
Abstract
Objective:
The aim of this research was to review preoperative and intraoperative findings in patients with rectus muscle endometriosis (RME) and to describe the current authors' novel technique of laparoscopic excision of RME.
Materials and Methods:
This was a retrospective case series at a single academic institution. The operations in this series were conducted between January 2009 and January 2019. RME was excised laparoscopically or by an open approach, with or without diagnostic laparoscopy to evaluate for pelvic endometriosis. Demographic and perioperative data were obtained from the medical records, and descriptive statistics were generated.
Results:
Twenty-two patients were included in the analysis. Each of 21 (95%) patients had at least 1 prior cesarean section, and 5 patients each (23%) had a prior excision of abdominal wall endometriosis. All patients reported pelvic or abdominal pain and three-quarters of them reported cyclic pain. One-quarter complained of masses or lumps; however, only 55% had palpable nodules felt on abdominal examinations. All but 1 patient had preoperative imaging, of which 81% were magnetic resonance imaging. Of the 22 cases, 11 (50%) lesions were excised laparoscopically and 11 (50%) were excised with open excision. In 3 patients who had open excisions, laparoscopic evaluation of each patient's pelvis was also performed. Concurrent pelvic endometriosis was present in 71.4% of patients who underwent laparoscopy, with the most-common location being the bladder or ureter (60%). All cases of laparoscopic excision of RME were performed by a minimally invasive gynecologic surgeon. Ninety-four percent of patients reported having complete symptom relief at their postoperative visits.
Conclusions:
Both open and laparoscopic resection of RME are feasible treatment options and the surgical approach should be determined by specific symptoms, physical examination, and preoperative imaging. Due to the high incidence of concurrent pelvic endometriosis, laparoscopic evaluation of the pelvis should be considered when excision is planned using an open approach.
Introduction
Rectus muscle endometriosis (RME) is defined as a specific form of abdominal wall endometriosis (AWE) whereby ectopic endometrial tissue is found within the rectus muscle body. 1 RME is a subtype of AWE, which can be found in any layer of the abdominal wall, and is most-commonly found in the scar tissue of Pfannenstiel incisions, laparoscopic port sites, or hernia repairs. 2 RME can be isolated without the involvement of other layers of the abdominal wall but can also be an extension of endometriosis from subcutaneous tissue through the fascia into the muscle.1,2 Ecker et al. stated that the rectus muscle is involved in 17% of cases of AWE. 2
Patients with RME may have cyclic localized abdominal pain and a tender mass similar to patients with AWE. A palpable tender abdominal wall mass is not always felt by the patients or the surgeons. Some patients with RME also have typical endometriosis symptoms, including dysmenorrhea, dyspareunia, or dyschezia. Patients frequently report worsening pain with activities that strain the rectus muscle including, coughing, Valsalva maneuvers, or abdominal crunches. Preoperative imaging with ultrasound (US), computed tomography, or magnetic resonance imaging (MRI) is helpful when RME is suspected to evaluate the extent of fascial involvement 2 (Fig. 1). If the differential diagnosis is broad, a biopsy can be performed prior to surgical management. 3
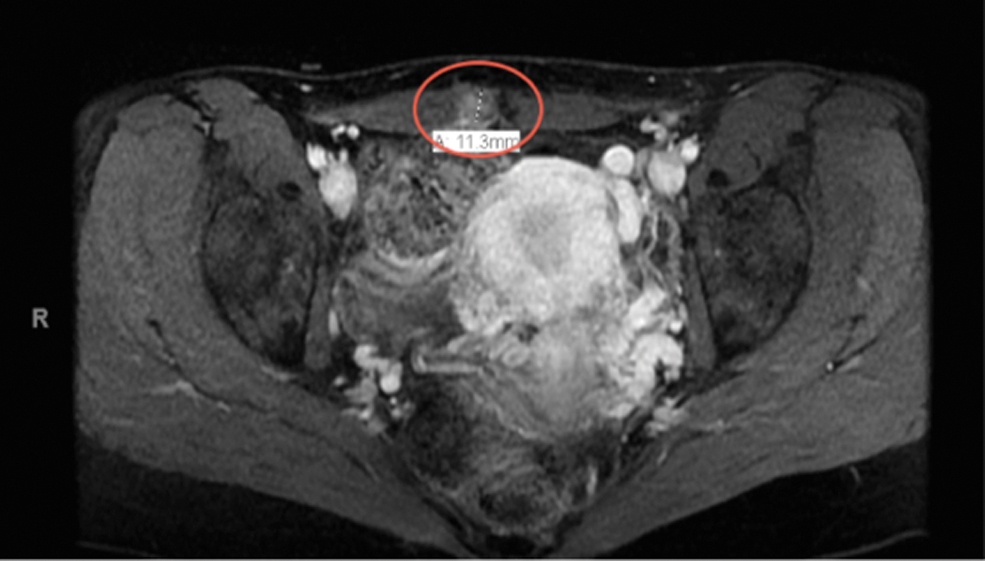
Magnetic resonance imaging revealing rectus muscle endometriosis. Color images are available online.
Experts have historically recommended wide local excision using an open approach as the treatment of choice for RME.1,4,5 However, Ecker et al. first described a laparoscopic approach to remove AWE, specifically for lesions involving the rectus muscle as opposed to AWE isolated in the subcutaneous layers.1,2 The rectus muscle is easy to access laparoscopically, and this technique minimizes disruption to the fascia. When patients undergo laparoscopic excision they also benefit from the known advantages of minimally invasive surgery, including shorter hospital admissions, lower infection rates, and faster recoveries. This technique is also feasible for larger fascial defects requiring mesh, which can be placed laparoscopically.1,2,4
The purpose of this study was to present a case series of patients who underwent surgical excision of RME and to define preoperative characteristics that can determine surgical approaches. This study was unique because the current authors' novel laparoscopic approach to RME has not yet been discussed in the literature. The goal was to describe a new technique for resection, so that women will have the benefits of minimally invasive surgery in appropriate cases.
Materials and Methods
Subjects and methods
Following approval by the University of Pittsburgh's institutional review board (approved: February 15, 2019; study number: 19010069), a retrospective review was performed of all patients with RME at the University of Pittsburgh Medical Center (UPMC) between January 2009 and January 2019. Surgical calendars and pathology records were utilized to identify patients who underwent surgical excision of RME. The electronic medical records were reviewed for demographic information, presenting symptoms, medical and surgical histories, therapy attempted, imaging findings, surgical findings and approaches, length of hospital stays, and complications. The study included patients who were at least 18 years old and had pathologic confirmation of endometriosis involving the rectus muscle. The study excluded patients who met these criteria but did not follow-up within 4 or more weeks. Mode of surgery was defined as either laparoscopic or open and was characterized by how the rectus muscle endometriosis was removed. It was also recorded if surgeons performed evaluations of each patient's pelvis via laparoscopy in addition to open RME resection. The study was not powered to detect a difference between groups. A dedicated gynecologic pathologist reviewed all pathology reports.
Statistics
Descriptive statistical analysis was performed with STATA, version 15, software. Continuous data were reported as mean and standard deviation when normally distributed, and as median and interquartile range when not normally distributed.
Abdominal approach to rectus muscle endometriosis
The nodule is palpated and marked. A horizontal skin incision is made above the nodule. The subcutaneous tissue is dissected until the nodule is exposed. The nodule is then elevated using a towel clamp or other sharp clamp. The borders of the nodule are identified using tactile feedback against the fibrosis (the “squeeze technique”) and blunt dissection, which can be performed with an HARMONIC® scalpel or advanced bipolar devices such as LigaSuretm or Enseal.® A curved hemostat is used to delineate the borders of the nodule and the subcutaneous, fascial, and rectus tissue is dissected off the nodule along the hemostat. Once the entire nodule is removed, the fascial defect is closed using a monofilament-delayed absorbable suture in a “figure-of-eight” fashion. When a nodule on imaging appears too large to reapproximate the facial defect, a preoperative consult to general surgery or plastic surgery can be placed to assist with closure with or without mesh.
Laparoscopic approach to rectus muscle
A peritoneal incision is made at the suspected site along the anterior abdominal wall. Typically, a patient will have had an MRI to guide the procedure when the nodule is not palpable. Bony landmarks—such as the anterior superior iliac spine (ASIS) and symphysis pubis—in the MRI images are used to determine the location of the nodule when this occurs. Smaller lesions might require an US-guided needle localization preoperatively. The incision is enlarged in all directions, paying close attention to the inferior epigastric vessels and the dome of the bladder. In cases when the endometriosis is low in the pelvis, the space of Retzius is dissected to drop the bladder away from the lesion of interest. Port placement is dependent on the location of the nodule: for RME caudal to the ASIS, visualization with the umbilical port is appropriate; for lesions cephalad to the ASIS, a subxiphoid port should be utilized for better visualization and ease of excision. A 45°-angled laparoscope is helpful for viewing the pathology on the anterior abdominal wall better.
During dissection, the bipolar energy device is used through the suprapubic, umbilical, or subxiphoid ports, with the lateral ports providing countertraction. Using a combination of sharp and blunt dissections, the lesion of endometriosis and surrounding fibrosis is enucleated and excised from the surrounding muscle. With downward traction on the endometriosis lesions from the lateral assistant ports, tactile feedback against the fibrosis (the same squeeze technique as mentioned above) helps delineate the margins of the lesion. Bipolar devices are not able to cut through the diseased tissue, given the significant resistance from fibrosis, and the surrounding normal tissue offers no resistance, so this technique enucleates the nodule naturally.
After the lesion is excised, the fascia is inspected. When the fascia is intact, no additional steps are necessary. 6 A small fascial defect can be repaired with interrupted delayed absorbable sutures with a Carter–Thompson Suture Closure Device under direct visualization. A large defect (> 3 cm) can be repaired by securing mesh to the edge of the fascial defect with absorbable tacks and additional sutures if necessary (Fig. 2). In addition, an omental patch can be sutured to the mesh as a barrier to bowel adhesions. In patients with RME with large facial defects requiring mesh placement, concurrent hysterectomy is not recommended due to contamination of the mesh from vaginal flora.

Case of rectus muscle endometriosis requiring mesh repair (3 views).
Results
The study population included 22 cases of RME. The median age was 34 years (31.5–37.75). All but 1 patient were multiparous and had at least 1 prior cesarean section, and 59% had 2 or more prior cesarean sections (Table 1). Of the 22 cases, 11 (50%) were excised laparoscopically and 11 (50%) were excised with an open approach (Table 1). No cases were lost to follow-up.
Baseline Characteristics of Women with Rectus Muscle Endometriosis
IQR, interquartile range; BMI, body mass index; CS, cesarean section(s); AWE, abdominal wall endometriosis; MRI, magnetic resonance imaging; US, ultrasound, CT, computed tomography; IR, infrared; bx, biopsy.
All of the patients presented with pelvic or abdominal pain, with 77% having pain that was cyclic in nature (Table 2). Pain that was triggered by coughing, sneezing, or performing a sit-up was more common in the laparoscopic cohort. On examination, 8 (72.7%) patients undergoing open excision had palpable nodules and 8 (72.7%) experienced focal abdominal tenderness, compared to patients undergoing laparoscopy (4 [36.3%] and 9 [81.8%], respectively). All but 1 patient had imaging, the vast majority of which was MRI. Only 45.5% of the cases excised laparoscopically involved the fascia, as opposed to 100% of open-excision cases (Table 3). Overall, 6 patients required mesh placement to repair their fascial defects, 4 in the open-excision cohort and 2 in the laparoscopy cohort. Minimally invasive gynecologic surgeons performed all 11 (100%) of the laparoscopically excised RME cases (Table 3).
Presentation and Location of Symptoms
RLQ, right lower quadrant; LLQ, left lower quadrant.
Intraoperative and Postoperative Findings
SD, standard deviations; MIGS, minimally invasive gynecologic surgeon; OBGYN, obstetrics/gynecology.
A total of 14 patients underwent laparoscopic evaluation of the pelvis and 10 (71.4%) of those patients had endometriosis excised and confirmed by pathology. Of the open-excision cases, 3 (27.3%) underwent laparoscopic evaluation of the pelvis. Pelvic endometriosis was most commonly found on the bladder or ureters. Besides the urinary tract, endometriosis was most-often identified on bilateral uterosacral ligaments, and in the rectovaginal and perirectal spaces. Regardless of the route of RME excision, there were no intraoperative complications. All of the patients who underwent laparoscopic excision went home on the day of surgery. Of those cases who were admitted to the hospital, the hospital stay was between 1 and 4 days. There were 3 complications within 30 days in the combined-approach group, 2 of which were surgical-site infections, and the other was a superficial wound separation without evidence of infection. One patient in the laparoscopic group developed an incisional hernia 1.5 years later that ultimately required repair with mesh. At the postoperative visits, all but 1 patient reported pain relief (Table 3).
Discussion
The current study was unique because it was the largest case series specifically describing RME and laparoscopic removal of RME. Until this case series, the vast majority of cases in the literature described open, wide local excision, and not laparoscopy.1,4,5,7 Ecker et al. published the first case series describing laparoscopic excision of AWE. 2 The current series built upon their findings but exclusively focused on cases of RME, as these cases have clinical features that are different from AWE. The decision to approach RME laparoscopically or with an open approach depends on where the bulk of the endometriosis lies. If the bulk of the endometriosis is in the subcutaneous tissue, an open incision is preferred. Endometriosis isolated to the rectus muscle should be approached laparoscopically, as the disease burden is within the peritoneal cavity. The current study showed that rectus muscle endometriosis that involves some subcutaneous tissue is still amenable to a laparoscopic approach (Figs. 1 and 3). The current series also demonstrated that fascial defects can be repaired laparoscopically with or without mesh, whereas previous literature described mesh repair solely when using an open approach. 4

Laparoscopic resection of rectus muscle endometriosis (2 views).
The clinical features of RME vary based on the location of the disease, and this can help guide surgical planning. All of the patients in the current study presented with pelvic or abdominal pain, and the majority specifically cited having cyclic pain. This differs from cases mentioned in the literature wherein approximately one-third of cases presented with both cyclic pain and an associated mass. 4 Although all of the current study's patients presented with pain, 91% had focal abdominal tenderness noted on examination and only 54% had palpable nodules. The lower rate of palpable nodules might be due to the subfascial location of disease, compared to more superficial AWE. Moreover, the lack of a palpable mass can potentially lead to a delay in diagnosis. When a patient presents with cyclic abdominal wall pain consistent with AWE but no palpable mass is felt, the provider should consider RME as the differential diagnosis.
Imaging, specifically MRI, can provide information on the size, depth, and involvement of the fascia to assist in surgical planning. 4 Although MRI is more expensive, the images enable the surgeon to choose the best approach and to anticipate the need for general surgery consultation or surgical reconstruction with mesh.4,8 Low-cost alternatives to MRI, such as US, can also be used with up to 92% sensitivity for identifying RME. 7 The use of US to guide the feasibility of laparoscopic removal of RME is unknown, as this is the first case series describing this approach.
All but 1 of the patients in the current study had histories of at least 1 prior cesarean section, which is a known risk factor for AWE and RME.1,2,4 Of the 138 cases of RME reported in the literature, only 6 had no prior surgery1,9–11 (Table 4). Interestingly, 5 (23%) patients in the current study previously had surgery for excision of AWE and had been referred due to recurrence in symptoms. One possible explanation for the high number of reoperations is that the rectus endometriosis was missed when the initial surgeons did not excise disease below the fascia. In cases when subfascial disease is suspected, beginning with a diagnostic laparoscopy can be helpful to evaluate the rectus muscle and possibly avoid an open procedure. Another explanation is that RME was not suspected if adequate preoperative imaging was not ordered. Preoperative imaging is crucial, and, in recurrent cases, large lesions, or if fascial and muscular involvement is suspected, the current authors perform preoperative MRI. 4 This helps optimize surgical planning and counseling.
Cases Reported of Rectus Muscle Endometriosis in the English Language
yr, year(s); mo., month(s); US, ultrasound; CS, cesarean section, CT, computed tomography; MRI, magnetic resonance imaging; TAH, total abdominal hysterectomy; N/A, not applicable.
In the current study, 71% of women who had laparoscopic evaluation of the pelvis had additional lesions of endometriosis excised at the time of surgery. This is higher than the reported rates in AWE case series, which range from 5% to 26%.4,12–14 Of the 10 cases with pelvic endometriosis excised during laparoscopy, 60% had bladder or ureteral endometriosis. Patients with RME may be at higher risk of having concurrent genitourinary endometriosis, given the anatomically close relationship of the bladder and rectus muscle after a cesarean section. A physical examination suggestive of other deep infiltrating endometriosis, such as nodules and/or tethering, is also an important part of the preoperative evaluation. In women with pelvic or abdominal pain and physical examination findings suggestive of pelvic endometriosis, the current authors recommend a laparoscopic evaluation of the pelvis, given the high rate of pelvic endometriosis present in this population. Findings of endometriosis, such as deep infiltrating endometriosis or genitourinary disease, on preoperative MRI can also guide surgeons toward a laparoscopic approach (Fig. 4). Given the high rate of genitourinary endometriosis, laparoscopic resection of RME should be performed by a surgeon who is an endometriosis specialist and comfortable with complex disease presentations.
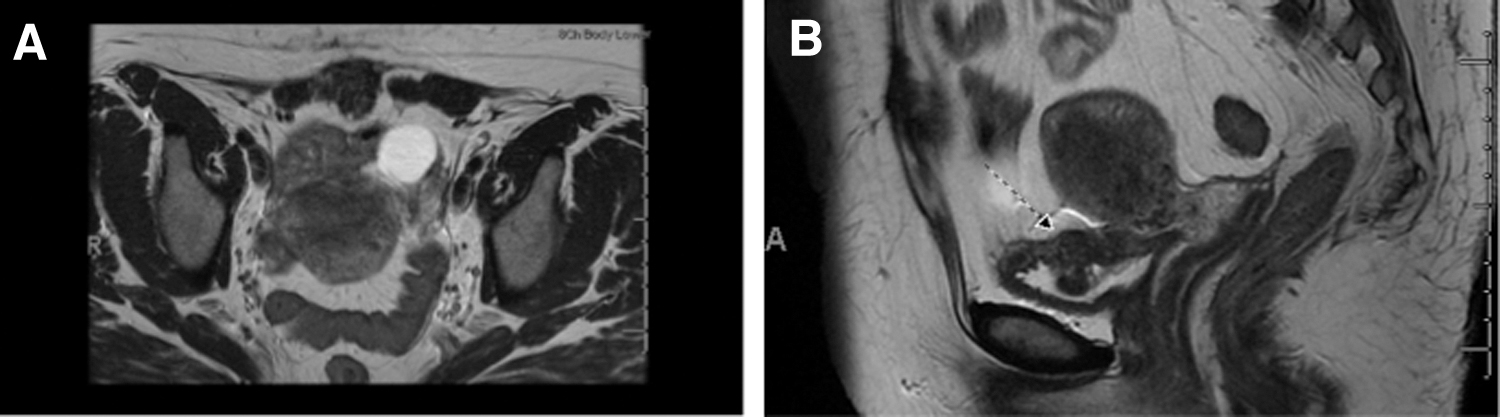
Magnetic resonance imaging of a case of rectus muscle endometriosis, requiring mesh repair, and concurrent bladder endometriosis (2 views).
One alternative to surgery is medical management. A mainstay of treatment is combined oral contraceptive pills (OCPs) or progestins provided continuously to suppress ovulation thereby creating a hypoestrogenic state. 15 OCPs are not ideal in all populations, particularly for women older than age 35 who are smokers or women at higher risk for cardiovascular events. In addition, women taking progestins can commonly experience breakthrough bleeding. 15 Second-line therapy includes gonadotropin-releasing hormone agonists, which are particularly helpful for deep infiltrating and extrapelvic endometriosis; however, these agents are not recommended for long-term use, given the risk of loss of bone density and menopausal symptoms. 15
Medical management in the current study population was attempted by 63.6% of patients who underwent laparoscopic excision and 18.2% of patients who underwent open excision. One hypothesis for the lower-than-expected use of conservative management is that the vast majority of patients had palpable nodules and/or focal tenderness. These patients often presented to their primary gynecologists who counseled the patients and then referred them to highly specialized surgeons with experience in the removal of RME. In cases of large lesions (> 3 cm) with a higher risk of mesh placement, a brief course of preoperative medical management to shrink the endometriotic lesion can be used.
Recurrence rates for symptomatic endometriosis without hormonal suppression can be as high as 50% at 5 years. 16 However, recurrence rates for symptomatic RME are not yet known. To limit recurrence, the current authors obtain a margin of normal tissue beyond the nodule to capture microscopic endometriosis. Patients are not placed on postoperative medical management, given the high level of certainty that all of the RME has been excised during surgery.
A strength of this study is that it was the largest case series looking exclusively at RME as a subtype of AWE. The clinical presentation of RME is subtly different than AWE with fewer patients with RME presenting with palpable masses.2,4,5 This study highlighted the variation in symptoms, workups, and treatment for RME uniquely, depending on where the bulk of the disease exists. Finally, this was the first study to recommend a laparoscopic approach to RME that enables access to the disease intraperitoneally, minimizes disruption to the fascia, and allows evaluation and treatment of pelvic endometriosis.
A limitation of this study was the nature of a retrospective case series. It was not possible to compare the groups of patients directly, given that RME is a rare disease with only 22 cases seen over 10 years at UPMC, making a comparative study difficult to power. The short-term (4 weeks) follow-up was another limitation, as no conclusions could be made on long-term symptom relief, recurrence patterns, or efficacy. The small population size and short-term follow-up does not allow evaluation of the risk of recurrence, pain levels, or satisfaction of women who had concomitant treatment of pelvic endometriosis, compared to those who did not, but future studies can explore this further.
In addition, the study did not characterize women with RME who were managed conservatively with medications. Another limitation was selection bias for highly skilled surgeons, which might prevent generalizability of the results or recommendations. The surgeons in this UPMC practice are comfortable with complex endometriosis resections, including laparoscopic mesh placement and genitourinary surgery. For suspected cases of RME, referral to an endometriosis surgeon is preferred. In facilities where this is not feasible, the current authors suggest a multidisciplinary approach with general surgery for the laparoscopic revision of the abdominal wall and with gynecology for excision of concurrent pelvic endometriosis.
Conclusions
This article described a minimally invasive approach to treating RME that may be a safe alternative to open, wide local excision. Even when excision is planned using an open approach, laparoscopic evaluation of the pelvis should be considered due to the high incidence of concurrent pelvic endometriosis.
Author Disclosure Statement
No financial conflicts exist.
Funding Information
The authors had no financial support for this study to disclose.