
Abstract
Background:
Uterine perforation is one of the most-serious complications after a surgical abortion, and the risk of such perforation is increased in second-trimester procedures. When a uterine perforation occurs, products of conception (PoC) can migrate through the uterine defect to the abdominal cavity requiring surgery for their extraction.
Case:
In a 17-year-old patient, intra-abdominal fetal remains were caused by multiple uterine perforations following a dilation and evacuation procedure for a surgical abortion at 19 weeks' gestation. An emergency laparotomy was required to control this patient's bleeding, repair the uterine perforations, and extract the fetal remains. Fetal reconstruction from extracted fragments was incomplete, and, despite performing an extensive review of the abdominal cavity and an intraoperative radiography that did not identify fetal structures, a postoperative computed tomography scan showed fetal remains in the left parietocolic region. A diagnostic laparoscopy was performed for their extraction during the same hospitalization.
Results:
After the extraction, the patient recovered well.
Conclusions:
Intra-abdominal retained PoC must be considered after a surgical abortion complicated with uterine perforation, especially if fetal reconstruction of the extracted fragments is incomplete and no intrauterine fetal remains are identified by ultrasound. (J GYNECOL SURG 37:263)
Introduction
It is estimated that 56 million induced abortions occur each year worldwide, and that 10%–15% of them are performed in the second trimester of pregnancy.1,2 Uterine evacuation in the second trimester can be accomplished by medical induction of labor or by a surgical procedure, which is dilation and evacuation (D&E). 3 D&E involves preoperative dilation of the cervix with osmotic dilators; administration of prostaglandins or a combination of both; and an operative evacuation of the uterus with suction, extraction forceps, and/or curettage. Although surgical abortion in the second trimester is a safe procedure, it is associated with a higher rate of complications, compared with abortions performed in the first trimester of pregnancy.4,5
Uterine perforation is an uncommon, but potentially serious, complication of surgical abortion and occurs in fewer than 1% of second-trimester D&E procedures.6–8
The risk of uterine perforation is increased by factors that make access to the endometrial cavity difficult (e.g., cervical stenosis or inadequate cervical preparation) or alter the strength of the myometrial wall (e.g., increasing gestational age, multiparity, or a previous uterine scar). 6 The failure to use ultrasound (US) guidance during the procedure, poor expertise of the physician performing the procedure, inadequate anesthesia, and use of grasping instruments and curettage instead of aspiration will also increase that risk.5,6
Uterine perforation may be associated with injury to surrounding blood vessels or viscera (bladder or bowel), and can result in hemorrhage or sepsis.6,8 When a uterine perforation occurs, products of conception (PoC) can migrate to the abdominal cavity through the uterine defect, requiring abdominal surgery for their extraction. 6 This article reports a rare case of intra-abdominal fetal remains caused by multiple uterine perforations following a D&E for a surgical abortion at 19 weeks' gestation.
Case
A 17-year old female was referred from a private medical center to its reference tertiary-care hospital because of persistent hypotension following a dilatation and evacuation (D&E) procedure for an induced legal abortion at 19 weeks' gestation. No information was given regarding fetal parts that had already been extracted or the instruments used for the uterine evacuation. On arrival at the emergency department, this patient presented with hypotension and tachycardia, and a US scan showed evidence of intra-abdominal free fluid. After stabilizing the patient with fluids, a computed tomography angiography (CTA) was performed for evaluation of the possibility of uterine embolization. The CTA confirmed the presence of a hemoperitoneum and multiple uterine perforations that were actively bleeding, but no clear bleeding vessel was identified. In addition, a heterogeneous object—suggestive of fetal remains—was observed adjacent to the uterine wall.
Given that there was profound bleeding and that surgery was required for extraction of the possible fetal remains, the patient underwent an emergency laparotomy with a subumbilical midline incision that confirmed the presence of blood in the abdominal cavity, multiple uterine perforations on the anterior and posterior uterine walls, a laceration of the right fallopian tube, and a perforation of the sigmoid colon (Fig. 1). Following drainage of 2 L of blood, fetal remains that were identified during surgery were extracted from the abdominal cavity and the integrity of bladder was ensured by methylene-blue instillation through a urinary catheter. The uterine and sigmoid-colon perforations were sutured and a right salpingectomy was performed.

Macroscopic view of the initial surgery. Multiple uterine perforations were visible on the anterior uterine wall.
After ensuring that there were no other bleeding sites, an intraoperative radiography was requested to ensure there were no fetal remains left in the abdominal cavity. This was requested because no information was available regarding the totality of extracted fetal fragments in the hospital of origin and the fetal reconstruction out of the extracted fragments in the current center was incomplete. The abdominal radiography was normal, and did not show any bony fetal structures in the abdominal cavity. A BLAKE® drain was inserted intra-abdominally, and the abdominal wall was closed in layers. Next, a vaginal examination was performed, showing a small laceration on the right vaginal wall that did not require suturing. There was no evidence of fetal remains in the vagina or the endocervix, and a postoperative vaginal echography showed an empty uterine cavity. A total of 6 units of red blood cells and 1 unit of plasma were transfused during the operation and the immediate postoperative period. Prophylactic antibiotic treatment with meropenem was also started. The patient remained stable during the postoperative period with the exception of a single temperature spike on day 3. Blood tests and cultures showed no evidence of infection, and the BLAKE drain was removed on day 5.
On day 8, when the patient had achieved a correct postoperative recovery, a computed tomography (CT) scan was requested to ensure that no intra-abdominal fetal remains had been missed during the surgery and on the intraoperative radiography. The CT scan showed a heterogeneous object measuring 50 × 35 mm in the left parietocolic region, at the level of L-4–L-5, suggestive of fetal remains (Fig. 2). As the patient was stable and did not require urgent surgery, laparoscopic surgery was planned for extraction of these fetal remains and was programmed into the next available surgical slot. On day 12, the laparoscopy was performed and confirmed the presence of the additional fetal remains in the abdominal cavity, which corresponded to fragments of a spinal column and a lower extremity. Blunt dissection and cold cut were used to separate the fetal remains from the surrounding tissue. After ensuring hemostasis, these fetal remains were extracted in a bag through a 12-mm portside placed in the right iliac fossa.
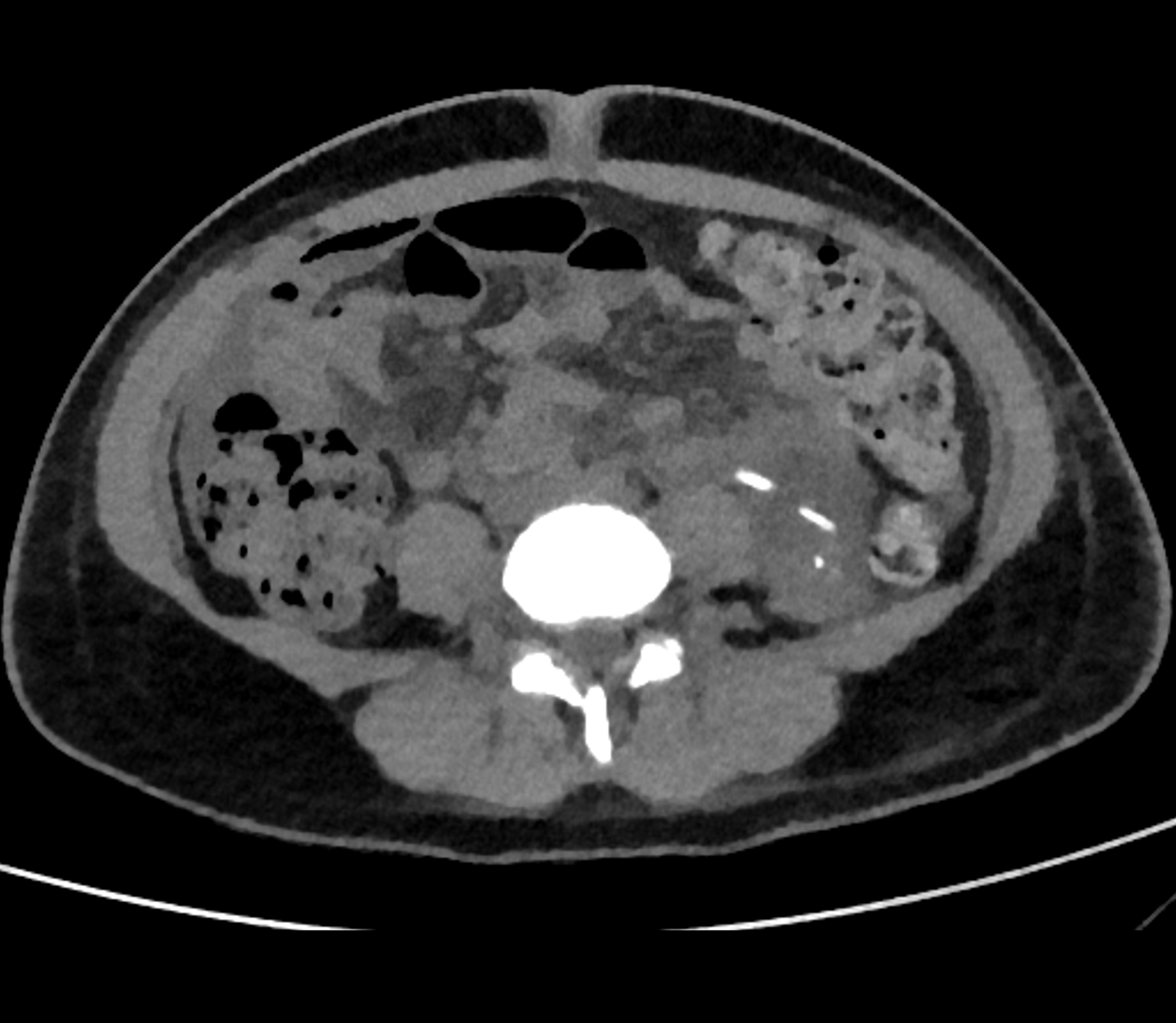
A computed tomography was scan performed on day 8 after the first surgery, showing abdominal fetal remains in the left parietocolic region.
Results
After this laparoscopy, the patient made a good recovery, and was discharged 3 days later.
Informed consent
Written informed consent was obtained from the patient and her mother for the publication of the present case report.
Data availability statement
Data are provided within the article or its Supplementary video (the Supplementary video is available online at www.liebertonline.com/gyn). Figure 3 is a still image from this video.

Still image from Supplementary video (available online at www.liebertonline.com/gyn). Laparoscopic surgery was performed on day 12 for the extraction of abdominal retained products of conception.
Discussion
D&E is the surgical procedure of choice for second-trimester abortions, and one of D&E's most-serious complications is uterine perforation. Uterine perforation occurs in <1% of D&E procedures, and usually affects the anterior or posterior uterine walls.6–9 Perforation at the midline typically leads to minimal bleeding, whereas a lateral uterine perforation may lacerate uterine blood vessels, resulting in immediate and profuse hemorrhage or even a broad-ligament hematoma. 10 When a uterine perforation occurs, surrounding viscera can be injured and also incarcerated in the uterine defect. 11 The migration of PoC into the abdominal cavity through a uterine perforation is an extremely rare complication of surgical termination of pregnancy that has been previously reported in the literature.12,13
After a D&E procedure, fetal reconstruction from the extracted fragments is advisable to ensure that all PoC have been extracted. 14 A gestational sac must be identified in <9 weeks' gestation, while fetal parts may begin to be identified in gestations between 9 and 10weeks. After 12 weeks, the skull, spine, 4 extremities, gestational sac, and placenta must all be identified. When a complete extraction of the PoC cannot be ensured and intrauterine fetal remains are not visible on US, a uterine perforation and the possibility of abdominal fetal remains migration must be suspected, and evaluated using by abdominal US or CT scanning. 14
A uterine perforation that is not complicated by bleeding or injury to surrounding structures can be managed conservatively if there is no concern about potential retained PoC. 10 However, when intra-abdominal bleeding or injury is suspected, or when it is not possible to ensure that all PoC have been extracted, surgical inspection of the abdominal cavity must be performed. 15 During surgery, an exhaustive revision of all abdominal organs and structures is essential in order to detect inadvertent lesions, and retained PoC in the abdominal cavity must be excluded. Surgical evaluation of intra-abdominal retained PoC may be challenging, as fetal fragments are usually small and can be located in any abdominal area. The value of an intraoperative radiography may be limited by its image quality, due to the reduced radiation energy used to minimize medical-staff exposure, compared to conventional radiography. In addition, the patient's supine position; the absence of a lateral view; and artifacts related to the presence of surgical drapes, catheters, and surgical instruments in the radiation field can impair optimal interpretation of the imaging test.
Given the difficulty in evaluating the presence of fetal remains during laparotomy, as exemplified in this case, it is essential that good communication exists between the referring clinician and the tertiary-hospital team regarding all the details of the D&E procedure, including the fetal remains that were extracted.
Conclusions
After a D&E procedure, a reconstruction of the extracted fetal remains must be performed to rule out retained PoC. When complete extraction of the PoC cannot be ensured and intrauterine fetal remains are not visible on transvaginal US, a uterine perforation must be suspected, and the migration of fetal remains into the abdominal cavity should be assessed using abdominal US or CT scanning.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
The authors received no financial support for the research or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.