
Abstract
Background:
Large leiomyomas can outgrow their blood supplies leading to cascades of inflammatory reactions and ischemic changes resulting in various kinds of degeneration. Massive cystic degeneration might mimic an ovarian cyst, posing a diagnostic dilemma. This article presents a case of a woman with marked cystic degeneration of a uterine leiomyoma mimicking an ovarian neoplasm.
Case:
A 42-year-old woman presented to the gynecology outpatient clinic of SRM Medical College Hospital and Research Centre, SRM Nagar, Chengalpattu District, Tamil Nadu, India. She had a huge abdominopelvic mass. Clinically and radiologically, the mass was suspected to be an ovarian neoplasm. This patient's tumor markers were normal. Intraoperatively, a huge mass filling the entire abdominal cavity was seen. The mass was decompressed and 4.5 L of serous fluid were drained. It was attached to the posterolateral wall of the uterus and left ovary. She underwent a total abdominal hysterectomy, a bilateral salpingo-oophorectomy, and an infracolic omentectomy
Results:
Histopathology confirmed a final diagnosis of a degenerated leiomyoma. The patient's postoperative course was uneventful and she was discharged on her eighth postoperative day.
Conclusions:
When a patient has a huge pelvic mass, cystic degeneration of this fibroid mass should be retained as a differential diagnosis prior to surgical intervention.
Introduction
Leiomyoma of the uterus is the most-common benign tumor arising from uterine smooth muscle. The sizes of leiomyomas vary from being microscopic to being giant; giant myomas are exceedingly rare. As leiomyomas enlarge, they outgrow their blood supplies, which can lead to cascades of inflammatory reactions and ischemic changes that result in various kinds of degeneration, such as hyaline, cystic, myxoid, or red degeneration. Hyaline cystic degeneration is relatively rare and has been observed in ∼4% of leiomyomas. 1 Massive cystic degeneration can mimic ovarian cysts, posing diagnostic dilemmas. This article presents a case of a woman with marked cystic degeneration of an exophytic uterine leiomyoma mimicking an ovarian neoplasm.
Case
A 42-year-old woman presented to the gynecology outpatient clinic of the SRM Medical College Hospital and Research Centre, in SRM Nagar, Kattankulathur, Chengalpattu District, Tamil Nadu, India. She had abdominal distension for 1 week prior with occasional abdominal pain. She also experienced loss of appetite for 2 months. She was a nulligravida who had been evaluated for primary infertility 10 years prior. Her menstrual cycles were regular with no dysmenorrhea. There was no other significant medical history. Her general condition was fair with mild pallor with no evidence of any lymphadenopathy. On clinical examination a huge nontender abdominopelvic mass soft to cystic in consistency was palpated extending up to the xiphi sternum with restricted mobility. On bimanual examination it was difficult to differentiate the mass from the uterus. Clinically, the mass was suspected to be an ovarian mass.
Ultrasonography (USG) showed a large (20 × 16 cm) cystic mass, with multiple thin septations, internal echoes, and solid components, arising from the pelvis and occupying the entire abdominal cavity (Figs 1 and 2). The uterus was normal with a thin endometrium. The right ovary was normal, but the left ovary could not be visualized. Thus, a provisional diagnosis of a left ovarian tumor was made. Tumor-marker levels, such as cancer antigen–125–28.96 U/mL and carcinoembryonic antigen–1.610 ng/mL, were normal.

Ultrasound image showing cystic tumor with multiple septations and internal echoes.

Ultrasound image showing a part of the tumor with a solid component.
Subsequently, she underwent a laparotomy that revealed the large ovarian mass extending from the pelvis up to the lower border of her rib cage and occupying the entire abdomen. Due to the difficulty involved in removing this huge mass from the abdominal cavity, the mass was decompressed by making a small incision in it. A suction cannula was inserted, and 4.5 L of serous fluid were drained, with precautions taken to avoid any spillage.
The patient's uterus was normal with normal right adnexa. The huge mass was attached on the left side to the posterolateral wall of the uterus along with the left ovary (Figs. 3 and 4). The consistency of this mass was variegated and predominantly cystic. There was minimal free fluid in the pelvis. Subsequently, the patient underwent a total abdominal hysterectomy, a bilateral salpingo-oophorectomy, and an infracolic omentectomy. The pelvic and para-aortic nodes were not palpable. Peritoneal fluid was sent for cytological examination to rule out malignancy.
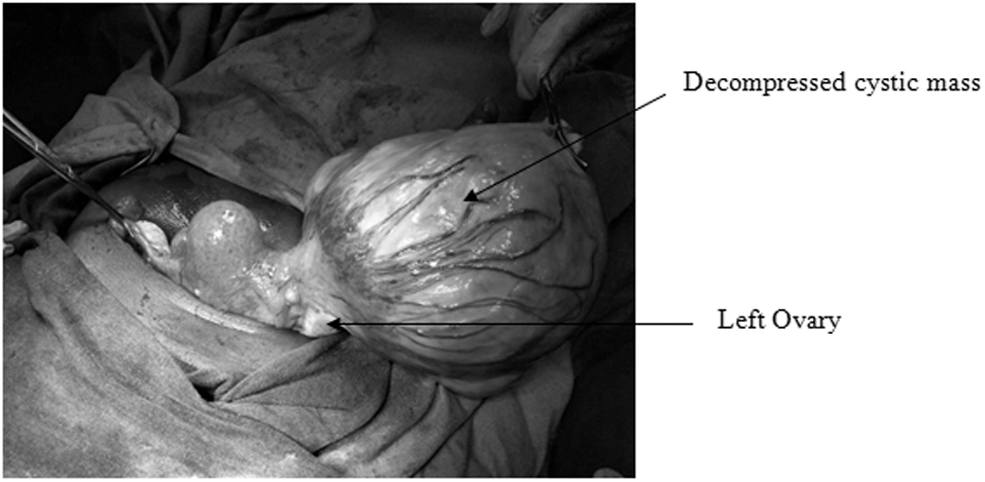
Decompressed cystic mass with pedunculated attachment to the uterus and left ovary.
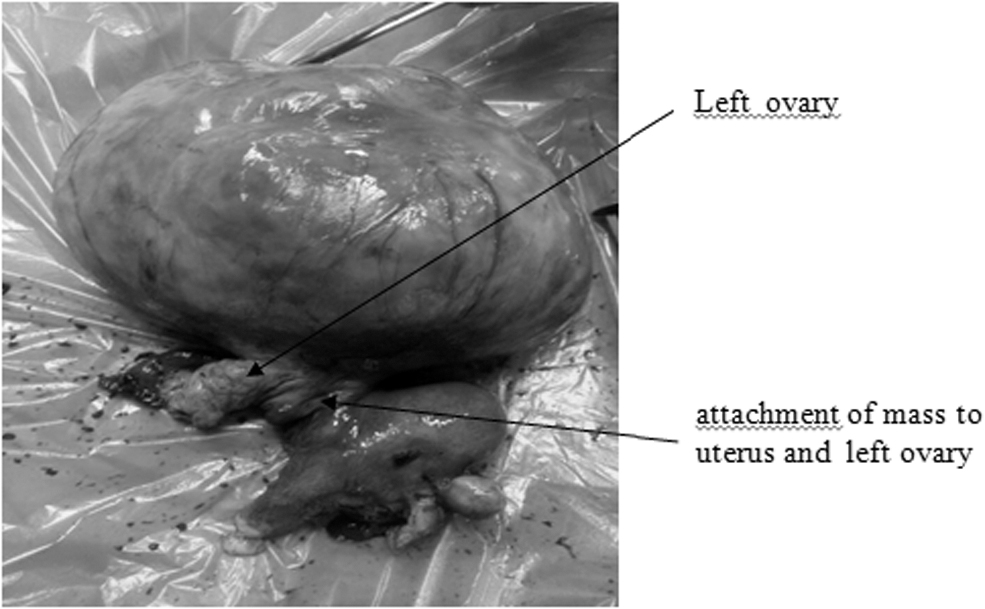
Hysterectomy specimen: Cystic mass with attachments to both the uterus and the ovary.
Results
This patient's postoperative course was uneventful, and she was discharged on her eighth postoperative day. Histopathological examination showed that the mass was a subserous leiomyoma with hyaline and myxoid degeneration.
Discussion
As leiomyomas enlarge, they can outgrow their blood supplies, inducing a series of inflammatory responses and ischemic changes that result in various kinds of degeneration, including hyaline, cystic, myxoid, or red degeneration; and dystrophic calcification. Degenerative or secondary changes are detectable in ∼65% of uterine leiomyomas as follows: hyaline degeneration (63%); myxoid changes (19%); calcification (8%); cystic changes (4%); fatty degeneration (3%); and red degeneration (3%). 1 Cystic degeneration is mainly a pseudocyst derived from liquefaction of hyaline changes (in the late stages). Pedunculation of a subserosal fibroid can compromise the blood supply of the fibroid and play a role in the pathogenesis of cystic degeneration.2,3
Typical cases of leiomyoma are easy to identify radiologically. However, uterine leiomyomas altered by degenerative changes, can be misdiagnosed. On USG, leiomyomas are characterized by homogeneous or heterogeneous hypoechoic masses, but, with cystic degeneration, a fibroid can have a variegated appearance. The fibroid can mimic an ovarian cyst, an endometrioma, or an abscess.4,5 There are few case reports of degenerative fibroids mimicking ovarian carcinomas.3,6–8 Clinical features and investigations have mimicked ovarian tumors and the diagnoses were made intraoperatively. So far, fewer than 20 cases of degenerated leiomyomas mimicking ovarian tumors have been reported in the literature.
Anyanvu et al. reported 2 case series of cystic degeneration in pregnant and nonpregnant women. 9 In 1 of these cases, there was a combination of three kinds of degeneration (hyaline, cystic, and myxoid), which is extremely rare; 8.2 L of fluid were drained from that fibroid. 9
Bhardwaj et al. reported a case of massive cystic degeneration of a fibroid that was aspirated laparoscopically; the surgeons then proceeded with a hysterectomy. 10 Enakpene et al. reported the largest leiomyoma with cystic degeneration (containing 11 L of serous fluid) in a nulliparous woman whose case was managed with fertility-preserving surgery. 11
The first differential diagnosis of a large cystic mass with irregular septae and solid components filling the pelvic cavity is ovarian malignancy. This can be ruled out by visualizing normal ovaries or continuity of the mass with the uterus on imaging. Absence of ascites and elevated tumor markers may favor a diagnosis of a leiomyoma. The ovarian vascular pedicle sign noted on computed tomography (CT) is another way to confirm the ovarian origin of a pelvic mass and for differentiating the mass from a subserosal uterine fibroid. 12
Maizlin et al. reported a case in which the sonographic features supported the diagnosis of an ovarian tumor but magnetic resonance imaging (MRI) aided the preoperative diagnosis of cystic degenerations of fibroids. 13 In the current patient's left ovary also could not be visualized on USG. Thus, the role of MRI in choosing the preoperative diagnosis cannot be overemphasized and MRI should be performed in all cases when there are huge cystic masses and adnexae are not visualized. Yorita et al., in a review article, noted that, among 17 cases mimicking ovarian tumors, most (70%) were actually subserosal pedunculated masses and 6 cases had multilocular cystic morphology. All 12 ovarian tumorlike uterine leiomyomas could not be clinically diagnosed using imaging modalities, such as ultrasound, CT and/or MRI, partly because of their failure to show the stalk of the pedunculated fibroids. 14
This case was presented here because of its rarity. Even intraoperatively, the mass was suspected to be a ovarian mass as it was attached to one ovary and to the uterus. Only histopathology testing confirmed the final diagnosis of a degenerated leiomyoma.
Conclusions
Extensive cystic degeneration in leiomyomas can result in unusual presentations and diagnostic dilemmas. Cystic degeneration of a fibroid should be retained as a differential diagnosis prior to surgical interventions for such type of huge pelvic masses.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this work.