
Abstract
Objective:
Second uterine carcinosarcoma (UCS) occurs in <1% of patients after >5 years of treatment with concurrent chemoradiotherapy (CCRT) for cervical cancer. Surgical staging with lymphadenectomy is the mainstay of management that is largely done by the laparotomic approach. A Medline search for treatment of uterine carcinosarcoma after radiotherapy for cervical cancer was done using terms “uterine carcinosarcoma,” “radiotherapy for cervical cancer,” and “second primary uterine cancer,” there is no case report or literature wherein UCS is treated by laparoscopy.
Case Report:
We present the first documented case of UCS diagnosed in a 72-year-old lady after 11 years of CCRT for cervical cancer stage 1B2, managed by laparoscopic staging wherein washing cytology, total hysterectomy, and bilateral salpingoophorectomy with pelvic and para-aortic lymphadenectomy were done.
Conclusion:
Minimal invasive surgical approach for surgical staging of irradiation-induced UCS may become a useful surgical option even in advanced stage in the era of minimally invasive surgery, offering advantages such as lower intraoperative blood loss, less need of transfusion, and shorter hospital stay with probably improved survival.
Introduction
Concurrent chemoradiotherapy (CCRT) is a mainstay of the treatment for bulky and locally advanced cervical cancer. However, treatment with radiotherapy (RT) has been found to be an important predictor that increased the risk of second cancer in cervical cancer survivors. 1 They have 80% increased risk to develop a second malignancy when compared with the general population. Uterine carcinosarcoma (UCS) has been the mostly reported second malignancy in patients treated with RT for cervical cancer. 2 This occurs in <1% of patients after >5 years of treatment with CCRT for cervical cancer. For the management of UCS, besides stage IV disease that warrants palliative care in general, the primary management is surgery for both staging and initial treatment. 3
The mode of surgery in most of the reports of management of UCS is through laparotomy. We present, for the first time, laparoscopic surgical staging that includes washing cytology, total hysterectomy, and bilateral salpingoophorectomy with pelvic and para-aortic lymphadenectomy done for management of a 72-year-old lady with UCS, diagnosed 9 years after CCRT for cervical cancer stage 1B2. Informed consent was taken from the woman for case report, and ethical clearance was provided by the institutional review board of Chang Gung Medical Foundation.
Case Descriptions
A 72-year-old P5L5 woman, with menopause at the age of 55 years, was in regular follow-up at the outpatient clinic of Chang Gung Memorial Hospital, Linkou, Taiwan, since 9 years. She was diagnosed as having squamous cell cancer of cervix stage IB2 as per the 2009 International Federation of Gynecology and Obstetrics (FIGO), 9 years back in October 2011, for which she had undergone uneventful CCRT management. Since then she was being followed up with yearly cervical Pap smear, imaging study, and tumor markers that were within normal limits until December 2019, when her serum level of CA125 was raised to 238.6 units/mL. There was no vaginal bleeding or other systemic complaints. But pelvic examination revealed cervical atrophy with tender uterus and adnexae and a free parametrium. Transvaginal sonography showed hydrocorpus with internal solid mass with normal adnexae as shown in Figure 1. Magnetic resonance imaging (MRI) showed distended endometrial cavity with mass lesion of 4.2 cm in the low uterine segment (Fig. 2). No evidence of other mass lesions in the abdominal visceral organs and lymphadenopathy was noted in MRI except for atrophy and synechiae of the cervix. So MRI was highly suspicious of primary endometrial or UCS with hydrometra. Tumor board conference suspected a second primary endometrial cancer or sarcoma postirradiation. With this impression she underwent operative laparoscopy with primary port through the Lee–Huang point. 4 Intraoperatively uterus was enlarged as 12 weeks gestation size. Washing cytology followed by total laparoscopic hysterectomy and bilateral salpingoophorectomy with bilateral pelvic and para-aortic lymphadenectomy below the inferior mesenteric artery was done. All specimens were removed vaginally after placing in endobag after draining out the hydrometra. Intraoperative blood loss was 100 mL. Total surgery time was 110 minutes. Gross specimen examination revealed uterine hydrocorpus with friable necrotic tissue growth noted of endometrial origin at the lower part of the uterus as shown in Figure 3. Frozen section biopsy of endometrium favored carcinosarcoma. Frozen section was done to rule out if this is endocervical cancer as this will change further management. Later fixed section biopsy confirmed endometrial carcinosarcoma with 75% myometrial invasion. There was also evidence of lymphovascular invasion to the right ovary and right fallopian tube with 80% depth of invasion by extension to the cervical stroma. Left pelvic and para-aortic lymph nodes also showed metastasis. So the final diagnosis was endometrial carcinosarcoma, tumor–node–metastasis classification was T3aN2mi. Postoperatively she had uneventful course and was discharged on fifth postoperative day. Currently she is under chemotherapy and had received fifth cycle of chemotherapy with paclitaxel and carboplatin, which was well tolerated. Our plan is to complete six cycles of chemotherapy and follow-up her.
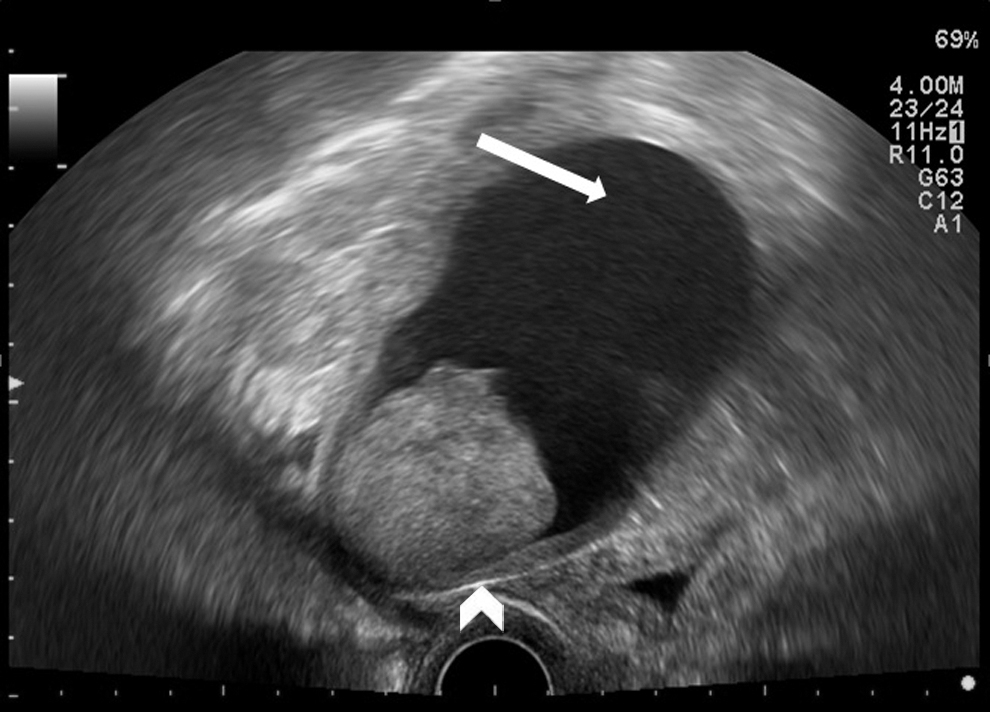
Transvaginal sonography shows hydrocorpus (white arrow) with internal solid mass (arrowhead).

T2-waited magnetic resonance imaging showed distended endometrial cavity (solid black arrow) with mass lesion of 4.2 cm in the low uterine segment and a small growth in the fundal area (arrowheads).

Cut section of uterus shows endometrial friable growth from lower endometrium. Previous primary cervical malignancy (white arrowhead).
Discussion
Carcinosarcoma of the female reproductive system often represents a highly aggressive neoplasm that is characterized by a mixture of malignant epithelial and stromal elements comprising carcinomatous and sarcomatous neoplastic cells. 5 They are rare tumors that account for <5% of all uterine malignancies for which the optimal adjuvant management has not been fully established. The endometrium is usually the primary site. 6 UCS presents similarly to other uterine adenocarcinomas.
Most commonly a patient with UCS is postmenopausal with bleeding, abdominal pain, and uterine enlargement. Elevated preoperative CA125 levels have been shown in a single institution study of 54 patients with UCS to be associated with extrauterine disease and deep myometrial invasion as we also found in index case. 7 Radiation-induced UCS tends to be of high grade, higher stage, and with high-risk histologic subtypes, indicating that these tumors differ from sporadic endometrial carcinomas with poorer prognosis. 8 The recurrence rate also tends to be higher for this type of UCS. In general, for women with evidence of stage IV disease, treatment is palliative. For all other patients, the primary management of carcinosarcoma is surgery for both staging and initial treatment. 3 This is a rare histologic type, for which the optimal adjuvant management has not been fully established. Literature search reveals staging laparotomy for early stage of disease as well as neoadjuvant chemotherapy followed by staging laparotomy for advanced disease. 9
Minimal invasive approach has been described for early stage of disease with equal survival and recurrence rate. 10 A Medline search for treatment of uterine carcinosarcoma after RT for cervical cancer revealed that there is no case report or literature wherein UCS is treated by laparoscopy, so we can say this is the first case. Most of the reported cases of radiation-induced UCS are managed by the laparotomic approach for surgical staging.11,12 A recent retrospective review done by Wakayama et al. among 313 cervical cancer patients with stage IB to IVA, treated with CCRT, found 3 cases (0.96%) with a second uterine corpus malignancy after CCRT. Among these patients, two patients received abdominal surgery and one patient received supportive care. 13 Probably because of rarity and technically difficult nature of laparoscopic surgery in UCS, it has not been described or reported in the literature.
The high recurrence rate and poor overall survival for UCS suggest the need for improved management strategies. Use of minimal invasive approach even in advanced stage may lead to improvement in survival compared with laparotomy for surgical staging. Although further accumulation of cases is needed, the minimal invasive surgical approach for surgical staging of irradiation-induced UCS may become a useful surgical option even in advanced stage in the era of minimally invasive surgery, offering advantages such as lower intraoperative blood loss, less need of transfusion, and shorter hospital stay with improved survival.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.