadenectomy in the period from January 1, 2016, to December 31, 2019. At time of hospital admission, patients signed written informed consents to allow using their medical information by the researchers for research purposes.
Inclusion criteria
Females with complete data in their records, with confirmed diagnosis of cancer cervix stages I–II according FIGO 2009 and who were managed with radical hysterectomy pelvic lymphadenectomy with or without para-aortic lymphadenectomy, were included.
Exclusion criteria
We excluded inoperable cases, cases with late stage who received preoperative neoadjuvant chemotherapy, cases who have synchronous malignancies at time of cancer cervix diagnosis, and women with insufficient number of dissected LNs (<10 pelvic and 5 para-aortic nodes).12,13 After application of the inclusion criteria, we included 60 patients with cancer cervix stages I–II and divided them using a computerized randomization into two equal groups: the first group was managed by radical hysterectomy, dissection of both pelvic and para-aortic LNs, and the second group of patients underwent radical hysterectomy with dissection of only pelvic LNs.
All operations were performed by a certified team that included surgical and gynecologic oncology team who performed radical hysterectomy with Piver's type III hysterectomy.
Para-aortic lymphadenectomy was performed by removal of the lateral aortic, preaortic, precaval, interaorticocaval, and lateral caval nodes till the left renal vein. Postoperative adjuvant therapy was used for patients with high and intermediate prognostic risk factors, such as large size of the tumor, positive LN, invaded surgical margins, invasion of the parametrium, lymphovascular invasion, and deep stromal invasion. Pelvic radiation at 40–50 Gy with or without concurrent cisplatin-based chemotherapy was individually offered. Extended field irradiation was taken in case of positive para-aortic LNs and chemotherapy was taken in cases of rejection of radiotherapy.
For all included patients, we have collected clinical, pathologic, and follow-up data such as age of the patient, size of the tumor, histopathologic subtype, presence of invasion of the vagina, uterine body, parametrium, ovaries, number of removed LNs, and number of positive pelvic and para-aortic LNs.
To assess the association between the extent of lymphadenectomy and patients survival, we stratified patients according to total number of dissected LNs into four groups: <10 LNs, 11–20 LNs, 21–30 LNs, and >30 LNs. Then we performed separate analyses for patients with either LN positive or LN negative.
The vital status of each patient was recorded. We recorded follow-up data as disease progression, recurrence, metastases, and survival rates. Follow-up data were collected and correlated with dissected and positive LNs to detect survival benefits of the extent of lymphadenectomy.
Results
Clinicopathologic data of included study population are detailed in Table 1.
Association Between Clinical Pathologic Parameters and Para-Aortic Lymph Nodes Metastases in Patients Who Underwent Para-Aortic Lymphadenectomy
Cth, chemotherapy; LNs, lymph nodes; LVSI, lympho-vascular invasion; Rth, radiotherapy; SCC, squamous cell carcinoma.
The patients' age at surgery ranged from 23 to 81 years with mean patients age = 57.8 ± 8.1 year.
Thirty patients underwent radical hysterectomy, bilateral salphingo-oophorectomy, pelvic lymphadenectomy, and para-aortic lymphadenectomy, whereas the remaining 30 patients underwent radical hysterectomy and bilateral salphingo-oophorectomy with only pelvic lymphadenectomy.
We found that larger size of the tumor (p = 0.043), higher grade of the tumor, advanced clinical stage (stages IB–II), presence of deep stromal invasion, invasion of the lymphovascular space, invasion of the parametrium, uterine body invasion, vaginal invasion, ovarian spread, presence of gross enlargement and histopathologic confirmation of pelvic LN metastasis, presence of gross enlargement of common iliac LN, and presence of gross enlargement of para-aortic LN were related to histopathologically confirmed positive para-aortic LNs (p < 0.001) (Tables 1–3 and Fig. 1).
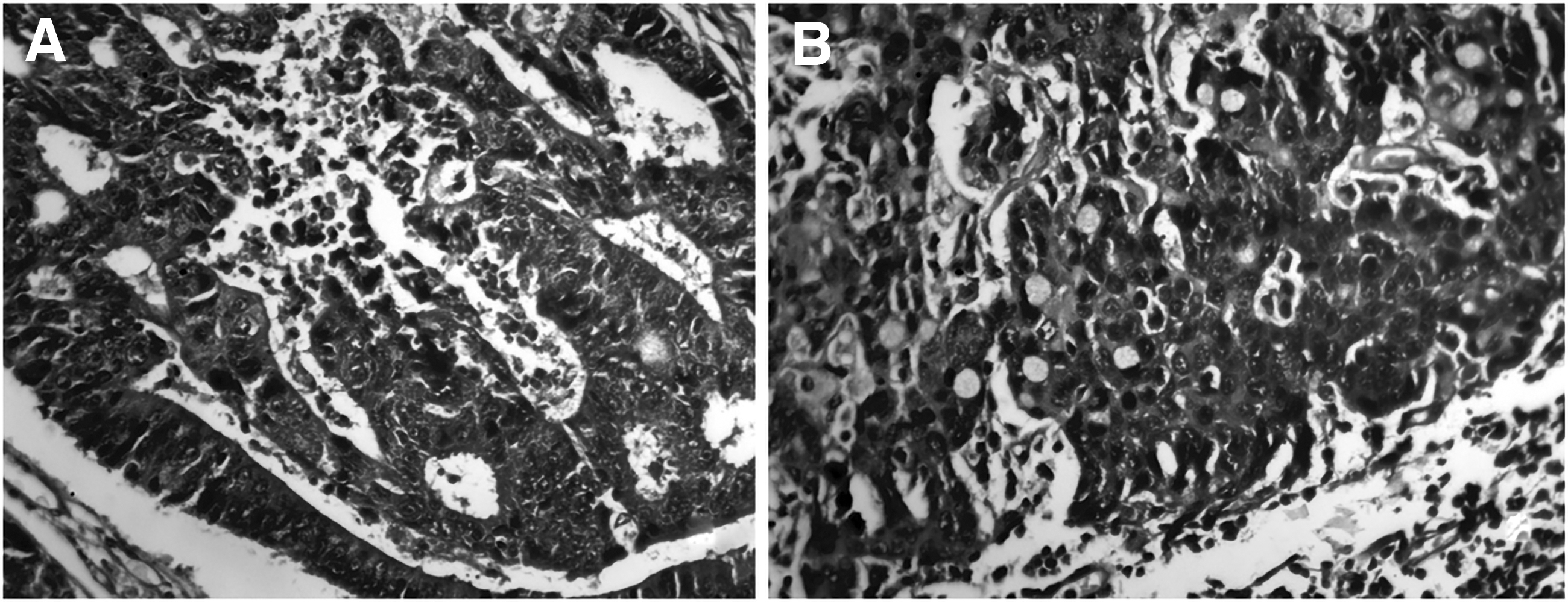
Histopathologic features of early cervical carcinoma.
Association Between Disease Progression, DFS Rate, and OS Rate in Patients Who Underwent Para-Aortic Lymphadenectomy
CI, confidence interval; DFS, disease-free survival; OS, overall survival.
Multivariate Analysis of Predictive Factors of Pathologically Confirmed Para-Aortic Lymph Nodes Metastases in Patients Who Underwent Para-Aortic Lymphadenectomy
HR, hazard ratio; Sig, significant; #########, insignificant values.
We found no statistically significant role of type of treatment in predicting para-aortic LNs metastases.
Follow-up, progression, and survival outcomes are given in Tables 4 and 5 and Figures 2 and 3.
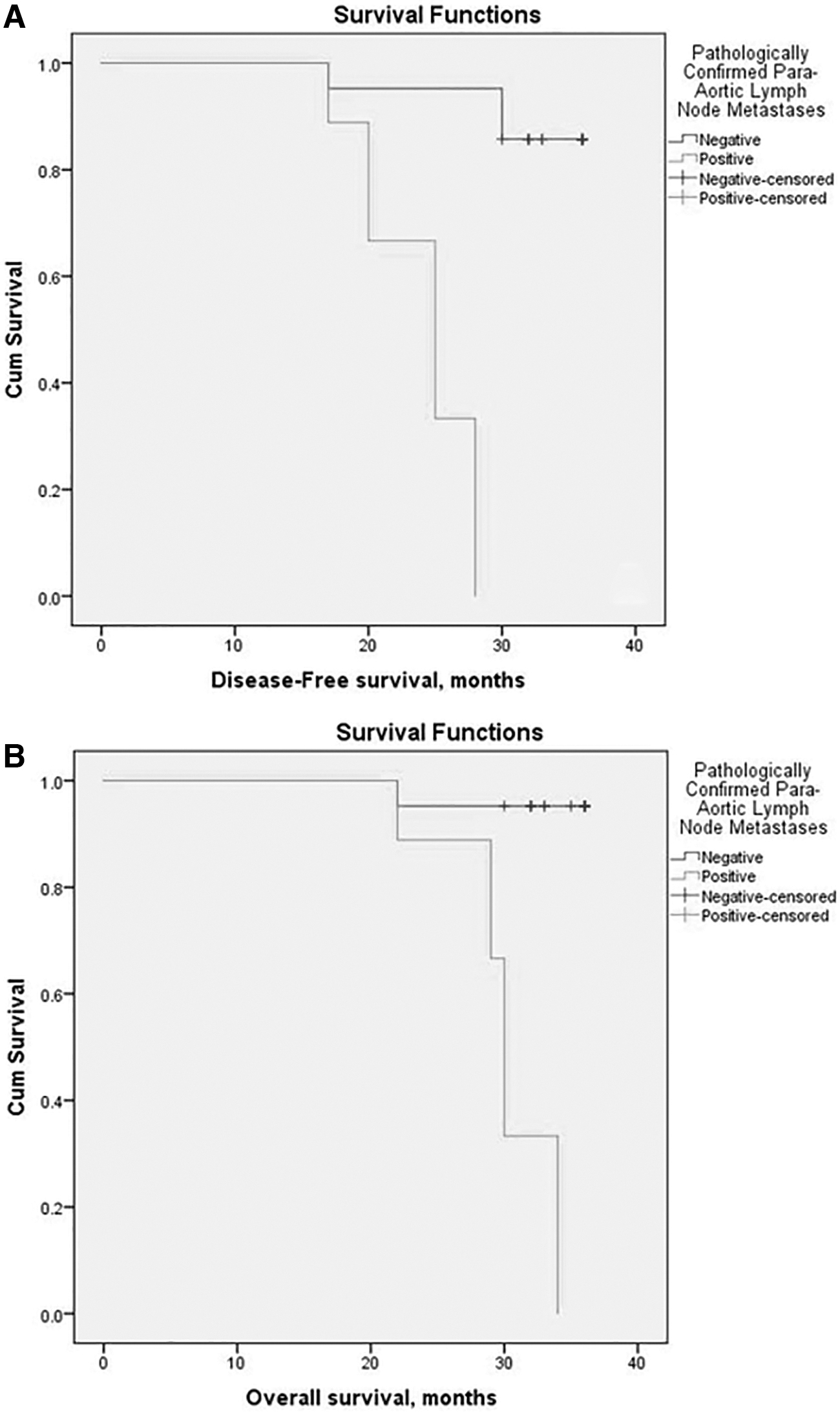
Kaplan–Meier survival curves of the first group of patients who underwent total abdominal hysterectomy, pelvic lymphadenectomy, and para-aortic lymphadenectomy
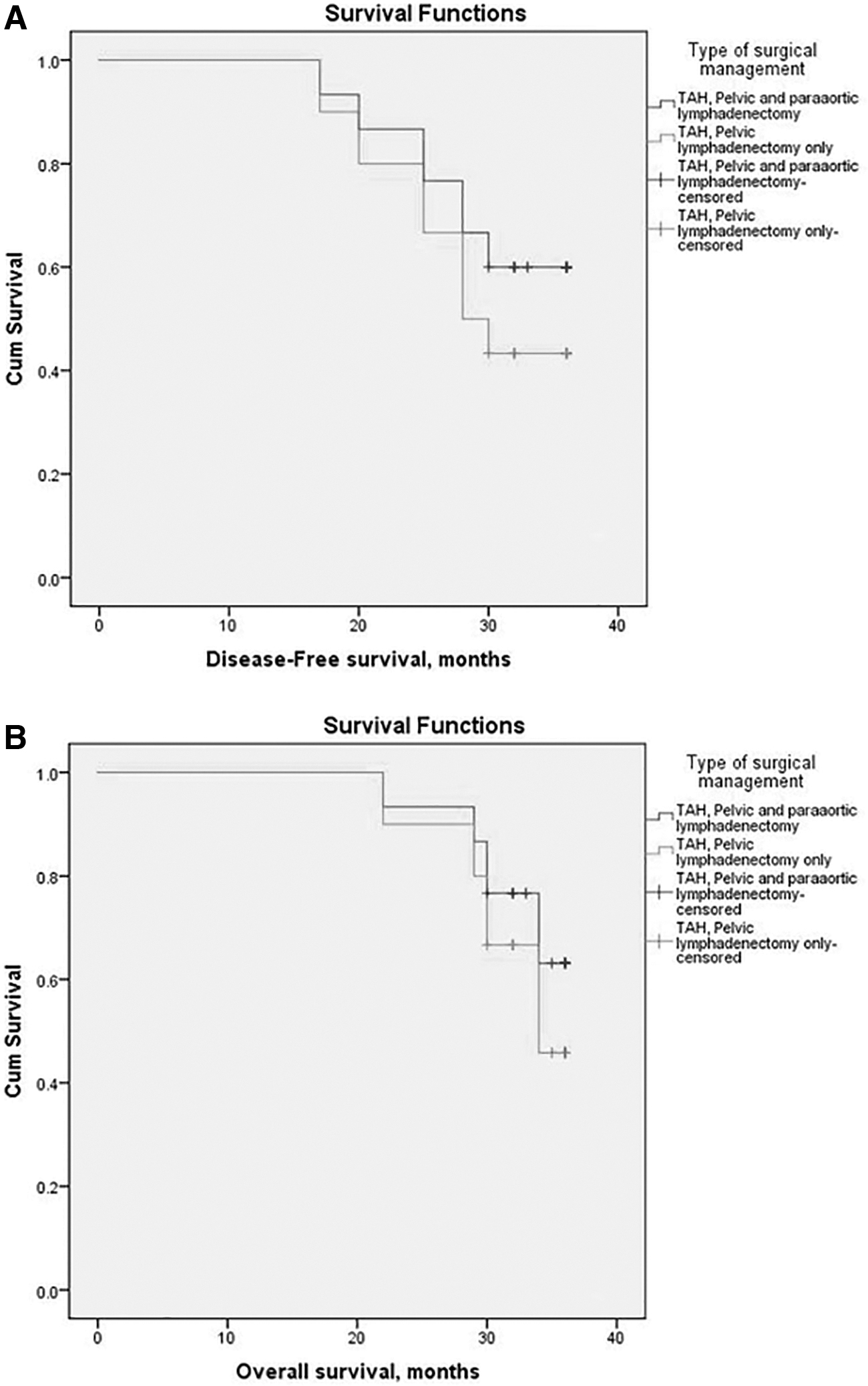
Kaplan–Meier survival curves of patients who underwent total abdominal hysterectomy, pelvic lymphadenectomy, and para-aortic lymphadenectomy and patients who underwent total abdominal hysterectomy and pelvic lymphadenectomy only
Correlations Between Patients Who Underwent TAH, Pelvic Lymphadenectomy, and Para-Aortic Lymphadenectomy and Patients Who Underwent TAH and Pelvic Lymphadenectomy Only Regarding Clinical and Pathologic Parameters
TAH, total abdominal hysterectomy.
Correlations Between Patients Who Underwent TAH, Pelvic Lymphadenectomy, and Para-Aortic Lymphadenectomy and Patients Who Underwent TAH and Pelvic Lymphadenectomy Only Regarding DFS Rate and OS Rates
NR, no response.
Patients with histopathologically confirmed para-aortic LNs metastases have higher incidence of disease progression, recurrence, unfavorable disease-free survival (DFS), and unfavorable overall survival (OS) rates (p < 0.001).
We correlated patients cancer-related mortality with lymphadenectomy extent particularly para-aortic lymphadenectomy and found that patients who underwent para-aortic lymphadenectomy have fewer incidences of disease progression, recurrence, favorable progression-free survival, and OS rates. DFS rate and OS rate were more favorable in patients who underwent para-aortic lymphadenectomy than the other group who underwent only pelvic lymphadenectomy, but the differences between both groups are statistically insignificant.
Discussion
In the first group of patients who underwent radical hysterectomy with pelvic lymphadenectomy and para-aortic lymphadenectomy, we found that older age of the patients, higher grade of the tumor, advanced clinical stage, large tumor size, presence of deep stromal invasion, invasion of the lymphovascular space, invasion of the parametrium, uterine body invasion, vaginal invasion, ovarian spread (p < 0.001), presence of pelvic LN metastasis, and common iliac LN metastasis were related to positive para-aortic LNs. Ayhan et al. 1 showed nearly similar results. It was previously reported that the rate of spread to the para-aortic nodes widely varied and it ranged from 1.6% to 24.1% according to sample size.4,5 We showed a rate of involvement of the para-aortic LNs similar to previous studies.1,14,15
In addition, we stated that pelvic LNs metastases are important predictive factors for para-aortic LNs spread, and we showed that nearly all patients with positive para-aortic LNs spread have pelvic LNs invasion, similarly previous studies reported that all patients with positive para-aortic LNs had pelvic LNs metastasis.3–5,16
Tsuruga et al. 14 and Huang et al. 17 showed that 92.3% and 94.7% of included para-aortic LNs had pelvic positive LN metastasis, respectively.
Ayhan et al. 1 showed that 91.6% of included women have positive pelvic LN metastasis. Differences in rate of metastases to the para-aortic LNs could be due to inadequate dissection or inaccurate histopathologic evaluation of sent samples.15,17Although positron emission tomography–computed tomography were widely applied for nodal status assessment in cervical cancer patients, there are high rates of reported false-negative results for involvement of the para-aortic LNs. 18 These false-negative results are due to failure of micrometastasis detection by using imaging techniques. 19
Histopathologic confirmation of positive LNs metastases is the gold standard for evaluating para-aortic LNs status. 15 Sentinel LNs biopsy was highly suggested for most of gynecologic cancers and it is particularly recommended for early stage cervical cancer if tumor size was <2 cm. 2 Para-aortic LNs metastases are very low in patients with cancer <2 cm, reaching about 4%. 1 So sentinel LNs biopsy and examination have no values in cervical cancer patients and there is a real need to detect predictive parameters of para-aortic LNs metastases in cervical cancer. 6
We showed that more extensive lymphadenectomy has therapeutic advantages by removing many LNs that allow adequate histopathologic evaluation, detecting micro-metastases, decreasing disease recurrence, and improving patient survival.
Shah et al. 10 showed the same results in cervical cancer patients that removal of huge number of LNs improves survival of patients with histologically confirmed negative para-aortic LNs but has no effects on patients with positive LNs.
The prognostic values of performing extensive lymphadenectomy in cancer patients with histopathologically negative LNs metastases have been proved in many solid tumors.11,12 As pelvic lymphadenectomy and para-aortic lymphadenectomy lead to some sorts of morbidity, it is important to adequately assess the therapeutic advantages of performing them and carefully assess against their morbidity.
Conclusions
There are many predictive factors for para-aortic LNs metastases in patients with early stage cervical cancer such as age of the patients, tumor size, presence of lympovascular invasion, and pelvic LNs spread, additionally we concluded that performing para-aortic lymphadenectomy has survival benefits mainly in high-risk patients with higher stage and widespread pelvic LNs metastases; those patients presumably had microscopic para-aortic LNs metastases. The risk factors for undetected microscopic disease are the presence of positive pelvic nodes.
Further studies are needed to determine the number of dissected paraaortic lymph nodes that is needed to confirm their survival advantages and allow making evidence-based about degree of adequate lymphadenectomy.
Points of strengths of our study
We included only patients with early cervical cancer and followed them for ∼3 years to assess the predictive factors for positive para-aortic LNs; moreover, we compared patients who underwent para-aortic lymphadenectomy with patients who did not allow us to detect the survival advantages of performing para-aortic lymphadenectomy.
Limitations and points of weakness
The relatively small number of patients in either of the groups makes some of the results statistically insignificant. Moreover the short time of the follow-up period could not allow more confirmation of the results.
There was a selection bias for performing para-aortic nodes to the patients who had >4 cm size tumors (24 vs.13)
Recommendations
We recommend performing para-aortic lymphadenectomy in all cases of early cervical carcinoma, but further studies including large number of patients with longer follow-up time are needed to assess survival benefits and values of para-aortic lymphadenectomy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this work.