
Abstract
Objective:
There are limited studies on laparoscopy for benign hysterectomy in low- and middle-income countries. This article describes national trends in modes of hysterectomy in Brazil and compares outcomes by regions and health sectors.
Materials and Methods:
This was a cross sectional retrospective analysis of benign hysterectomies from open-access national databases (public sector: 2008–2017; private sector: 2016) in Brazil. Variables examined included the modes (vaginal, abdominal, and laparoscopic) of hysterectomies, geographic regions, mortality rates, and lengths of stay (LOS).
Results:
Benign hysterectomies decreased by 19.2% over 10 years. The proportion of abdominal surgeries increased from 85% to 88%. Despite an increase in laparoscopic surgeries (0.2–0.9%), minimally invasive surgery (vaginal and laparoscopic) decreased (14.7%–12.6%), largely driven by a drop in vaginal cases (14.5%–11.7%). More laparoscopic hysterectomies were performed in the private sector compared to the public sector (11% versus 1%; p < 0.001). There were significant geographic disparities, with 17% of hysterectomies in the private sector performed laparoscopically in the south compared to 9% in the northeast (p < 0.001).
Conclusions:
Trends in modes of hysterectomies have changed. There are regional inequities, with wealthier regions accessing more laparoscopic surgery. Understanding the trends and factors affecting access to laparoscopy is essential for ensuring equitable access to high-quality gynecologic care. (J GYNECOL SURG 37:337)
Background
Hysterectomy is the most frequently performed non-obstetric surgical procedure in women, with up to 35% of women in high-income countries (HICs) undergoing this procedure by ages 55–60.1–3 In many HICs, there has been a shift from abdominal hysterectomy to minimally invasive approaches to hysterectomy, including those that use vaginal, laparoscopic, and robotic techniques.2,4 Compared to abdominal hysterectomy, vaginal and laparoscopic approaches have been shown to induce faster returns to daily activities, shorter hospital stays, fewer infections, lower intraoperative blood losses, and lower costs 1 . As such, these minimally invasive surgical approaches are recommended as the preferred approach by professional organisations.5,6
There is much less evidence available on the frequency of hysterectomy in low- and middle-income countries (LMIC), and even more scarce data on the use of laparoscopy or other minimally invasive surgeries in these contexts. Expansion of laparoscopy in LMICs could play a critical role in ensuring that patients have access to high-quality surgical care. The proven benefits of shorter hospitalization, decreased recovery time, and faster return to normal activities could make a critical difference in settings where resources are limited and where long postoperative recovery can result in impoverishment.1,7
Brazil is an upper–middle-income country with a single-payer, single-provider, free-at-the-point-of-care, universal health care system. However, inequities in access to surgical care exist among regions, 8 and little is known about hysterectomy and laparoscopy use in this country. The overall purpose of this article is to describe the national trends in modes of benign hysterectomies performed in Brazil.
Materials and Methods
Data sources
This was a cross-sectional retrospective analysis of hysterectomies performed for benign indications in Brazil over a 10-year period ending in 2017 (the most-recent year with a complete data set available) and registered in national databases. A 10-year-period prior to 2017 was thought sufficient to assess changing trends of modes of hysterectomy. Data were obtained from two publicly available online data platforms containing data on hospital admissions and linked to the Brazilian Ministry of Health. DATASUS contains data from the Sistema Único de Saúde (SUS), and has been collecting aggregate data on hospital admissions financed by SUS for almost three decades. 9 Data were also retrieved from a private health plan, the Agencia Nacional de Saude Suplementar (ANS), which collects data on patient admissions paid for by a private health plan, which supplements the health care coverage of approximately one-quarter of Brazilians. 10 ANS data are newer and, at the at the time of this study, contained complete data for 2016 only. Both DATASUS and ANS collect data on procedure codes and International Classification of Diseases diagnosis codes tied to admissions; however, individual patient-level data, such as demographic and medical comorbidity were not available. There was no overlap in procedures captured by these two databases.
Inclusion and exclusion criteria
To enable a trend analysis, all hysterectomies were included for benign indications performed in Brazil in the 10 years prior to the most recently available data at the time of the study (i.e., 2008–2017). All of the benign hysterectomies performed in 2016 by the private system (ANS) were also included. All cases performed for malignant indications were excluded. For both public and private databases, this corresponded to codes for “oncology” and “radical hysterectomies.” Procedures coded as “hysterectomies with salpingectomy and/or oophorectomy” were excluded from analysis as the mode of hysterectomy was not specified within the databases for these cases. Robotic-assisted hysterectomies were also excluded, as these are not routinely performed in the public sector and the few performed in the private sector, are not covered by insurance companies and therefore are not reported in the databases. Although database coverage is limited to inpatient admissions, hysterectomies are not routinely performed in ambulatory settings in Brazil, and a search of national databases on ambulatory surgical procedures yielded no records for hysterectomies.
Variables
To assess trends over time and to provide sufficient data to calculate perioperative mortality rate (POMR), data were extracted on total volume of hysterectomies, modes of hysterectomies, and mortality from the public database from 2008 to 2017. Data on length of stay (LOS) for 2017 were also extracted from the public database. To enable a public–private comparison data on volume, mode, and region were extracted for 2016 from both public and private databases. From the private sector, ANS database data were extracted from January to December 2016, the most-recent and complete dataset available for that database.
In the public database, modes of hysterectomy were coded as vaginal hysterectomy, laparoscopic hysterectomy, total hysterectomy, and subtotal hysterectomy. The latter two refer to abdominal hysterectomy and were combined in one category. In the private database, modes of hysterectomy were coded as subtotal laparoscopic and total laparoscopic, which were grouped as laparoscopic procedures. Other procedure codes included subtotal hysterectomy and total hysterectomy, including all abdominal and vaginal hysterectomies, without further disaggregation. For the public data, a category of minimally invasive surgery was defined by combining laparoscopic and vaginal hysterectomies.
Similar categorization was not feasible in the private sector given the lack of disaggregation of abdominal and vaginal cases; therefore, data were analyzed as laparoscopic versus open, with the latter including both abdominal and vaginal approaches. POMR was defined as the rate of in-hospital deaths during the same admissions in which the surgical procedures were performed. Given that mortality is a rare outcome of benign hysterectomy, data on in-hospital mortality was restricted to the public database only, to allow aggregation from January 2008 to December 2017. LOS was defined as the number of in-hospital days. Region of location included one of the five geographic regions in Brazil: North; Northeast; Central–West; Southeast; and South. The North and Northeast regions are the most rural and poor areas of the country, while the South and Southeast are the most urban and wealthiest regions. 11 These data were extracted for 2017, the most recent and complete dataset of the public sector.
Statistical analysis
For the public data set from 2008 to 2017, the total number of benign hysterectomies and percentages by mode of hysterectomy were calculated. A generalized linear model was used in a regression analysis, with the Wald test used to assess the trend in total number of hysterectomies over time. the Cochran–Mantel–Haenszel χ 2 test was used for trend to assess changes in the trend of modes of hysterectomies over time.
Total surgical volume was defined as the number of benign hysterectomies per 100,000 women ages 25 or older performed in the public sector and private sector, and calculated nationally as well as for each region. Laparoscopic volume was defined as the number of benign laparoscopic hysterectomies per 100,000 women ages 25 or older performed in the public sector and private sector, and calculated nationally as well as for each region. Population data on women above age 25 were obtained from the 2015 census. 12
Mortality and LOS were compared by mode of hysterectomy. Mode of hysterectomy and surgical volume were compared by region and sector (public versus private). Comparisons between mortality rates and mode, and mode by regions and sectors, were done using the χ 2 test and Fisher's exact test. Continuous data on LOS were presented as mean and standard deviation based on aggregated data extraction, and analysis of variance (ANOVA) was used to perform comparisons by types of approaches. A 2-tailed α of p < 0.05 was used to determine statistical significance. It was determined posthoc, that the sample size of hysterectomies between 2008 and 2017 would provide an 80% statistical power to detect a 1% change in surgical approaches over time and among the regions using the χ 2 exact test and assuming a 2-sided α level of 0.05. Power and sample size calculations were performed using nQuery Advisor, version 8.0 (Statistical Solutions Ltd., Cork, Ireland). All statistical analyses were performed using Stata, version 15.0 (StataCorp, College Station, TX).
Ethics
No ethical institutional review board approval was required, as both databases (DataSUS and ANS tabnet) are publicly available, open access, and contain only de-identified aggregated data. No written consent was required from patients as the data is de-identified, public, and aggregated.
Results
A total of 1,013,889 benign hysterectomies were performed in the public sector between 2008 and 2017. After excluding radical hysterectomies (n = 7563) and hysterectomies for which the mode could not be determined (n = 273,621), the final sample of hysterectomies for trend and mortality analysis in the public sector was 740,268 (Fig. 1: top panel). In 2017, there were 64,2175 hysterectomies available for LOS and regional analysis. (Fig. 1: top panel). In 2016, there were 65,563 hysterectomies in the public sector and 26,354 in the private sector available to determine surgical volume, regional analysis, and public–private sector comparisons. (Fig. 1: bottom panel).

Top panel: Final sample size after exclusion criteria were applied to hysterectomies performed in the public sector in the decade between 2008 and 2017 and for 2017 alone. Bottom panel: Final sample size after exclusion criteria were applied to hysterectomies performed in the public sector and private sector in 2016. This sample was used to analyze surgical volume, conduct a regional analysis, and make public sector versus private sector comparisons for 2016.
Trend of modes of hysterectomies over time
The total number of included hysterectomies performed for benign indications in the Brazilian public sector varied from 79,641 hysterectomies in 2008 to 64,275 in 2017, representing a 19.2% decrease over the 10-year period. The proportion of abdominal hysterectomies increased from 85% to 88% from 2008 to 2017 (p < 0.001; Fig. 2). Laparoscopic hysterectomies also increased from 0.2% to 0.9% (p < 0.001), while vaginal hysterectomies decreased from 14.5% to 11.7% in the 10-year period. Driven by the drop in vaginal cases, overall minimally invasive surgery (vaginal and laparoscopic) decreased significantly from 14.7% in 2008 to 12.6% in 2017 (p < 0.01).
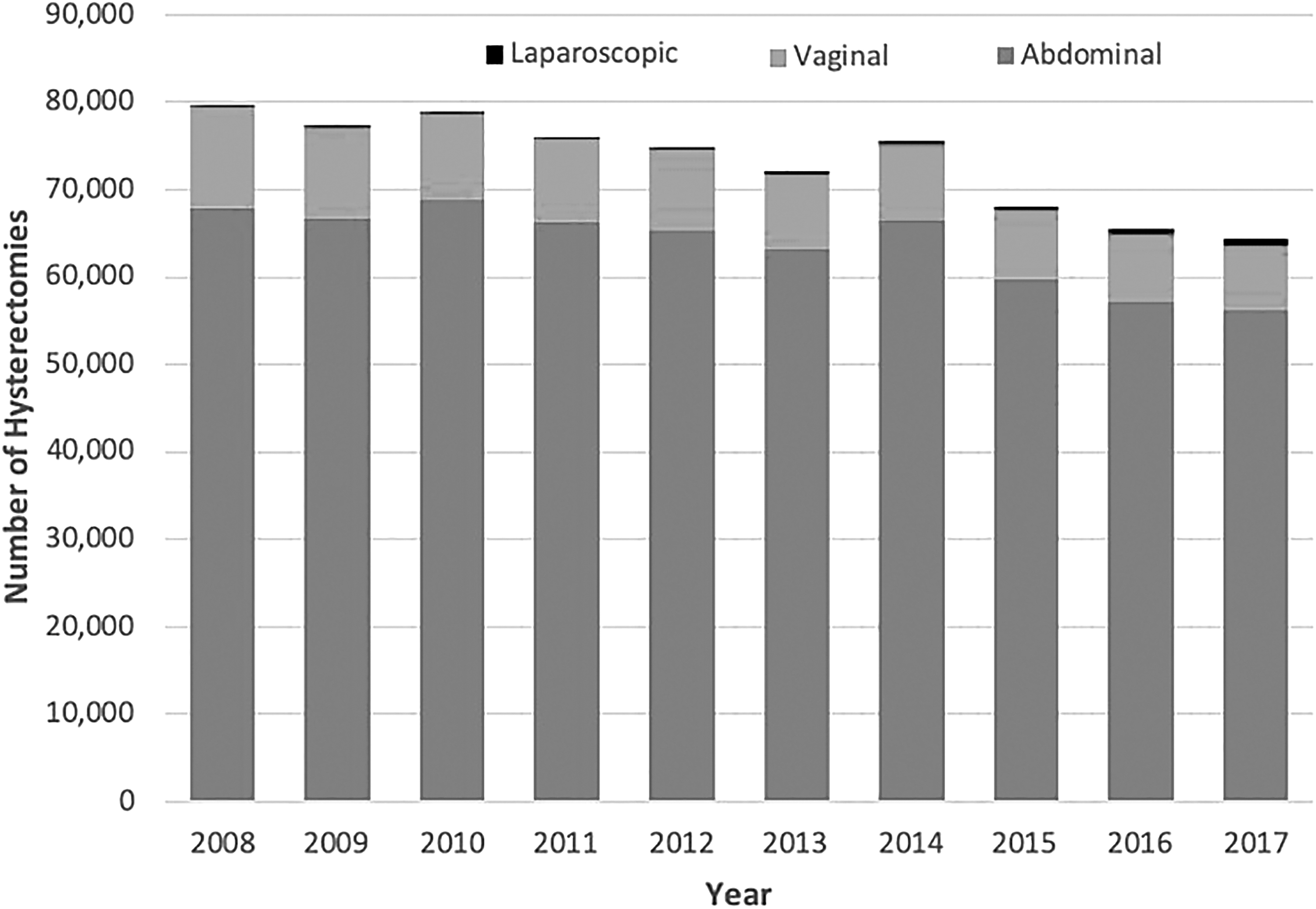
National trends in hysterectomy mode in the public sector in Brazil over the last 10 years.
Mortality
From 2008 to 2017, there were 721 deaths among 714,668 women undergoing benign hysterectomy in the public sector, giving an overall POMR for benign hysterectomies of 0.1%. Overall, the mortality rates for abdominal, vaginal, and laparoscopic hysterectomies were 0.11%, 0.05%, and 0.03%, respectively. Minimally invasive surgical (laparoscopic and vaginal) hysterectomies was significantly lower, compared to abdominal hysterectomies nationally (0.05% versus 0.11%; p < 0.001). There was a significant difference in mortality rates between minimally invasive surgical (laparoscopic and vaginal) and abdominal hysterectomies. See Table 1.
Incidence of Mortality per 1000 Procedures for Minimally Invasive Surgical (Laparoscopic and Vaginal) Versus Abdominal Hysterectomies Stratified by Region in the Public Health Sector Between 2008 and 2017
Indicates statistically significant results (p < 0.05).
MIS, minimally invasive surgical.
LOS (public sector)
In the public sector in 2017, the mean LOS in-hospital was significantly different according to the mode of surgery (p < 0.001). LOS was shortest for patients undergoing laparoscopic surgery (2.46 days; 95% confidence interval [CI]: 2.4–2.6), followed by vaginal hysterectomy (2.57 days; 95% CI: 2.4–2.8), and was longest for abdominal surgery (2.65 days, 95% CI: 2.5–2.8).
Modes of hysterectomies by geographic regions
To estimate current regional variations in modes of hysterectomy, data from the most recent year, 2017, in the public sector were analyzed. There were significant regional variations in access to laparoscopic surgery, with the South and Southeast regions performing a larger percentage of laparoscopic and vaginal hysterectomies, compared to the North, Northeast and Central–West regions (Table 2).
Modes of Benign Hysterectomies by Region in the Public Health Sector in Brazil in 2017
Values are n (%). p-Values are calculated using the χ 2 test. p-Values compare the distribution of procedures across all regions.
Private sector and public health sector comparison
Overall, the public sector accounted for the majority (77.7%), of the 91,917 included hysterectomies performed in 2016. This distribution between private and public sectors varied significantly by region (p < 0.002). The private health system performed the majority of hysterectomies in the Southeast region (58%) but a minority (3%) in the North region.
Overall, the private sector had a significantly higher proportion of laparoscopic hysterectomies (13%), compared to the laparoscopic proportion in the public sector (0.6%). This remained true in all geographic regions with the largest difference being in the South, where 17% of all hysterectomies in the private sector are performed laparoscopically, compared with to only 0.21% of hysterectomies in the public sector (Table 3).
Proportion of Hysterectomies Performed Laparoscopically by Region in the Private Sector and Public Sector in 2016.
Values are n (column %).
% in the sector.
All p-values <0.001; p-values are calculated using the χ 2 test.
Surgical volume by geographic region in public sector and private sector
To estimate surgical volume, private and public data for 2016—the most current dataset available for both sectors—were combined. Nationally, there were an estimated 212 benign hysterectomies per 100,000 women (95% CI: 210–212 per 100,000). This varied regionally, from 168/100,000 (95% CI: 164–172 per 100,000) procedures in the North region to 272/100,000 (95% CI: 270–275 per 100,000) procedures in the Northeast region. Nationally, laparoscopic surgical volume was 11/100,000 (95% CI:10.6–11.1 per 100,000), varying from 4/100,000 (95% CI: 3.7–4.8 per 100,000) laparoscopic hysterectomies in the North region to 16/100,000 minimally invasive surgery (95% CI: 14.9–16.4 per 100,000) procedures in the South region. (Fig. 3)

Discussion
Principal findings
This study examined trends in hysterectomies by mode over time in Brazil and was one of few studies examining trends in gynecologic surgery in LMICs. Fewer hysterectomies were performed over time, and a decreasing proportion of these hysterectomies were performed by minimally invasive surgery (vaginal and laparoscopic), driven by a decrease in vaginal hysterectomies. The private sector performed a significantly higher proportion of laparoscopic hysterectomies, compared to the public sector. There were also significant regional differences in rates, modes of hysterectomies, and POMR.
Results in the context of the literature
The decrease in hysterectomies in Brazil is consistent with global trends, and likely stems from an increase in pharmacologic, hysteroscopic, and radiologic treatments for benign gynecologic disease. 3 The Brazilian reported population-based hysterectomy rate is likely an underestimate, given the exclusion of hysterectomies not coded for mode. Reported population-based hysterectomy rates range from 175/100,000 women in Denmark 13 to 540/100,000 in Australia 2 ; thus, even with higher numbers, the finding for Brazil likely falls in the range reported by other HICs. 3
Minimally invasive surgery (vaginal and laparoscopic) in Brazil is currently largely driven by vaginal hysterectomy unlike in HICs, where increasing rates of minimally invasive surgeries are largely driven by increases in laparoscopic surgeries.4,5,14 However, vaginal surgery is declining, which is similar to global trends and accounts for the overall decrease in minimally invasive surgeries that were found. There are likely to be differences in the drivers of trends in HICs and LMICs, which are not yet understood. In Brazil, for example, a high national cesarean section rate of 55%, might influence mode of hysterectomy due to the high prevalence of prior surgeries. 15
There were regional disparities in benign hysterectomy volumes and minimally invasive surgery use, as well as differences in proportions of laparoscopic surgeries in the private sector and public sector. These disparities mirror those seen in the United States in mode of hysterectomy by race, ethnicity, and insurance status, 16 and likely reflect systemwide inequities in access to surgery, as well as disparities in education and training. 17
In Brazil, higher POMR was noted in the south and Southeast regions despite better access to healthcare in these areas. This finding was consistent with POMR trends reported for other surgical procedures. 8 Further research is needed to understand if these are real disparities due to differences in underlying disease burdens, patients' demographics, access to and quality of care, or limitations of data quality.8,18
Clinical, research and policy implications
Given the disparities we found in access to minimally invasive surgery by region and sector, policies targeting scale up of laparoscopy in Brazil must consider how to do so equitably. Brazil has seen a doubling of laparoscopic cholecystectomies in the public sector, indicating that a scale-up of minimally invasive surgery is feasible even in the public sector. 19 However, inequities in laparoscopic training might be amplified due to challenges in obtaining equipment, costs, and steep learning curves, particularly in rural areas with limited support.20,21 Approaches to equitable national scale-up in LMICs have been described through coordination of multiple stakeholders and should be considered in Brazil.22,23
Although differences in LOS were statistically significant, differences by approach were <0.5 days, therefore, are likely of limited clinical significance. However, the LOS for laparoscopic and vaginal hysterectomies (∼ 2.5 days) was higher than those reported in other studies, in which LOS are on average <1 day for vaginal hysterectomies and <2 days for laparoscopic hysterectomies.4,24 This indicates there are further efficiency gains to be derived from minimally invasive surgery in Brazil. Current LOS might stem from longstanding systems of postoperative monitoring and uncertainty around the ease of return if complications arise. Quality-improvement programs directed at creating clinical pathways to enhance recovery after surgery and minimize inpatient stays while maximizing safety could reduce LOS, costs and burdens for patients. Efficiency savings in the public sector are particularly important, given the austerity measures currently in effect in Brazil. 25
Further research is needed to understand barriers to scale-up of laparoscopy in Brazil, and, importantly, to understand what might facilitate the retention of vaginal surgery. Research with individual-level data is also needed, as this would allow for risk-adjustment and a deeper understanding of trends. This, along with measurement of other major complications, could also provide insight on the quality of gynecologic surgical care. 26 Administrative databases in Brazil have been used extensively for epidemiologic and public health studies due to their comprehensive longitudinal data sets and coverage of a large and diverse population. Working with clinicians to make minor modifications in the way the data are collected and reported could enhance their utility significantly for epidemiologic and clinical research.
Strengths and limitations
The databases accessed provide comprehensive, large-sample, national surgical data, which are scarce in LMICs. DATASUS has been used extensively for public health studies, but, being an administrative database, it has some limitations. 18 First, there might be variations in reporting by regions, which could account for some differences seen in mode, rates, and POMR. Second, a lack of unified coding between the public and private sectors limited the comparisons between sectors.
Finally, due to a lack of specific coding in minimally invasive surgery (vaginal and laparoscopy) for all procedures, it was not possible to include hysterectomies with salpingo-oophorectomies. Compared with a vaginal approach, salpingo-oophorectomy has been described to occur 8 times more often with laparoscopic hysterectomies and 12 times more often with abdominal hysterectomies. 27 Thus, the current study's results likely underrepresented abdominal and laparoscopic surgeries and overrepresented vaginal hysterectomies. Given that this coding was uniform across regions and sectors, this study provides a useful initial national assessment as well as a useful analysis of the variations among the regions. Finally, as the private database was relatively new, and data were only available for 2016, a trend assessment for change in approach to hysterectomies was not possible in the private sector. Given the finding that the private sector performs significantly more laparoscopic procedures than the private sector does, this could mean that, at the national level, our findings underestimated growth in this procedure. These data, however, offer an understanding of trends in the public sector, where most of the Brazilian population seeks care. 28
Conclusions
The uptake of laparoscopy in Brazil has been slow in the last decade. There are regional disparities in patients who can access minimally invasive surgery (laparoscopy and vaginal), driven by differences in public sector versus private sector rates. Understanding the trends and factors affecting access to minimally invasive surgery is a first step for surgeons and policymakers to advocate and plan for enhanced training and provision of minimally invasive surgery to ensure equitable access to high-quality gynecologic care.
Footnotes
Author Disclosure Statement
Dr. Abrao reports non-financial support from Bayer, Chugai Pharmaceuticals, Myovant and AbbVie as well as personal fees from Johnson & Johnson, However, none of these are related to the work presented in this publication. All other authors report no conflict of interest or financial disclosure.
Funding Information
Drs. Roa, Ramos, and Citron received support from the Ronda Stryker and William Johnston Global Surgery Fellowship Fund. AA. Boatin is supported by the career development awards from the Eunice Kennedy–Shriver National Institute of Child Health and Human Development (K23 HD097300-01) and the Massachusetts General Hospital Executive Committee on Research through the Center for Diversity and Inclusion.