
Abstract
Background:
This article describes a very rare entity—a mature cystic teratoma occurring in the retroperitoneum in a postmenopausal patient, which is also a rare age for this presentation.
Case:
A 51-year-old postmenopausal woman presented with a history of low-back pain that radiated to a lower limb. During her evaluation, a mature cystic teratoma was found in the retroperitoneal region with calcification. She was operated on to remove adhesions that she had and to remove the teratoma.
Results:
This patient's low-back pain was resolved after her operation.
Conclusions:
Although rare, a retroperitoneal teratoma can present in postmenopause, usually in a patient with nonspecific complaints. At this age of presentation, malignancy should always be ruled out by surgical excision and careful histologic examination of the excised specimen.
Introduction
Mature cystic teratomas are rare germ-cell tumors of the ovary, comprised of all germ-cell layers—ectoderm, mesoderm, and endoderm. 1 These tumors account for ∼25% of all ovarian tumors but not more than 5% of malignant ovarian tumors. Mature cystic teratomas often occur in younger patients, with an average age of 30. 1 These tumors are typically evident within the pelvis because of their fat and calcific density.1,2 The presenting case is a rare retroperitoneal teratoma in an older woman. These tumors are uncommon in postmenopausal patients. In addition, this case also demonstrates the detection of the tumor and the proper referral of a female patient with a calcific mass.
Case
A 51-year-old, para 4, postmenopausal female (menopause attained 9 years back) was referred from an orthopedic department for a 2-month history of low-back pain, after exclusion of musculoskeletal and neurologic causes and a finding of a right pelvic mass with bone formation noted on a KUB [kidneys, ureters, and bladder] X-ray (Fig. 1).

KUB [kidneys, ureters, and bladder] X-ray film where the arrow points to the irregular calcification pattern of a retroperitoneal teratoma.
This patient complained of a dull, aching lower-back pain with right lower-limb numbness that was not associated with abdominal pain, change in bowel habits, urinary symptoms, nor vaginal discharge.
Her general physical examination was unremarkable, and her body mass index was 24. Systemic and neurologic examinations yielded normal findings. On abdominal examination, this patient's abdomen was soft with no guarding nor rigidity. There was a nontender, smooth-surfaced, firm lump, 10 × 8 cm, with restricted mobility that was palpated in the right iliac fossa. Pelvic examination showed a normal-size uterus with a mass in the anterior and right fornixes.
Pelvic ultrasound showed a right ovarian mass of 10.5 cm in diameter with echogenic shadowing that indicated a calcified component. All laboratory investigations, including tumor markers, such as cancer antigen (CA)–125, α-fetoprotein, and CA 19-9 were 30.2 U/mL, 4 ng/mL, and 25 U/mL, respectively—within normal ranges.
With a preoperative diagnosis of an ovarian tumor in this postmenopausal woman, she was counseled about a total laparoscopic hysterectomy (TLH) with a bilateral salpingo-oophorectomy (BSO).
A 4-handed surgery was started through the Lee–Huang point. Intraoperative findings showed a normal-size uterus, a normal left ovary, and a right retroperitoneal mass of ∼10 cm in diameter reaching the presacral region. The mass was densely adhered to the rectum and right ureter. First, adhesiolysis was done to identify the rectum and right ureter. Then, the retroperitoneal mass was excised using LigaSuretm and a monopolar scissor to cut the bony elements and calcified tissue. After that, a TLH and a left salpingo-oophorectomy were performed. During the operation, bleeding in the presacral region was controlled with hemoclips (Fig. 2).
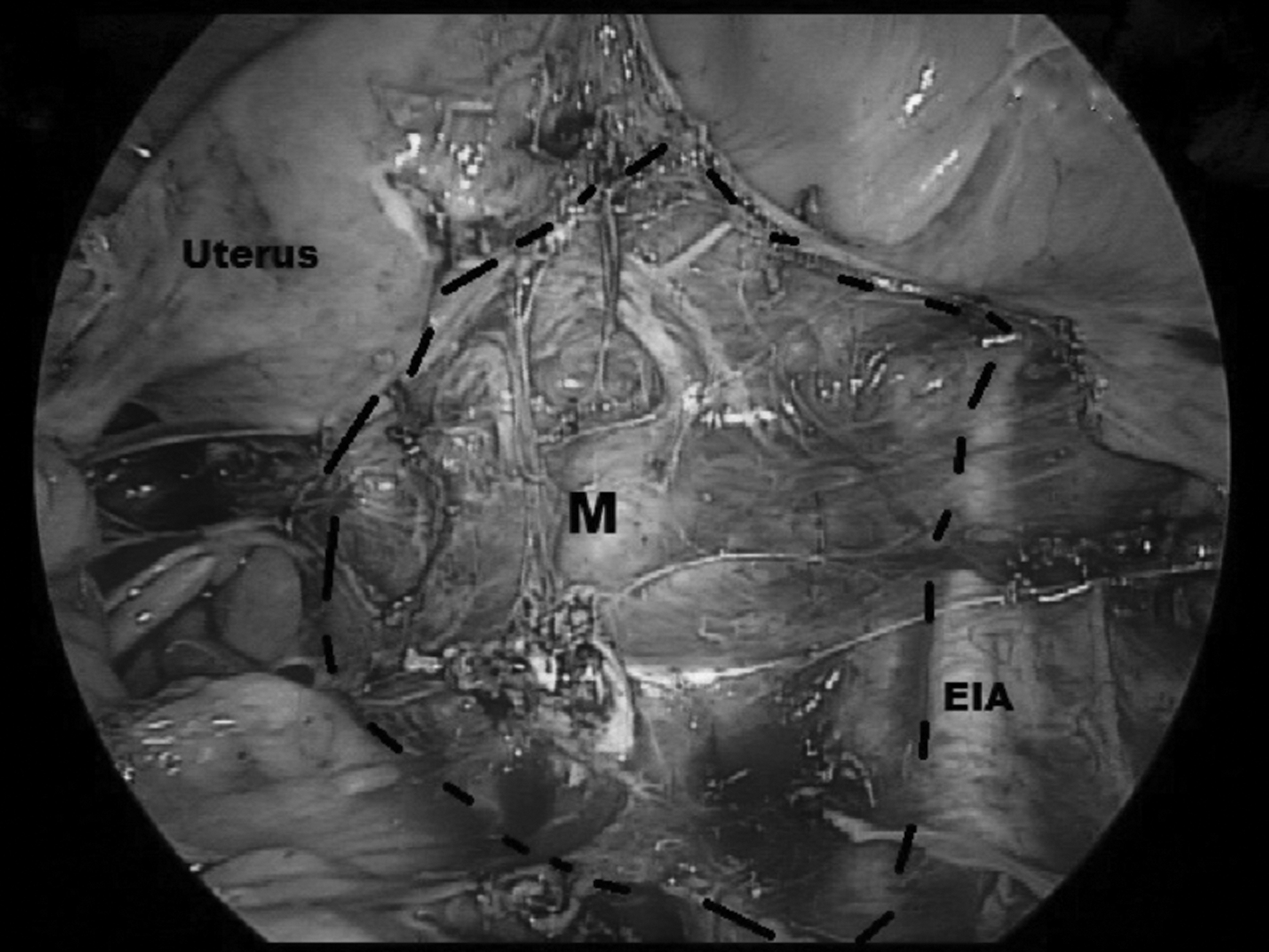
Laparoscopic view of the pelvis showing the uterus, M represents the retroperitoneal teratoma with its border demarcated by black short lines, reaching the right external iliac artery (EIA), with obliteration of the cul de sac.
The gross specimen was comprised of 2 pieces of tissue measuring 8.3 × 5.7 × 5.5 cm and 6.3 × 1.9 × 1.4 cm (Fig. 3). There was hair, fatty tissue, bony tissue, and sebaceous content inside the mass. A histopathology examination revealed a cystic tumor comprised of squamous epithelium, respiratory-type ciliated columnar epithelium, skin appendages, mature fat tissue, lamellar bone with bone-marrow spaces, and some melanin pigments–all indicating that the mass was a mature cystic teratoma.

The gross specimen showed that the calcified retroperitoneal teratoma was ∼9 cm.
Results
This patient's low back pain was relieved after her operation.
Discussion
Teratomas are germ-cell tumors that develop from the 3 embryonic germ cell layers. 1 Grossly, teratomas might be cystic or solid. Cystic teratomas are composed of completely mature parts and include sebaceous material and hair. These tumors are mostly benign. Solid teratomas, in most cases, are malignant and comprised of immature embryonic tissue. 3 Many researchers reported that 1% of mature cystic teratomas undergo malignant transformation, mostly into squamous-cell carcinoma. 4
Extragonadal teratomas are suggested to arise from primordial germ cells or early embryonic cells5,6; some of these tumors are primary retroperitoneal teratomas. These teratomas represent ∼1%–11% of all retroperitoneal tumors. They appear most commonly in neonates and young adults. 7 These teratomas have a bimodal age peak, as they tend to occur in the first 6 months of life and in early adulthood. Approximately 43%–55% of retroperitoneal teratomas are diagnosed within the first year of life, and less than 10%–20% present in patients older than 30. 8
Benign teratomas are usually diagnosed as incidental findings, unless these teratomas grow large, causing obstructive symptoms to develop. However, common presenting symptoms include back pain or abdominal pain. 9
Many radiologic findings can indicate the diagnosis of teratoma, such as a complex lesion containing a well-circumscribed fluid component, fatty regions, and calcifications. 10 In more than half of these cases, plain X-ray films can show irregular calcifications, representing a calcific rim of the cyst wall or even a calcific structure, such as a tooth or a bony element. 11 Approximately 12.5% of calcified tumors are malignant. 3 However, a definitive diagnosis can only be made after surgical resection and careful histologic evaluation of the excised mass. 10 As the current patient was postmenopausal, a TLH and a BSO were performed.
Conclusions
A retroperitoneal teratoma is a rare development. Although most commonly encountered in infants, children, and young adults, it can also present in a postmenopausal woman with nonspecific complaints. Malignancy should always be ruled out by surgical excision and careful histopathologic examination of the excised specimen.
Footnotes
Acknowledgments
The authors thank the Asia-Pacific Association for Gynecologic Endoscopy and Minimally Invasive Therapy for providing the International Fellowship Endoscopy Training Program at Chang Gung Memorial Hospital at Linkou, Kweishan, Taoyuan, Taiwan.
Funding Information
No funding was received from any agency or institution.