
Abstract
Objective:
The goal of this research was to perform a cost–utility analysis of abdominal hysterectomy (AH), compared with laparoscopic hysterectomy (LH), at the Ramathibodi Hospital, of Mahidol University, in Bangkok, Thailand, from a societal perspective.
Materials and Methods:
A prospective study was conducted from May 2018 to May 2019 with 112 participants (n = 56 for each group), ages 35–50, who underwent AH or LH for benign conditions. Health–utility value was evaluated by the EQ-5D-5L [EuroQual–5 Dimensions–5 Levels] questionnaire upon admission and at 6 weeks and 3 month post the operations. Direct costs, direct nonmedical costs, indirect costs, health-related quality of life (QoL), and incremental cost-effectiveness ratio (ICER) values were compared between AH and LH. A 1-way sensitivity analysis also identified cost variables that affected ICER most.
Results:
Patients who had LH had lower estimated blood losses, shorter hospital stays, and fewer days off after surgery, but had longer operation times, than patients who had AH. There was no significant difference in rates of complications between the 2 groups. The direct medical costs for LH were higher than for AH (median [minimum–maximum], $1836.00 [$1082.80–$3072.70] versus $1151.30 [800.10-2529.50]; p < 0.001), but no significant differences were found for direct nonmedical costs (p = 0.274) and indirect costs (p = 0.729) between AH and LH. The ICER at 6 weeks post operation was $647.1 per 1 additional utility score. The factor that affected ICER most was direct medical costs of LH.
Conclusions:
LH has several clinical advantages over AH for patients with benign gynecologic conditions. However, when comparing LH to AH in Thailand, LH seemed to be less cost-effective relative to LH in Western countries because of the higher direct costs of LH than AH in Thailand. The incremental cost for a better QoL for patients undergoing laparoscopic surgery was $647.10 for 1 extra unit of QoL per day. Direct medical costs of LH was the most-important factor affecting incremental cost.
Introduction
Hysterectomy is the second most-common procedure after cesarean section in obstetrics and gynecology and is the choice of treatment for many conditions, such as uterine fibroids, endometriosis, pelvic organ prolapse, and malignancy. According to the evolution of surgery, the development of various types of hysterectomy emerged from laparotomy, through vaginal hysterectomy, and, eventually, laparoscopic surgery, which has been developed since the 1970s. 1 Previous studies compared the advantages of various hysterectomy methods. In most cases, laparoscopic hysterectomy (LH) induced lower blood losses and less postoperative pain, shorter hospital stays, and days off after surgery, as well as facilitating faster returns to normal activities, but usually required longer operative times. A Cochrane review of surgical approaches to hysterectomy (vaginal, laparoscopic, abdominal [AH], and robotic hysterectomy [RH]) for benign gynecologic diseases published in 2015 showed that vaginal hysterectomy (VH) appeared to be superior to LH and AH because of VH's shorter postoperative recovery. In addition, LH had more advantages than AH when it was not feasible to performVH. 2 Thus, quality of life (QoL) for patients undergoing laparoscopic surgery is assumed to be better than for those who undergo laparotomy.
Data on the cost-effectiveness of types of hysterectomies are controversial. Kaaki et al., in the United States, compared the direct costs of VH, AH, LH, and RH, 3 and Pellegrino et al., in Italy, compared the direct costs of AH, LH and RH. 4 Both studies demonstrated higher direct costs and longer hospital stays with AH than LH. A study from China, by He et al. compared 4895 hysterectomies in multicenters and demonstrated greater cost-effectiveness of LH than AH because of lower estimated blood losses (EBLs) and less postoperative pain. 5 Although many studies favored LH, some previous studies did not show the benefit of LH over AH. Sculpher et al. studied the cost-effectiveness of LH, compared with standard hysterectomy, in 1346 woman who underwent hysterectomy for benign diseases. Quality-adjusted life-years (QALYs), compared between LH and AH groups, were not significantly different (mean QALYs: 0.007; 95% confidence interval [CI]: −0.008 to 0.023), but LH required higher operative costs than AH—that is, about $240.00 per person within 52 weeks of follow-up. 6
Geographic region affects the cost of the hysterectomy procedure. Even in the studies performed in various regions within the United States, the operation costs in the mid-Atlantic region were the highest, compared with the Pacific, South Atlantic, and South Central regions. 7 In Thailand and Southeast Asian countries, there is no published cost analysis of LH, compared to conventional AH. Therefore, this study compared cost–utilities, using an economic evaluation between LH and AH.
Materials and Methods
This prospective study and cost–utility economic evaluation was conducted at Ramathibodi Hospital (of Mahidol University, in Bangkok, Thailand), a tertiary medical school with resident and fellow training. There were 2894 AHs and 3646 LHs within 10 years (2008–2019) in this hospital. The study was approved by the Ethical Clearance Committee on Human Rights Related to Researches Involving Human Subjects, of the university's faculty of medicine.
The inclusion criteria were women, ages 35–50, with benign conditions who were underwent either AH or LH from May 2018 to May 2019. Subjects were excluded if concomitant operations other than salpingo-oophorectomy were performed or if the subjects had endometriotic cysts. The other exclusion criteria were patients who were diagnosed with cancer and were not able to follow-up by telephone at 6 weeks and 3 months post the operations.
The included patients were allocated to either the AH or LH by the individual surgeons and based on the patient's health care coverage and financial viability. The Social Security System (SSS), the Civil Servants System (CSS), and the National Health Security Program (NHSP) are the 3 public-health coverage schemes in Thailand. Private health care insurance is purchased by some people for extra coverage. AH costs are covered fully by the SSS, CSS, and NHSP, but LH costs are only partially covered by the by CSS and are not covered at all by the SSS and NHSP. Private health insurance providers cover both AH and LH. Moreover, some patients pay for the surgical expenditure by themselves.
The current authors performed total hysterectomies for all women who underwent AH or LH. There were 6 staffs in the study, and all of them performed both procedures. Each surgeon performed ∼70 AHs and 60 LHs within 1 year and had more than 10 years of experience in both types of surgery.
Primary outcomes were direct costs, health-related QoL, and incremental cost-effectiveness ratio (ICER). This cost–utility study was involved analysis from a societal perspective. Health–utility value was measured by QoL. The sample size was calculated by a 2-independent means of 2–normally distribution formula from a pilot study considering a data loss of 10%, an α of 0.05, and a power of 80% (β = 0.8). The sample size was 56 participants for each group.
After enrollment, informed consent was obtained from each patient. During admission, participants were interviewed for demographic data and completed, in the Thai language, the EuroQual–5 Dimensions–5 Levels (EQ-5D-5L) questionnaire for QoL. 8 Use of this EQ-5D-5L questionnaire was allowed for the present study by the EuroQual group. At 6 weeks and 3 months' postoperation, participants were interviewed by telephone to collect data regarding expenses and QoL. The answers describing the health state in the 5 dimensions of the EQ-5D-5L questionnaire were converted into utility scores by taking the utility score of 1 (complete health) and subtracting the coefficients of the 5 dimensions. The coefficients represent the utility lost from being in a state of incomplete health. The utility score was developed by the Health Intervention and Technology Assessment Program under the Ministry of Public Health of Thailand and Mahidol University. 8
Direct medical costs referred to operative services, operative instruments, inpatient days, medical imaging, and laboratory services. These costs also included possible readmissions and reoperations. Costs of hospital stays included staff costs, medicine costs, and costs of basic utilities. Surgical costs were considered to be staff costs, anesthetic costs, equipment costs, and costs of basic utilities during the operations. No standard fix rate for surgical costs was provided. Direct nonmedical costs included costs for accommodations, transportation, food, caregiver pay, etc. Indirect costs included costs of lost work days for both patients and their caregivers.
Statistical analysis
The demographic data were presented as either mean + standard deviation or median (minimum–maximum) for parametric or nonparametric continuous data, respectively, and percentage for discrete data. Student's t- and χ 2 tests were applied for normally distributed continuous and discrete data, respectively. A Mann–Whitney-U test was used to analyze nonnormally distributed continuous data. p-Values <0.05 were considered to be statistically significant. Data were analyzed using SPSS, version 18.0. ICER was evaluated to define the relationship between costs and utility-scores for each method and calculated with the following formula:

where ΣCost is a summation of direct medical, direct nonmedical, and indirect costs. A 1-way sensitivity analysis with a Tornado diagram was performed to define the influential factors for the ICER. All costs were adjusted for inflation rate and represented as 2019 values based on the time of the study and were presented in US dollars (∼ $1 USD = 30 Thai Bahts; THBs).
Results
A total of 112 participants, 56 for each group, were enrolled in this study. Baseline characteristic data are reported in Table 1. There were no significant differences in age, parity, underlying medical conditions, previous abdominal surgeries, and principal diagnoses. However, participants in the LH group had higher incomes, and a greater number of participants in the LH group paid for their medical costs by themselves or through private health insurance than the AH group. The LH group also had smaller estimated uterus sizes but higher body mass indices (BMIs) than the AH group. While the operation times in the AH group were shorter than in the LH group, the AH group had more EBLs than the LH group. Participants in the AH group stayed in the hospital and took more postoperative days off than the LH group (Table 2). The number of intra- and postoperative complications was not significantly different between the 2 groups, as shown in Table 3. However, there were 2 conversions of LH procedures to AH procedures due to these patients' severe pelvic adhesions.
Participants' Baseline Characteristics
Data presented as mean ± standard deviation.
Data presented as number (percentage).
Data presented as median (minimum–maximum).
AH, abdominal hysterectomy; LH, laparoscopic hysterectomy; yrs, years; BMI, body mass index.
Intra- and Postoperative Data
Data presented as mean ± standard deviation.
Data presented as median (minimum–maximum).
AH, abdominal hysterectomy; LH, laparoscopic hysterectomy; min, minutes; EBL, estimated blood loss; d, days.
Surgical Complications
AH, abdominal hysterectomy; LH, laparoscopic hysterectomy; TAH, total abdominal hysterectomy.
Outcomes of the cost- and utility-scores are shown in Tables 4 and 5. The LH group had significantly higher direct medical costs and surgical costs, compared to the AH group but no difference in costs of hospital stays or direct nonmedical and indirect costs. In addition, there was no significant difference between the utility scores of the AH and LH groups, as shown in Table 5. All patients provided data about their QoL.
Direct and Indirect Costs of AH and LH
AH, abdominal hysterectomy; LH, laparoscopic hysterectomy.
Utility Scores Calculated from the EQ-5D-5L Between AH and LH
EQ-5D-5L, EuroQual–5 Dimensions–5 Levels questionnaire for quality of life (used with permission by the EuroQual group); AH, abdominal hysterectomy; LH, laparoscopic hysterectomy; SD, standard deviation.
For the cost–utility analysis, the utility scores and ICER were calculated. Although there was no significant difference between the utility scores of both groups, participants in the LH group had higher utility scores, compared to the scores in the AH group at 6 weeks post the operations. The ICER for a unit of utility score gained per day, generated at 6 weeks for LH was $647.10. The 1-way sensitivity analysis was calculated and produced a Tornado diagram (Fig. 1). The direct medical costs of LH was the most-influential parameter for the discount rates for cost and outcome.
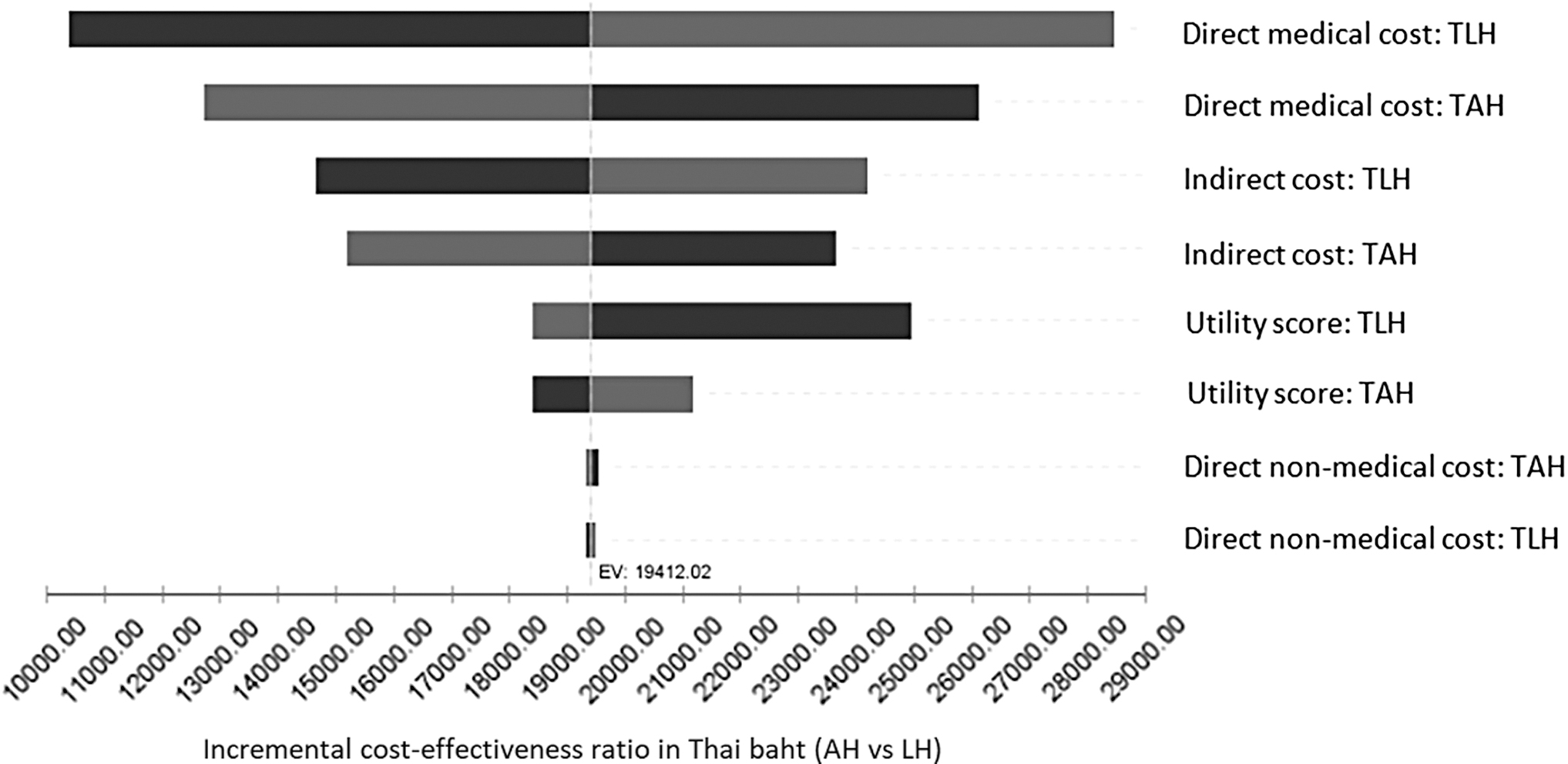
Sensitivity analysis shown by Tornado diagram. Variables tested in a 1-way sensitivity analysis are shown on the y-axis, while the dotted line on the x-axis represents the base-case value in terms of incremental cost-effectiveness ratio (ICER) in Thai Bahts (currency of Thailand). TLH, total laparoscopic hysterectomy; TAH, total abdominal hysterectomy.
Discussion
This study demonstrated that, in a university tertiary hospital in Thailand, the direct costs for LH were higher than for AH, but LH provided many other advantages over AH, such as lower blood loss, shorter operative times, reduced hospital stays, and fewer days off after surgery. The cost of surgery contributed most to the direct costs of AH and LH. There were no significant differences in indirect costs between AH and LH. The utility scores according to the EQ-5D-5L questionnaire for QoL were not significantly different between AH and LH within 3 months of the operations. The incremental cost for gaining 1 unit of utility score for the LH group, compared to the AH group, was $647.10 (∼ 19,412.02 THB). The direct medical costs of LH was the most-influential factor for the ICER.
LH reduces invasiveness of conventional abdominal surgery and has many advantages over AH. The current study's results were in line with the outcomes from the Cochrane study and other previous studies (lower blood loss, shorter hospital stay, fewer days off after surgery2–5,9,10); however, the present study showed no significant difference between the complication rates of the 2 study groups, which were different from those in another study. 10 This could be explained by the difference in experience between the staff at this Thailand hospital, who had usually performed laparoscopic surgery for more than 10 years, and the staff used in that other study. However, the lower BMIs and uterine weights in the LH group could be significant biases for selecting the types of surgery in the current study.
A diversity of direct medical costs was found among several countries. The current study's results were comparable to a systematic review of studies performed in many countries. 11 This review showed that total medical costs for hysterectomy in Western countries, including Canada, the United States, Italy, and Australia4,9,12,13 were far higher than in Asian countries, including China, Taiwan, and Korea as well as the current study in Thailand.14–17 Direct medical costs were influenced by method of hysterectomy, length of stay, and operative time. 13
Apparently, LH, compared to AH in Thailand and Asian countries are less cost-effective relative to those in Western countries. The direct medical costs of AH were higher than those of LH in Canada, the United States, Italy, and Australia, in contrast to the direct medical costs of AH in Thailand and China, which were lower than those of LH.3,6,9,14 While the costs of operative service are an important component of the direct costs in Thailand, costs of hospital stay contribute largely to the direct costs in Western countries. In addition, the indirect costs in the current study were not significantly different between LH and AH; therefore, the results showed that there were no societal benefits of LH over AH. This result contrasted with other studies,10,18–24 which was probably because of the lower labor cost of caregivers, compared to such costs in Western countries.
Costs of hospital stays (per day) contribute most to the direct medical cost difference between AH and LH in Western and Asian countries. These costs were several-folds higher in Western countries than in Thailand and Asian countries, although the length of stays were much longer for Thai and Chinese patients. 14 Data from previous studies showed that the length of hospital stays for AH were longer than for LH (AH versus LH, 4–5 versus 2 days in Western countries9,10 and 5 days versus 4 days in the present study); therefore, length of stays contributed to the higher direct costs for AH than LH in Western countries. It is a common practice in Thailand for a patient undergoing LH to stay in the hospital for 3–4 days because Thai women are very concerned and anxious about the surgery and its potential complications. Moreover, the cost of a hospital stay in Thailand is not expensive.
Data from the current study demonstrated that the incremental cost for achieving an additional QoL unit per day within 3 months after operations in the LH group, compared to the AH group, was $647.10 (∼ 19,412.02 THB). The direct medical cost of LH was the most-affected factor in the current study's ICER according to the sensitivity analysis. Therefore, a decrease in this cost might improve QoL because it would enable offering LH to patients.
Thai people are generally covered by both the public and private sectors, depending on each patient's workplace and the coverage's affordability. The 3 public health coverage schemes, as noted previously, are the SSS, the CSS, and the NHSP. The SSS provides social welfare for private employees. The CSS supports health care services for civil servants and their families. The NHSP, a tax-financed scheme, provides free health care and covers people who are without health protection by the first 2 schemes. Some people may also purchase extra private health care insurance. AH was fully integrated into the SSS, CSS, and NHSP coverage, but the cost of LH was only partially covered by the CSS and was not covered by SSS and NHSP. Private health insurance providers covered both types of hysterectomy. Therefore, patients who underwent LH were generally more affluent than other patients.
However, the direct medical costs of hysterectomy in Thailand were modest, compared with patients' incomes, which was reflected by the high affordability of health care costs for the operation that were paid by patients, themselves. The rates of self-payment for LH and AH were 23% and 17%, respectively. Therefore, to increase health care coverage for LH, it is necessary to lower the direct costs of LH.
Many published strategies have sought to reduce the overall direct costs of hysterectomy, for example, regarding the cost of the instruments and performing outpatient visits instead of performing conventional hysterectomies. Croft et al. showed that educating physicians about the cost of the instruments, which represents a large part of the total medical costs, could reduce the medical costs of LH. 25 Using reusable equipment instead of expensive disposable equipment and reducing the length of hospital stays could also reduce the direct medical costs of LH. Performing outpatient hysterectomies could be an another option for reducing medical care costs according to a study in the United States that showed the lower cost of outpatient LH compared with conventional-admission LH was ∼ $2,000. 9
This study was one of the first to examine cost–utility of hysterectomy in Thailand, an upper middle-income country, according to a classification by the Organization for Economic Co-Operation and Development (OECD). The results of this study could help inform patients who undergo hysterectomy and might be helpful for improving policy regarding hysterectomy method choices.
There were several limitations in the present study. First, the follow-up duration was limited to 3 months, and, consequently, utility was taken as the effect measure instead of QALY. Second, the telephone interviews could have been subject to recall bias. Third, without randomization, there might have been a tendency for selection bias. Finally, the data were collected from a tertiary-facility hospital and might not be generalizable to other secondary-facility hospitals in Thailand.
Conclusions
LH was shown to have lower EBL, reduced hospital stay, and fewer days off after surgery, compared to AH. In Thailand, LH seems to be less cost-effective relative to Western countries because of the higher direct costs of LH and because there is no difference in the indirect costs between LH and AH. Participants in the LH group had better QoL evaluation results but required $647.1 to gain 1 additional unit of QoL per day at 6 weeks post the operations. The direct medical costs of LH was the most important factor for the incremental costs.
Footnotes
Acknowledgment
The authors would like to thank the Department of Obstetrics and Gynecology, Faculty of Medicine, Ramathibodi Hospital, Mahidol University.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this article.