
Abstract
Background:
Growing teratoma syndrome (GTS) is a rare condition found in patients with nonseminomatous germ-cell tumors who have enlarging masses. This can be in the context of normalized serum markers and occur during or post appropriate systemic chemotherapy. The presence of a mature teratoma and the absence of malignant germ cells on a histopathology report confirms the diagnosis of GTS.
Case:
A 25-year-old female was diagnosed with growing teratoma syndrome at The Gujarat Cancer Research & Institute (GCRI), in Ahmedabad, India. The patient was operated on for an immature teratoma and received adjuvant chemotherapy elsewhere. She was evaluated and diagnosed with GTS at the GCRI and underwent cytoreductive surgery in 2 sessions to remove the now-mature teratoma..
Results:
She is currently disease-free and on regular-follow up for 2 years.
Conclusions:
No malignant germ cells were found in the final surgical pathology evaluation, and a mature teratoma was present, which confirmed the diagnosis. Awareness, early diagnosis, and finally, prompt and complete surgical resection of the tumor is critical for a good treatment outcome.
Introduction:
Growing teratoma syndrome (GTS) is an uncommon condition identified in both testicular and ovarian carcinomas. The occurrence of GTS after testicular nonseminomatous germ-cell tumors (NSGCT) is 1.9%–7.6%, while, within the setting of ovarian germ-cell neoplasias, GTS is obscure. 1 GTS is manifested by an expansion in metastatic mass brought about by the development of a mature teratoma with no germ-cell tumor during or after chemotherapy. This case is reported to highlight the diagnostic and management challenges often associated with GTS.
Case
A 25-year-old, second gravida female had been managed as an outpatient at 10 weeks of gestation in February of 2017. She underwent an open, right ovarian cystectomy for a mass measuring 14 × 10 × 9 cm. The histopathologic examination (HPE) report was suggestive of an immature teratoma.
In July 2017, at 8 months of gestation, she presented with acute breathlessness and abdominal distension. Ultrasonography (USG) was performed, which suggested a 11 × 9–cm, complex solid mass in the right adnexa and another 8 × 10-cm solid mass in the pelvis. Her serum α-fetoprotein (α-FP) level was 2911 ng/mL. Her ß–human chorionic gonadotropin (ß-hCG) and serum lactate dehydrogenase (LDH) were normal. A cesarean hysterectomy with a bilateral salpingo-oophorectomy with an omentectomy were done in July 2017 elsewhere. A live male child was born (2.17kg), but the child died 6 days after birth. The HPE report was suggestive of an immature teratoma (Norris grade 2–3) involving the right adnexa, right parametrium, uterine serosa, and omentum. The left ovary and parametrium were unremarkable. Postoperatively, her serum α-FP level was 2180 ng/mL. Three cycles of bleomycin, etoposide and cisplatin (BEP) were administered up to October 2017 elsewhere. Postchemotherapy, imaging, and tumor markers showed no evidence of disease.
This patient then presented at The Gujarat Cancer Research & Institute (GCRI), in Ahmedabad, India, for the first time in November 2017. She had severe breathlessness and abdominal distension. On clinical examination, a huge mass was palpable involving the entire abdomen. Her serum α-FP level was 9.7 ng/mL and her serum ß-hCG and lactate dehydrogenase were within normal limits. A computed tomography (CT) scan of her thorax, abdomen, and pelvis showed a 19 × 12 × 37–cm mass in the right side of her abdomen extending from the right iliac fossa and up to the right subdiaphragmatic surface (Fig 1). A 13 × 10 × 7–cm mass was also present along the peritoneal surface of the left lobe of her liver. A 2 × 3–cm pleural-based soft-tissue density was noted in the postero–basal segment of the left lower lobe of her lung. USG-guided biopsy of tissue from the abdominal mass was suggestive of a mature cystic teratoma.

Axial computed tomography abdomen plain image.
Debulking surgery was planned with the surgical oncology team. Removal of the huge mass—measuring 32 × 26 × 14 cm from the right iliac fossa up to the right subdiaphragmatic surface—with removal of another mass—measuring 20 × 16 × 10 cm—was performed. The pelvic masses of 10 × 8 × 5 and 9 × 5 × 4 cm were removed. A mass, measuring 3 × 2 × 1 cm, from the right lower lobe of the lung was removed through the diaphragmatic approach. The patient developed intraoperative hypotension after 6 hours of this extensive surgery. She was started on inotropes and other supportive measures. Further surgery was deferred in view of the unstable condition of this patient.
Results
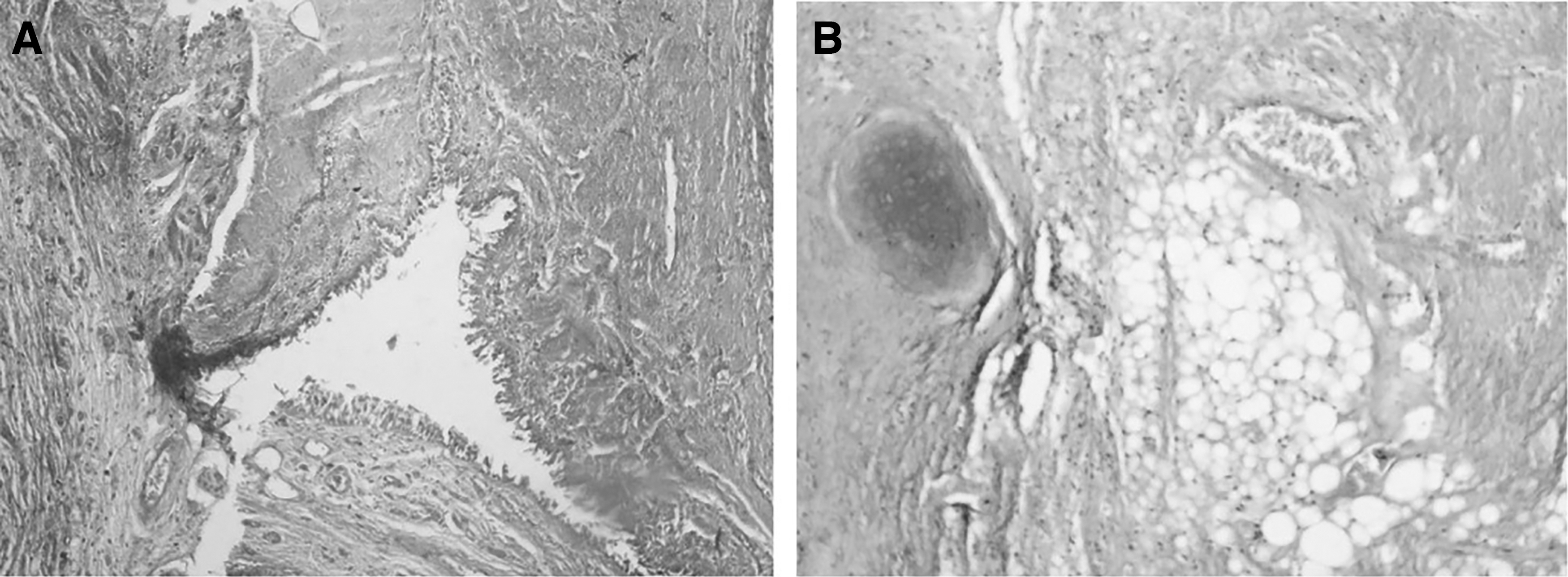
Postoperatively, this patient was stabilized. The final HPE report described a mature cystic teratoma with respiratory epithelium, adipose tissue, and mature cartilage in a background of benign stroma with no evidence of malignancy (Fig. 2).
Six weeks later, on clinical examination an irregular firm 4-cm mass was felt at the vault. CT of her whole abdomen showed an 8 × 13-cm fat-to-fluid–density lesion in the left hypochondriac region, abutting the left lobe of her liver with a loss of the fat plane with a similar characteristic lesion of 7 × 4.8 cm in her pelvis posterior to her urinary bladder. USG-guided biopsy of the mass was suggestive of a mature cystic teratoma. After thorough counseling the patient and her relatives, regarding the extensive surgery needed and the associated risks and comorbidities, she underwent cytoreductive surgery in February of 2018. The final HPE report suggested a mature cystic teratoma. With regular follow-ups, this patient has been disease-free for 2 years.
Discussion
Growing teratoma syndrome (GTS) was first described by DiSaia et al. in 1977 as “chemotherapeutic retroconversion.”
2
The definition of GTS according to Logothetis et al.'s criteria is as follows
3
:
Normalization of serum tumor markers, α-FP, and hCG Enlarging or new masses despite appropriate chemotherapy for NSGCT Exclusive presence of a mature teratoma in the resected specimen.
Chemotherapy causes growth of mature, benign teratomatous elements, but it cures immature malignant cells. Chemotherapy alters the cell kinetics and helps in transformation from a totipotent malignant germ cell to a benign mature teratoma. 1 Growing teratomas are considered to be benign; they expand rapidly with a median linear growth of ∼0.5–0.7 cm/month and a volume increase of 9.2–12.9 cm3/month. They have variable growth patterns.4,5 Aggressive local spreading and malignant degeneration make a GTS an unpredictable tumor.3,4,6 The retroperitoneum is reported to be the most-common site of this syndrome. Other sites are cervical lymph nodes, lungs, inguinal lymph nodes, supraclavicular lymph nodes, mesentery, forearm, perineal glands, and liver.7,8. Higher curative rates are achieved by surgical treatment and a lower recurrence rate is reported if there is no residual disease left.4,9,10
The current patient came with widespread disease and was in poor general condition. A team approach, including a surgical oncologist, an anesthetist, and an intensivist in a well-equipped intensive care unit, are vital for a successful outcome in such a case. An experienced gynecologic–oncologic pathologist's opinion is required to arrive at a final diagnosis of GTS. Inadequate and incomplete resections can lead to local recurrences. 4 Involvement of a vascular structure or other organs is not considered as a contraindication for surgery. 9
Speiss et al. reported on a study in which the patients who underwent complete resections had 89%–90% of 5-year overall survival. 4 No medical treatment for GTS has proven effective as of this writing; however, interferon (IFN) therapy has been found to play some role. Tonki et al. reported on an inoperable abdominal GTS case wherein the disease was managed with IFN for 8 years. 11 Mego et al. reported a case of partially resectable disease, in which the patient had noteworthy clinical improvement with bevacizumab used biweekly for 6 months. 12
Conclusions
Awareness of GTS, prompt imaging of patients undergoing chemotherapy for NSGCTs, early recognition of the paradoxical response of the disease to chemotherapy (enlarging tumors and normal serum tumor markers), early diagnosis, and swift and complete surgical resection of tumors are critical for good treatment outcomes.
Footnotes
Acknowledgments
The authors appreciate the index patient for agreeing and consenting to her information to be used in this case report.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this study.