
Abstract
Background:
Corona virus disease-19 (COVID-19) pandemic emergency is of particular concern to oncologists in view of an often immunocompromised status of cancer patients along with the urgent need of cancer-directed treatment. Since the situation is unprecedented, deferring the oncologic procedures remains a dilemma. The importance to organize cancer care during the COVID-19 pandemic has become crucial. The goal of this study is to share experience in the management and surveillance of patients with gynecologic cancers during the global crisis.
Methodology:
This is a single-arm prospective observational study from February 1, 2020 till May 31, 2020. The study was performed at a tertiary care oncology institute in North India. All patients attending gynecologic oncology outpatient department (OPD) and in-patient department, both new and follow-up, were included. There was no control group for this study.
Results:
The number of gynecology oncology cases seen in OPD were 792. Among them new cases were (n = 168). Total number of surgery performed were (n = 120). Total number of patients who underwent COVID-19 real-time reverse transcription polymerase chain reaction testing were (n = 32). Five patients tested positive for COVID-19 during preoperative workup and the surgery deferred till a negative report. Postoperative course was uneventful.
Conclusion:
We share the best practices and measures taken at our institute for cancer treatment during the pandemic. With precautions, following standard guidelines, organizational support structure, and preparedness a similar good outcomes of surgery can be achieved balancing pandemic control with providing continued cancer care. Add (J GYNECOL SURG 37:222)
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV2), which originated from Wuhan, China, 1 has been declared pandemic by the World Health Organization (WHO) 2 on March 11, 2020.
The first case of COVID-19 in India was reported on January 30, 2020 and in Delhi on March 2. In India case fatality rate is low, at 1.9% against the global rate of 3.5% as of August 16, 2020. 3 The mortality rate for patients with cancer and COVID-19 coinfection is 7.6%. 4
In this ongoing pandemic elective surgical procedures were largely suspended in initial phase to prevent undue complications and to save the health resources for managing active COVID cases. Deferring the oncologic care remains a dilemma. 5 Comprehensive cancer care strategies and recommendations are being proposed and initiated by many oncology associations and societies.6–8
We share our experience in management of patients diagnosed with gynecologic cancers during the current pandemic of COVID-19.
Purpose of the Study
To study the management options, outcomes and care of the patients with gynecologic cancers during the pandemic. We hypothesize that with adequate precautions and adherence to national guidelines, outcome of patients undergoing elective gynecologic oncologic surgery with a negative COVID-19 reverse transcription polymerase chain reaction (RT-PCR) test will not be adversely affected.
Methodology
This is a single-arm prospective observational study from February 1, 2020 till May 31, 2020. The study was performed at a tertiary care oncology institute in North India. All patients attending gynecologic oncology outpatient department (OPD) and in-patient department (IPD), both new and follow-up, were included. There was no control group for this study. We have compared our data with previous year data during the same time period. This, however, is not a true control.
COVID-19 measures taken at our center are explained in Table 1.
COVID-Directed Measures Taken at Our Center
MoHWF, Ministry of Health and Family Welfare; OPD, outpatient department; PPE, personal protective equipment; rRT-PCR, real-time reverse transcription-polymerase chain reaction; WHO, World Health Organization.
All patients were counselled preoperatively about the risks and benefits of surgery, their vulnerability to coronavirus infection, the augmented probability of intensive care unit admission and mechanical ventilation if they deteriorate, and in due course poorer outcomes. Total 32 patients underwent COVID-19 RT-PCR testing as per the institutional testing protocol with effect from April 14, 2020. Patients operated before April 14, 2020 were not tested for COVID-19 since no such protocol was available at the institution. As per national guidelines and institutional policy, surgery for patients who were positive was deferred except in emergency situations when such procedures were performed wearing full personal protective equipment. COVID-19 positive patients were retested after 14 days as per prevailing guidelines at that time.
Results
Between February 1, 2020 and May 31, 2020, 37,911 (3413 new patients and 27,720 follow-up patients) visited our center. Seven hundred ninety-two patients (168 new patients and 624 follow-up patients) were seen in gynecology oncology OPD. This excludes the gynecology oncology patients visiting radiation and medical oncology OPD during the study period.
Among follow-up cases (n = 624), cancer of ovary was seen in 281, endometrium in 143, cervix in 79, vulva in 11, and vagina in 12. Thirty-two patients had benign gynecologic lesions, 8 had premalignant lesions. Nongynecologic malignancy follow-ups were 58 in number. Among new patients (n = 168) of cancer, 81 were endometrium, 45 ovary, 12 cervix, 1 vulva, 3 vagina, and 17 were other nongynecologic malignancies. Also six patients of benign gynecologic lesions and three of premalignant lesions were seen (Fig. 1).
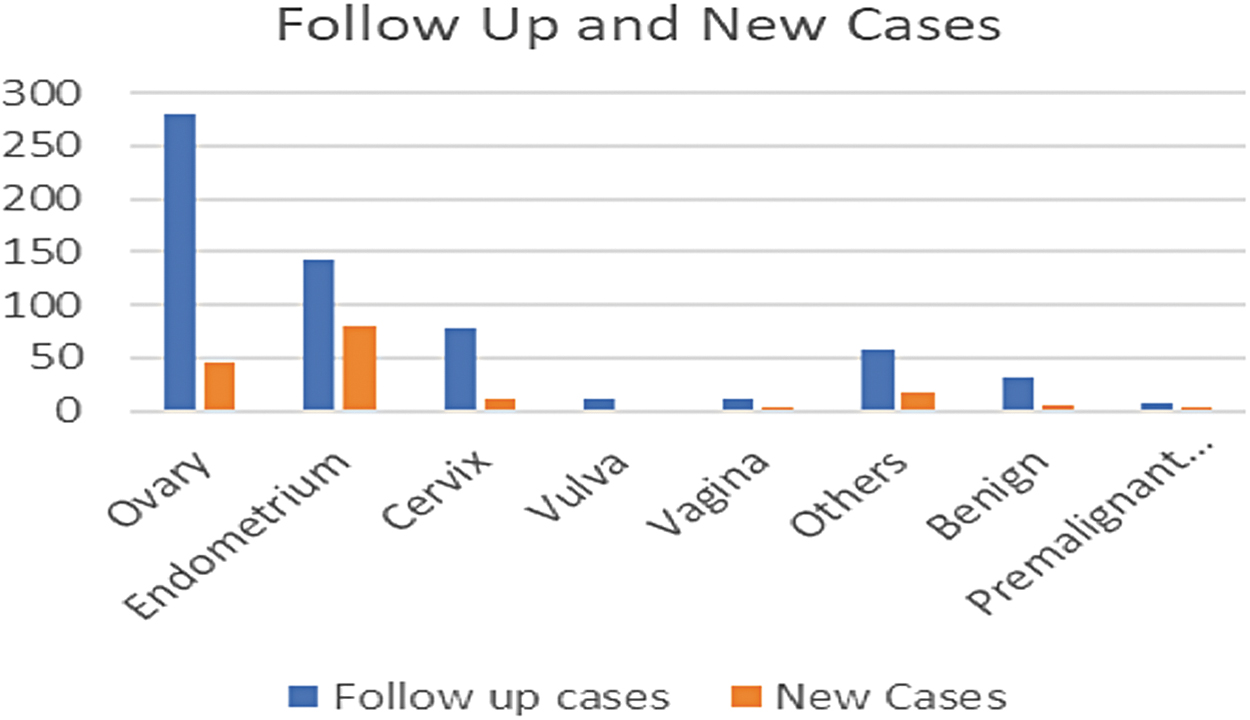
Gynecologic oncology cases (follow-up cases/new cases) visited RGCIRC from February 1, 2020 to May 31, 2020 during COVID-19 times. RGCIRC, Rajiv Gandhi Cancer Institute & Research Centre.
One hundred twenty patients were operated. Five patients tested positive for COVID-19 during preoperative workup and surgery was performed once they tested negative.
Sixty-five surgeries were done for ovarian cancer of which 15 were primary cytoreductive surgery (CRS), 29 interval debulking surgery (IDS), 11 patients IDS with hyperthermic intraperitoneal chemotherapy (HIPEC), and 10 secondary CRS. Eighteen patients underwent diagnostic hysteroscopy with dilatation and curettage for postmenopausal bleeding, dysfunctional uterine bleeding, or increased endometrial thickness in a follow-up of hormone positive carcinoma breast. Twenty-one patients underwent radical hysterectomy (nine robotic radical hysterectomy [eight cancer endometrial carcinoma]). Two radical vulvectomy with bilateral inguinofemoral lymphadenectomy and one partial vaginectomy were performed. Thirteen patients underwent surgery for adnexal mass, which proved benign on frozen section with final histopathology report suggesting endometriosis, mucinous cystadenoma, and so on (Fig. 2).
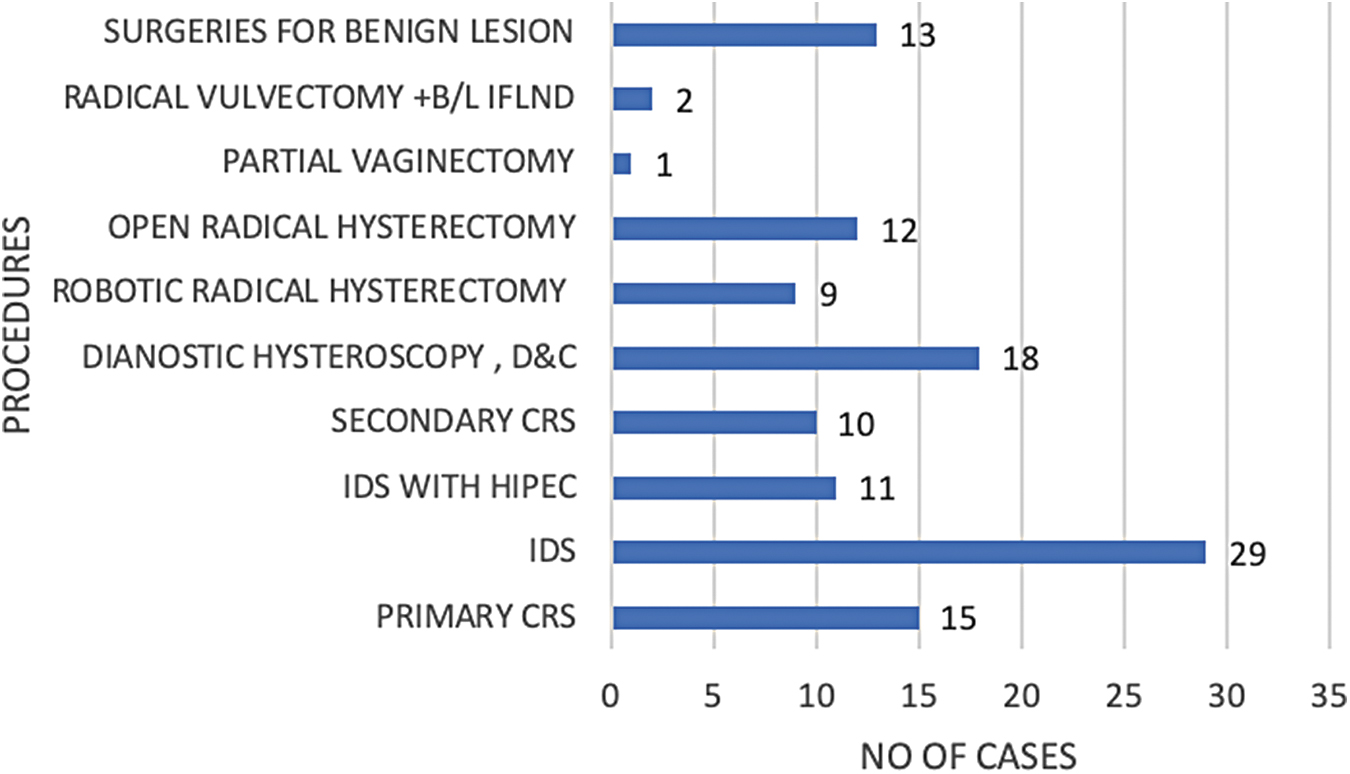
Gynecologic oncology cases operated at RGCIRC from February 1, 2020 to May 31, 2020 during COVID-19 times.
Immediate postoperative course was uneventful. Mean hospitalization stay duration was 5 days. Also postoperative outcome was measured in terms of lung infections or complications of chest infections hence during the hospital stay, and wound complications such as increased wound infections, dehiscence, or need of resuturing. Delayed postoperative recovery in terms of increased hospital stay was also the same observed as compared with similar times last year.
There was no incidence of wound infection postoperatively. None of the aforementioned morbidity was recorded during 2 weeks follow-up in our study population. Two patients who initially tested COVID-19 positive underwent planned surgery outside the study period (after a negative report) with no increase in postoperative morbidity. Surgery in these patients was performed 1 week after a repeat COVID-19 negative report was available.
There was no mortality among the gynecologic cancer patients treated during the study period as compared with previous times.
In preceding year during same time period, 204 surgeries were performed (major 160 and minor 44). There were 47 robotic radical hysterectomies performed (33 cancer endometrium and 14 cancer cervix) and 17 open radical hysterectomies were performed (7 cancer endometrium and 10 cancer cervix). For cancer ovary a total of 59 surgery were performed, including primary, interval, and secondary CRS with HIPEC as indicated.
Twenty-three exploratory laparotomy frozen proceed for adnexal mass or pelvic mass were done and 12 surgeries for other conditions (benign, palliative, and prophylactic).
During this pandemic, an impact on health care workers was also assessed. Fifty-six out of symptomatic 189 health care staff tested positive for COVID-19 RT-PCR during the study period. Out of total 2150 hospital employees, 1546 are the direct patient contact health care workers, including the doctors, nursing staff, technicians, and ancillary patient care workers at the institute. Probably the timely enforcement of guidelines aided in this low incidence (3%) of infection in medical and paramedical health care staff at our institute.
Discussion
There is a lack of data regarding outcome of gynecologic oncology patients during this ongoing pandemic. In India, as of August 16, 2020, there were a total of ∼25,94,612 confirmed cases with 50,126 mortalities. Patients undergoing active cancer treatment have been reported to be more susceptible to serious morbidities related to COVID-19. 5 Liang et al. 10 and the Chinese Centre for Disease Control and Prevention in their analysis reported significant mortality associated with COVID-19 in older patients and in patients with other medical comorbidities. 11
In comparison, in the previous year prepandemic period, between October 1, 2019 to January 30, 2020, the total number (n = 1521) of patients were seen in the OPD and the number of surgical procedures (n = 166) were performed. It was found that the total number of gynecologic oncology cases visiting OPD were 52.07% (n = 792) and gyneco-oncologic surgical procedures performed at hospital were 72.28% (n = 120) in the study period as compared with prepandemic declaration, respectively. This reduction in patients was attributable to a nationwide lockdown, lack of transport facilities, and widespread fear among patients and relatives against visiting hospital.
A delay in definitive cancer therapy is associated with risk of tumor progression and the potential loss of curative window that needs to be weighed against a probable risk of infection with COVID-19.
Zhang et al. 12 concluded that patients with gynecologic cancers are susceptible to morbidity that may be associated with COVID-19 infection. In our cohort, two patients were rescheduled for surgery outside the study period who initially tested positive for COVID-19. Surgery was performed 1 week after COVID-19 negative report as per our guidelines and as corroborated by various other cancer society guidelines.13–15 No additional postoperative morbidities were reported in these patients.
We found that out of total patients planned for surgery only five patients tested positive for COVID-19. In all patients who underwent elective surgery immediate postoperative period was uneventful. Patients were followed up to 2 weeks postoperative period with no wound infection, and a mean hospitalization duration of 5 days.
A reduction in number of patients able to reach hospital facility timely and hence an overall reduction in number of surgery or definitive treatment as seen in our study suggests that with the ongoing pandemic, it is likely that there will be delayed presentations to hospital, which may upstage the disease and increase the burden of inoperable cases. A teleconsultation approach can be useful to reassure and advice follow-up of patients. Outpatients scheduled for treatment should come with no or one attendant. Triage of patients with fever and/or respiratory symptoms is vital to prevent contact and exposure to other patients and health care providers.
Universal COVID screening was only applicable for past 6 weeks of the total 20 weeks that were studied. Therefore, number of COVID positive patients is not an accurate representation.
There was no mortality among our study group, hence the study could not be compared with the COVID-19-affected gynecology cancer patients. Long-term follow-up of these patients are yet to be determined for susceptibility and outcomes of COVID-19.
Conclusion
We share the best practices and measures taken at our institute for cancer treatment during the pandemic. With precautions, following standard guidelines, organizational support structure, and preparedness a similar good outcomes of surgery can be achieved balancing pandemic control with providing continued cancer care.
Footnotes
Authors' Contributions
R.S. was in charge of conceptualization, supervision, editing, and reviewed the article. A.N. designed, collected, compiled, reviewed, and edited the article. P.R. analyzed data and scripted the article. P.M. collected and compiled the data.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.