
Abstract
Objective:
The study aim is to determine reasons for cancellation of scheduled gynecologic surgeries.
Design:
This is a retrospective study of 760 patients.
Materials and Methods:
Predictor variables were from the domains of demographics (age, race/ethnicity, body mass index, and health insurance), chronic health conditions (diabetes and hypertension), surgical related (surgery type, surgery performed, preoperative diagnosis, and rescheduled), and timeline (day of week and season of year). The outcome was cancellation of gynecologic surgery.
Results:
The variable of rescheduled surgical procedures measured as either no or yes statistically differed (p < 0.001), where there was a greater percentage for “yes” rescheduled surgical procedures in the “yes cancellation” group (97.0%, n = 163) as compared with the “no cancellation” group (0.0%, n = 0). None of the demographics, chronic health conditions, and timeline variables statistically differed between the “no cancellation” and “yes cancellation” groups. Cancellation reasons included “patient” (46.4%, n = 78), “hospital” (37.5%, n = 63), and “unknown” (16.1%, n = 27).
Conclusion:
Our study found that the most common reasons for cancellations were patient related. We recommend that physicians assure that patients are sufficiently counseled before surgical scheduling regarding the importance of the surgery and necessary steps to proceed with the surgery such as presurgical testing and medical clearance. (J GYNECOL SURG 37:308)
Introduction
Surgery cancellations have a financial impact of increased costs, decreased efficiency, and insufficient utilization of employees and hospital resources.1,2 Repeat cancellations also negatively impact patient satisfaction and employee morale. 1 Surgery cancellation rates for all specialties range from 1% to 40%.1–4 In gynecology, surgery cancellation rates range from 2.5% to 3.9%.1,2
Surgery cancellation reasons can be classified as factors related to patients and to hospitals. One study of over 60,000 scheduled surgeries found that nearly half of all cancellations were by patient request. 2 Another large study of orthopedic patients reported similar findings with one-third of all scheduled surgeries cancelled by patient request, where half of these requests were due to desire for an earlier date, later date, or decision to forego surgery, and the remaining requests were related to family, work, or social reasons. 5 However, other studies of surgery cancellations found that hospital-related factors due to reduced surgical time or personnel and failure to complete preoperative assessment are more important for understanding surgery cancellations.3,4
Patient-related factors include demographics and chronic health conditions. For demographics, there are mixed findings with regard to age. One study reports that surgery cancellations are greatest among patients of age 80 years and above, 2 whereas another study observed the highest percentage of surgery cancellations for pediatric surgery. 6 Observed surgical cancellation rates are also reported to be unaffected by age. 7 Although we are unaware of any literature that identifies race or ethnicity impacting surgery cancellation, Hispanics and blacks are more likely to not attend their outpatient clinic appointments. 8 In addition, surgery cancellations are more common in patients with public health insurance than in those with private health insurance. 7 When considering body mass index (BMI), one report shows more surgery cancellations in obese patients with BMI from 35 to 39.9 kg/m2 than other obese categories and nonobese patients, 9 and greater than three-quarters of surgeons postpone elective surgery for obese patients. 10 As chronic health conditions, both diabetes 6 and hypertension6,11 are each associated with increased surgery cancellations.
Hospital-related factors include surgical-related and timeline variables. For urogynecologic surgery, patients scheduled for major cases are less frequently cancelled as compared with those scheduled for minor cases. 12 Also, patients with a malignant preoperative diagnosis have less surgery cancellations than patients with benign surgical indications. 13 For plastic surgery procedures, one large study found that even though more than 80% of scheduled procedures were elective, only 5% cancellations were observed with 42% attributed to patient-related reasons. 14 Timeline-related factors include cancellation based on day of the week where cancellations are greater on Mondays due to the “Monday effect” of a backlog of administrative affairs and staff fatigue on Mondays after the weekend 4 or at the end of the week 12 by patient preference. Another timeline-related factor is season of the year where some report more elective surgery cancellations during the winter than during fall, spring, and summer, 13 whereas others report no relationship of season with elective surgery cancellation.2,6
Although demographics, chronic health conditions, surgical related, and timeline factors are studied for their association with general surgery cancellations, to our knowledge there is only one study investigating the hospital-related factor of major versus minor surgery for urogynecologic surgery cancellations. 12 In this study, predictors of demographics (age, race, marital status, and education), chronic health conditions (liver or renal disease, diabetes, obesity, and coronary artery disease), surgical (prior surgery and major versus minor procedure scheduled), and timeline (day of the week) were included. 12 Our study investigates factors that impact cancellation of elective gynecologic surgery. We include predictors from demographics, chronic health conditions, surgical related, and timeline factors, and add additional potentially relevant demographic variables of BMI and health insurance status, surgical-related variables of surgery performed, preoperative diagnosis, rescheduled status, and timeline variable of season of the year. Our study investigates reasons for surgical cancellations and is limited to female patients. Our study focus on females may account for findings that differ from similar studies of general surgery cancellations because gynecologic surgery only serves a female population with an emphasis on reproductive health.
Materials and Methods
Setting
This is a retrospective study from a sample of 760 consecutive patients scheduled for gynecologic surgery from January 3, 2018, through November 28, 2019, at a single institution. Surgeries were scheduled at a suburban New York City safety-net hospital that typically serves immigrant patients of low socioeconomic and educational status. Inclusion criteria were women scheduled for gynecologic surgery. Exclusion criteria were women who received emergent gynecologic surgery without a scheduled surgery date and seven scheduled patients with incomplete information. Only the first scheduled case was included for the 20 patients with more than one surgery performed during the study period. Ethical approval was received from the hospital institutional review board to conduct this study.
Variables
The outcome variable was gynecologic surgery cancellation (no, yes). Predictor variables were (1) demographics of age (years), race/ethnicity (white, black, Hispanic, and Asian), BMI (kg/m2) as both continuous and categorical variables as defined by underweight and normal (17.00–24.99), overweight (25.00–29.99), class 1 obesity (30.00–34.99), class 2 obesity (35.00–39.99), and class 3 obesity (≥40.00) [the six underweight patients with BMI from 17.00 to 18.49 kg/m2 were included in the normal BMI group], and health insurance (private, public, and self-pay); (2) chronic health conditions of diabetes (no, yes) and hypertension (no, yes); (3) surgical related to surgery type (minor and major) (Table 1), indication for surgery (elective [bilateral tubal ligation, essure, and perineoplasty], nonelective [all surgeries other than elective]), surgery performed (no, yes), preoperative diagnosis (malignant and benign), and rescheduled (no, yes); and (4) timeline of day of week (Monday/Tuesday, Wednesday, Thursday, and Friday) [the five cases on Tuesday were added to Monday], and season (Winter [December, January, and February], Spring [March, April, and May], Summer [June, July, and August], and Fall [September, October, and November]). We also recorded the reasons reported in the medical records for cancellation that were then grouped into patient-related, hospital-related, and unknown reasons. Patient-related reasons consisted of patient changed her mind, pregnancy, social issues, illness, no-show to presurgical testing, no-show to surgery, and patient wanted to reschedule. Hospital-related reasons consisted of cancellations by surgeon, lack of medical clearance, cancellation by the anesthesiologist, financial/insurance reasons, patient no longer needed surgery, and lack of required resources.
Descriptive Statistics for Major and Minor Surgeries
EUA, examination under anesthesia; TVT, tension-free vaginal tape.
Statistical analysis
Descriptive statistics of mean and standard deviation were calculated for the continuous variables. Frequency and percentage were calculated for the categorical variables. Analysis of variance compared the continuous variables. The Pearson chi square statistic compared the categorical variables. All variables statistically significant in these univariate analyses were analyzed in a multivariate logistic regression analysis. The Firth logistic regression analysis was used due to cells with a zero value. 15 IBM SPSS Statistics Version 2516 and Stata SE Version 1517 were used for the analyses. All p-values were two tailed. Alpha level was p < 0.05.
Results
The observed surgery cancellations were 168 of the 760 total cases scheduled (22.1%) for our study period. Table 2 gives the comparisons between the gynecologic surgery “no cancellation” and “yes cancellation” groups. Surgery type statistically differed where there was a greater percentage of those with major surgery in the “no cancellation” group than the “yes cancellation” group (p = 0.004). Surgery indication statistically differed where there was a greater percentage of those scheduled for elective surgery in the “yes cancellation” group than the “no cancellation” group (p = 0.005). All surgeries (100.0%) in the “no cancellation” group were performed, whereas only 88.1% of surgeries in the “yes cancellation” group were ultimately performed (p < 0.001). The observed percentage of rescheduled surgeries was statistically significant when comparing the “no cancellation” group that required no rescheduled surgeries with 97.0% of cancelled surgeries that were rescheduled in the “yes cancellation” group (p < 0.001). None of the demographics, chronic health conditions, and timeline variables statistically differed between the “no cancellation” and “yes cancellation” groups. The highest percentage of cancelled surgeries was 69 of 244 (28.3%) patients scheduled for laparoscopic bilateral tubal ligation.
Sample Characteristics of Gynecologic Surgery Patients
One person from the no cancellation group had missing BMI information.
BMI, body mass index; M, mean; SD, standard deviation.
Table 3 shows the multivariate logistic regression analysis for cancellation. Surgery performed and rescheduled surgery both remained statistically significant by multivariate analysis when comparing “no cancellation” with “yes cancellation.” Surgery performed was associated with lower odds for cancellation (p = 0.002), whereas rescheduled surgery was associated with higher odds for cancellation (p < 0.001). However, surgery type and indication for surgery were no longer significantly associated with cancellation in the multivariate analysis. R square statistics for proportion of variance was very high with five of six measures ranging from 0.89 to a perfect value of 1.00.
Multivariate Logistic Regression Analysis for Cancellation
CI, confidence interval; OR, odds ratio.
In multivariate logistic regression analysis for cancellation that excluded the 244 patients with laparoscopic bilateral tubal ligations scheduled for elective surgery, the same significance pattern occurred as in the whole sample. Surgery performed was associated with lower odds for cancellation (odds ratio [OR] 0.0004, 95% confidence interval [CI] 6.13 × 10−6–0.03, p < 0.001). Rescheduled surgery was associated with higher odds for cancellation (OR 78,547.2, 95% CI 2486.19–2,481,576.00, p < 0.01). Surgery type was not significantly associated with cancellation (OR 0.94, 95% CI 0.01–128.78, p = 0.98).
Cancellation reason (n = 168) is illustrated in Figure 1. Nearly half of those cancelled were attributed to patient reasons and more than one-third for hospital reasons. Also, almost all cancellations occurred one time (n = 161, 95.8%). There were only four people (2.4%) who cancelled two times, one person (0.6%) who cancelled three times, and two people (1.2%) who cancelled four times. For the four patients with malignant diagnoses whose surgeries were cancelled, the reasons for cancellation were patient (n = 1), hospital (n = 2), and unknown (n = 1). These four surgeries were rescheduled and successfully performed.
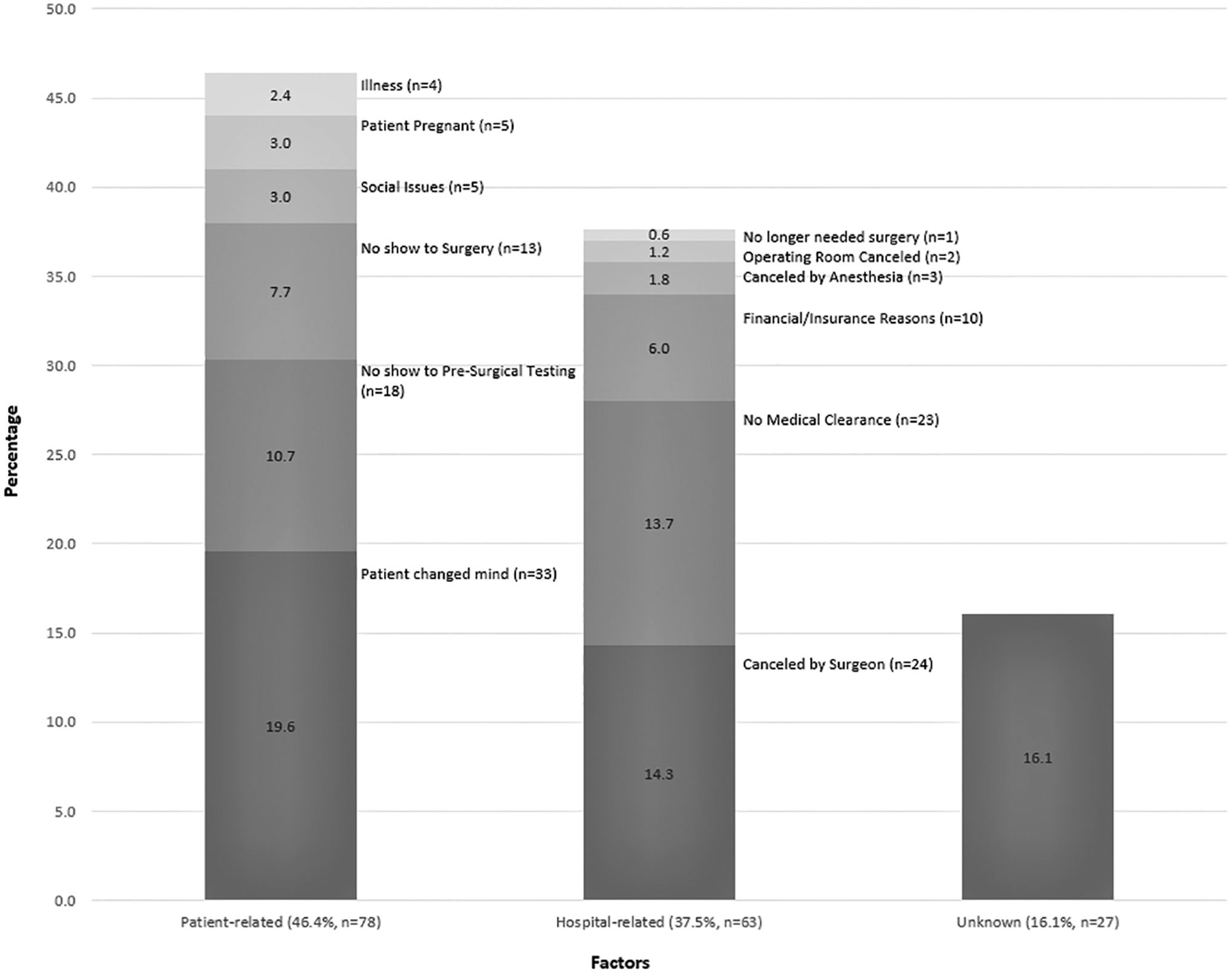
Percentages of reasons for cancellation (N = 168).
Discussion
We found that only surgical-related variables were associated with cancellation. In the multivariate analysis, surgery performed was associated with lower odds for cancellation and surgery rescheduled was associated with higher odds for cancellation. This was expected as all surgeries performed were not cancelled and all rescheduled surgeries had been previously cancelled. In the univariate analysis, there was a greater percentage of those with major surgery in the “no cancellation” group than the “yes cancellation” group. None of the demographics, chronic health conditions, and timeline variables were associated with cancellation. The typical cancellation pattern was to only cancel one time and there were very few repeat cancellations.
We found that surgery rescheduled was associated with higher odds for gynecology surgery cancellation. One study that looked at plastic surgery cancellations found that 66% of patients eventually received their surgery. 14 Our study found that 97% of cancelled surgeries were rescheduled and 88% of the patients who were rescheduled eventually received their surgery. The reasons for rescheduled surgeries are multifactorial. Patients may reschedule surgery to a more convenient time while others may delay surgery or choose to avoid it all together. Also, surgeries may be rescheduled for physician or hospital reasons related to lack of preoperative requirements or availability of requested intraoperative instrumentation or postoperative care. Furthermore, in our study, almost all surgeries were rescheduled and most were successfully completed. We found that surgery performed was associated with lower odds for gynecology surgery cancellation. This is expected since patients who receive their surgery indicate that their surgery was not cancelled.
We found that major surgery cases had statistically significant fewer cancellations than minor surgery cases in the univariate analysis, but this pattern was not retained in the multivariate analysis. Our univariate findings correlate with the urogynecology research reports that found major surgery cases have fewer cancellations than minor surgery cases. 12 However, we observed only 27 cancelled major cases of the 760 cases studied and this small proportion did not retain significance in the multivariate analysis. We suggest that the two predictor variables on multivariate analysis, that is, surgery performed and rescheduled surgery, are critical factors related to surgery cancellation and minimize the significance of additional factors.
We did not find any association of any demographic variables of age, race/ethnicity, BMI, or insurance type with gynecology surgery cancellations. Previous general surgery research reports that age is associated with surgery cancellation,2,6,7 whereas others observe no difference.12,13 Our study did not identify any independent association of age with surgery cancellations. We suggest that gynecology patients requiring elective surgery are generally of reproductive age and healthy. Gynecology patients are more likely to proceed with surgery unless a nonsurgical option for indicated therapy exists.
Previous literature reports that minority groups of Hispanics and blacks are more likely than whites not to attend their outpatient clinic appointments. 8 Cancellation rates for elective surgery observed in our study do not support this finding 12 and are similar among each of the race/ethnicities in our sample. However, nearly three-quarters of patients in our study were Hispanic and our study may not have sufficient statistical power to compare Hispanic patients with the smaller number of white and Asian patients.
The general surgery literature suggests that obese patients may have more surgery cancellations. 9 Our findings for gynecology surgery do not support this pattern. More than half of our study cohort was obese. We speculate that the women who seek surgical intervention for gynecologic indications are more likely to proceed regardless of preoperative counseling about potential morbidity from being obese. This may occur because the recommended gynecology surgery provides definitive treatment of their medical diagnosis and can only be provided by surgical intervention.
Previous research also reports that general surgery cancellations are more common in patients with public health insurance of Medicaid and Medicare than in those with private health insurance. 7 Our findings for gynecology surgery do not support this pattern. However, only 11.2% of our patients had private insurance and another 16.7% had public health insurance. The remaining approximately three-quarters of gynecology patients scheduled for elective surgery in our safety-net hospital setting were self-pay. For such patients at our institution, their surgery costs are highly subsidized by an income-based charity care financial reduction and, therefore, this is of less impact as a reason for cancellation.
We found no association of diabetes and hypertension with gynecology surgery cancellations. Previous research reports that diabetes 6 and hypertension6,11 are each associated with increased general surgery cancellations. Less than 10% of our patients exhibited diabetes and ∼20% reported hypertension. Medical problems that are clinically significant are less common in patients of reproductive age and likely influence surgery cancellation to a lesser degree.
Previous research reports that patients with a malignant preoperative diagnosis had less surgery cancellations than other patients. 13 Our study did not find any statistically significant difference between surgery cancellations for malignancy and benign cases. We suggest that the lack of statistical significance is most likely due to the low percentage of surgeries scheduled for malignancy from both the “yes cancelled” and “no cancelled” groups (4.7%).
We did not find any association of any timeline variable of day of week or season with gynecology surgery cancellations. Previous research reports either a “Monday effect” of increased general surgery cancellations 4 or increased urogynecologic surgery cancellations later in the week. 12 Our study differs from this pattern. We suggest that in our institution, the type of patients scheduled on Monday are likely patients with malignancy or more complicated surgeries and, therefore, these patients are typically more invested in the procedure and less likely to cancel their procedure. Previous research is mixed with the impact of season on general surgery cancellation where some report an association 13 whereas others do not.2,6 Our study is similar to those that report no association. We suggest that the patients in our study are less impacted by season or holiday schedules as they are less likely to have paid employment benefits for such holiday leave and also live in a community that has stable employment without seasonal fluctuations.
We found that there were large percentages of both patient-related and hospital-related cancellations. However, the typical cancellation pattern was to cancel only one time and 97% of cancelled cases were rescheduled and 88% were successfully completed. Our findings are greater than the 66% of patients rescheduled and completed surgeries reported in one study of plastic surgery cancellations. 14 The majority of the patient-related reasons for cancellation in our study were patient changed her mind (19.6%, n = 33) followed by no-show to presurgical testing (10.7%, n = 18). Only 2 of the 33 patients who changed their mind were scheduled for major surgical procedures and 24 of the remaining 31 were initially scheduled for bilateral tubal ligation. We suggest that the majority of cancelled elective surgeries in our study were optional surgical procedures for which viable alternative therapies are readily available. These patients may benefit from additional preoperative counseling before surgery scheduling.
The majority of hospital-related reasons for cancellation in our study included cancelled by an attending 14.3% (n = 24) and no medical clearance 13.7% (n = 23). There are various reasons as to why physicians might cancel scheduled surgeries, including personal illness, family emergency, unexpected delay in surgical start time, unavailability of surgical assistance or requested perioperative care, and discomfort with patient expectations or follow-up care. These decisions are also influenced by scheduling conflicts due to operating room administrative changes. There are several possible reasons for surgical cancellation for lack of medical clearance that include patients may have been unaware of the requirement, patients were unable to obtain clearance, or patients obtained clearance but did not provide the documentation in a timely manner. Written requests and clear instructions for providers as well as patients may significantly reduce this reason for cancellation. Hospital-related reasons for cancellation may be an area more suited to successful intervention than patient-related reasons for cancellation.
This study has some strengths. First, this study includes the ability to identify potential areas of improvement for patient care. For example, although elective surgery was not statistically significantly associated with cancellation, the highest volume of surgical cancellations was tubal ligations, which comprised 244 of 249 elective surgical procedures. Further investigation of this subset of surgical cancellations identified that patients were routinely consented for sterilization during pregnancy and scheduled for surgery immediately postpartum. Most new mothers chose to continue the contraceptive method they chose before hospital discharge after delivery rather than proceed with surgery. To avoid cancellation, our institutional practice changed to scheduled tubal ligation if desired, at the early postpartum visit instead of immediately postpartum. Second, this study illustrates the need for a comprehensive multidisciplinary approach to preoperative care to address patient, hospital, and surgeon-related components of optimal service.
This study has several limitations. First, this study was from a single safety-net community hospital and thus may not generalize to other types of hospitals. Second, although our site is a teaching hospital, gynecologic surgical volume for residency training is supplemented by participation at off-site facilities and these cases were not available for this project. Third, different providers individually documented the reasons for cancellation at their discretion and these were not standardized across disciplines or point of care. Fourth, gynecologic surgery cancellations may be impacted by administrative changes in delivery of care that may alter patient care over a limited time. For example, the availability of operating room time or the availability of surgeons to accommodate the operating room schedule can impact the number of cases that can be scheduled. Future research would be useful to study the role of administrative changes in delivery of care.
In conclusion, we found that rescheduled surgeries were associated with higher odds for gynecology surgery cancellation. Also, we found that the majority of cancellations were patient related. Patient-related reasons include patient changed her mind, pregnancy, social issues, illness, no-show to presurgical testing, and no-show to surgery. We recommend that before surgery scheduling, physicians modify their approach to ensure patients fully comprehend potential alternatives to surgery as well as the importance of patient commitment to undergo optional elective surgery as contrasted with recommended therapeutic surgical intervention. In addition, patients should understand clearly the importance of scheduled surgery and the necessary steps to proceed with surgery such as presurgical testing and medical clearance. Patients should be provided with enough time to obtain medical clearance before the surgery date. A multidisciplinary team that utilizes physicians, nurses, and patient navigators can optimize successful patient education and completion of preoperative testing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this project.