
Abstract
Objective:
Average operative blood loss in abdominal hysterectomy—the most common gynecologic surgery—ranges 300–400 mL. This may not be much in normal women, but women with preexisting anemia may require blood products pre- or postoperatively or have poor healing and more surgical-site infections. Minimizing blood loss in abdominal hysterectomy for leiomyomatosis uteri has been studied with limited success of gonadotropin-releasing hormone analogues and misoprostol. This study assessed the effectiveness of a single vaginal preoperative dose of misoprostol prior to open abdominal hysterectomy for reducing blood loss and drop of postoperative hemoglobin, compared to routine hysterectomy without misoprostol.
Materials and Methods:
This was a randomized, parallel-group, placebo-controlled interventional-drug trial with double-blinding. Each of 2 groups had 35 participants. Women randomized to group A received 2 200-μm tablets of misoprostol vaginally 30 minutes before the start of the operation. Women randomized to group B received 2 placebo tablets.
Results:
Both groups had comparable mean ages, body mass indices (BMIs), uterine sizes, symptoms, and medical comorbidities. The mean uterine weight in both groups was >365–391g and mean operating times (111–119 minutes) were similar in both groups. Operative blood loss was 394 ± 186 mL in the misoprostol group and 455 ± 288 mL in the placebo group, which was not significant. (p = 0.228). A difference of 61.5 mL (difference of 13%) occurred between the groups, but did not significantly affect postoperative requirements for blood products, postoperative complications, or hospital stays, which were not statistically different in the groups.
Conclusions:
Using a single vaginal misoprostol dose prior to total abdominal hysterectomy for large-size uteri (>12 cm) does not significantly reduce the intraoperative blood loss, drop in hemoglobin, nor need for postoperative blood transfusion.
Introduction
Abdominal hysterectomy is the most commonly performed gynecologic operative procedure around the globe for many uterine pathologies. Estimated average blood loss during hysterectomy is variable but, in uncomplicated open abdominal hysterectomy, the estimated blood loss (EBL) is 300–400 mL with 2% of patients having excessive bleeding. 1 Minimizing blood loss in abdominal hysterectomy is important—more so in developing countries where almost half (53.1%) of the women have preexisting anemia. 2
Reduced operative blood loss translates into lower requirements for blood products, reduced surgical-site infections (SSIs), better healing, timely recovery, and less need for hematinics for the patient. Preoperative build-up of hemoglobin, use of drugs such as gonadotropin-releasing hormone (GnRH) agonists and mifepristone can affect operative blood loss significantly. Meticulous surgical technique with tourniquets and uterine or internal iliac ligation; or use of intraoperative vasopressin, epinephrine, oxytocin, or misoprostol have been studied for reducing blood loss during hysterectomies. Misoprostol has a vasoconstrictive effect on the uterus and might be a less-expensive alternative, especially in low-resource settings.
Most studies assessing methods to reduce blood loss have included myomatous uteri, but from surgical experience, it is known that even bulky uteri (> 10 weeks) can cause significant operative blood loss due to retained blood in specimens apart from the average blood loss associated with the procedure. The current study assessed the effectiveness of using a single preoperative dose of misoprostol by a vaginal route prior to open abdominal hysterectomy for reducing blood loss and drop of postoperative hemoglobin, compared to routine hysterectomy without misoprostol.
Materials and Methods
This study was conducted in the department of obstetrics and gynecology, in a tertiary-level hospital in eastern India from July 2016 to December 2017 after obtaining approval from the institutional ethics committee of All India Institute of Medical Sciences (AIIMS)—Patna, in Patna, Bihar, India (institutional ethics committee ref no.: AIIMS/Pat/IEC 64/2016). The trial was registered with the Clinical Trials Registry–India (CTRI) registration no.: CTRI/2017/08/009494; registered on: August 25, 2017).
This was an interventional drug trial designed as a randomized, parallel-group, placebo-controlled trial with double-blinding. The participants, investigator, outcome assessor, and data-entry operator were blinded to the 2 groups in the study. Randomization was performed by using the random sequence method of computer-generated randomization and concealment was achieved by placing sequentially numbered, sealed opaque envelopes with the serial numbers; the envelopes were opened on day of surgery for the patients.
The average blood loss during hysterectomy of larger uteri as considered to be 450ml ±150 mL. The sample size was calculated to identify the difference of intraoperative blood loss of 100 mL between the 2 groups to affect clinical outcomes. Taking the power of study 0.8 and significance level of p-value of 0.05, the sample size was calculated as 70, with 35 patients in each group.
The study population included females, 35–55 years of age, who were symptomatic for, and undergoing, total abdominal hysterectomy (TAH) for benign gynecologic condition, such as symptomatic fibroid uteri, adenomyosis, or abnormal uterine bleeding (AUB) not responding to medical management; or having uteri sizes >10 cm.
Exclusion criteria were: hysterectomy for malignancy; contraindications to misoprostol (mitral stenosis, glaucoma, sickle-cell anemia, diastolic blood pressure >100 mm Hg, severe asthma; or known allergy to prostaglandin); conditions with dense pelvic adhesions and excessive bleeding, such as endometriosis or associated pelvic inflammatory disease; active medical disease; history of myomectomy; preoperative mifepristone or GnRH analogue treatment; or mental impairment or inability to give consent.
Women fulfilling the inclusion criteria, were recruited during their visits to the preoperative assessment clinic, usually 1–2 weeks before surgery. There were 80 eligible patients. Each patients was provided with verbal and written information and informed consent was obtained. After routine preoperative care, a standard technique was used to perform open abdominal hysterectomy. Prior to taking the patient, group allocation to experimental or control was made in in the preoperative area and the drug or a placebo was administered vaginally 30 minutes prior to the first incision. Women in group A received a 2 200-μg tablets of misoprostol vaginally 30 minutes before the start of the operations. Each woman in group B received 2 tablets of a placebo (similar-size white calcium-carbonate tablets). All women were given prophylactic antibiotics and thromboprophylaxis according to hospital protocols.
Operative blood loss was measured by weighing of soaked mops and gauze pieces and the amount of blood collected in the suction device. All patient data details were maintained on Excel® spreadsheets, per the data collected and entered in the predesigned proforma. Statistical analysis was performed on Statistica, version 6 (StatSoft Inc., Tulsa, OK, 2001) software.
On initial assessment 80 patients were eligible for the study, but 4 underwent laparoscopic hysterectomy, 3 did not give consent, and 1 patient who had a suspected cervical malignancy had her operation converted to a radical hysterectomy. These 8 patients were excluded. The remaining 72 patients were randomized to 2 groups of 36 patients in each group. In group A, 3 patients were excluded intraoperatively due to anesthetic and surgical complications. Thus, the final analysis included 33 patients in group A (misoprostol) and 36 patients in group B (placebo). Figure 1 shows the eligibility flow.
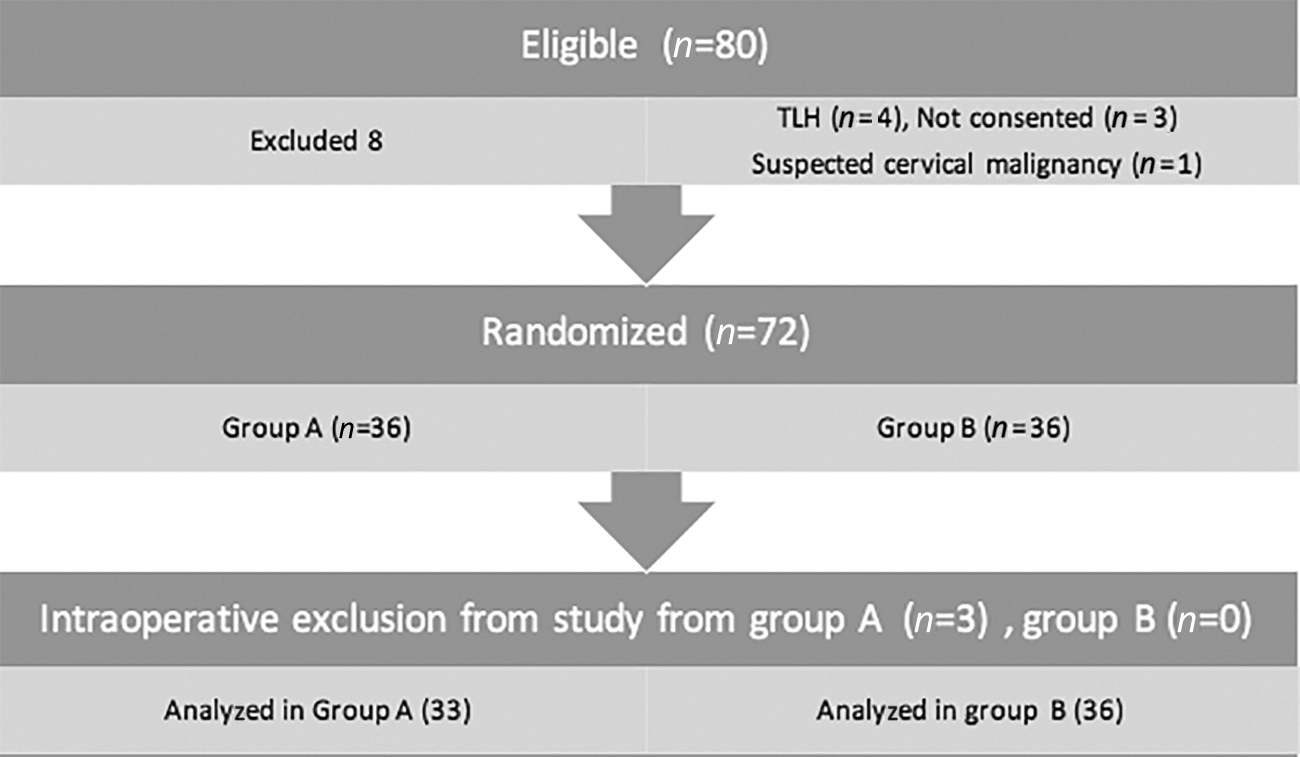
CONSORT flow diagram for this trial. TLH, total laparoscopic hysterectomy.
Variables were normally distributed according to a Kolmogorov–Smirnoff goodness-of-fit test except for variables of uterine size, uterine weight, number of blood units required, operating time,, and hospital stay.
Results
The mean age of patients enrolled was similar (42) in both groups. Their body mass indices (p = 0.432), clinical uterine sizes (p = 0.290), and sonographic uterine measurements (p = 0.104) were also was comparable between the 2 groups. Most patients presented with heavy menstrual bleeding (64% in group A and 54 % in group B); other symptoms were irregularity in menses (12% in group A and 3% in group B), heaviness in the lower abdomen, painful menstrual cycles (21% group A and 42 % group B), and postmenopausal bleeding in 1 patient in each group. With respect to comorbidities, 24% in group and 16.7% in group B had conditions such as hypertension, hypothyroidism, or diabetes mellitus. Indications for hysterectomy were still related to leiomyoma in most cases (68%–69%) in both groups (Table 1).
Preoperative Variables in the 2 Groups
* Student's unpaired t-test.
Mann–Whitney-U test.
χ 2 test.
yrs, years; BMI, body mass index; wks, weeks; USG, ultrasonography; HMB, heavy menstrual bleeding; PMB, postmenopausal bleeding; HTN, hypertension; DM, diabetes mellitus; AUB, abnormal uterine bleeding; L, leiomyoma; P, polyp; A, adenomyosis.
When comparing the operative details in both groups, it was noted that there was no significant difference if general or regional anesthesia was used (p = 0.06), or whether the operation was performed by a consultant or resident (p = 0.61), or whether the incision was Pfannenstiel or longitudinal (p = 1.00 ). The uterine weights in both groups was comparable (361 g in group A and 392 g in group B) as was the operative duration (119 minutes in group A and 111 minutes in group B; p = 0.65).
The operative blood loss was 394 ± 186 mL in the misoprostol group (A) whereas it was 455 ± 288 mL in the placebo group (B), which was not significant (p = 0.228), but a difference of 60 mL was noted between the groups, although all other variables were comparable and similar in both groups (Table 2).
Comparison of Operative Details Between the 2 Groups
* χ 2 test.
Mann–Whitney-U test.
Student's unpaired t–test.
Fisher's exact test.
GA, general anesthesia.
Postoperative hemoglobin levels (group A: 9.48 ± 1.37; group B: 9.69 ± 1.27) were similar in both groups and the hemoglobin difference (group A: 1.92 ± 0.92; group B: 1.87 ± 0.86) was not significant (p = 0.32). See Table 3. The length of hospital stay (p = 0.39), febrile episodes (p = 0.94), and SSIs (p = 1.0) were comparable in both groups. In group B, 6/36 patients received injectable iron, while in group A, 5/33 received injectable iron. In group A, 3 patients were given 2 units each of transfused blood, whereas, in group B, 4 patients each received 2 units, and 1 patient received a single unit. These were also nonsignificant differences in both groups (p = 0.5, p = 0.47).
Postoperative Outcomes Compared Between the 2 Groups
* Student's unpaired t-test.
Mann–Whitney-U test.
Fisher's exact test.
χ 2 test.
Hb, hemoglobin; d, days; SSI, surgical site infection.
Discussion
Large-sized uteri, even nonpathologic enlargements, can accumulate a greater amount of concealed blood in the uterine body. Removal of a large uterus is associated with concealed blood loss, in addition to the blood loss associated and expected during hysterectomy procedure. Clinical assessment of postoperative hematocrit status generally depends on the estimated operative blood loss that is visible in a suction device, mops, and gauze pieces.
A large leiomyomatous uterus (typically defined as ≥16 weeks' size or 350 g) is known to limit the choice of skin incision in an open hysterectomy and to result in increased intraoperative blood loss3,4 The current study included bulky uteri as seen on ultrasound (> 10-cm lengths) and a had a mean uterine weight of >350 g in both groups.
Preexisting anemia has been linked to increased likelihood of blood transfusion and risk of perioperative morbidity and mortality. In a systematic review of 20 observational studies, preoperative anemia was most strongly associated with a higher risk of receiving a blood transfusion. 5 In this current study, preoperative mean hemoglobin was 11.2 g/dL in group A and 11.3 g/dL in group B, showing that anemia was prevalent. Preoperative build-up of hemoglobin by blood transfusion was performed in 3 women in group A (7 units) and in 4 women in group B (8 units).
The average estimated intraoperative blood loss in abdominal hysterectomies is 300–400 mL, 6 and excessive bleeding complicates ∼2% cases.1,7 In a systematic review of randomized trials reported in 2012 by Lethaby et al., 8 blood loss was found to be only slightly less (85 mL) in subtotal, compared with, total hysterectomy. The risk of requirement of blood transfusion was not different in both groups. 8 A sensitivity analysis was performed by English et al. in 18,033 hysterectomies for benign indications from 61 hospitals to establish the associations of transfusion, readmission, reoperation, length of stay, and postoperative complications with estimated blood loss (EBL). In that study, the median EBL was 100 mL, while 400 mL was in the 90th percentile—the threshold for significantly increased risk of transfusion, readmission, reoperation, longer length of stay, and major postoperative complications. 9
The present study, compared to English et al.'s 9 study, had higher median blood losses in both groups (394 mL in the misoprostol group and 455 mL in the placebo group). This compared with many studies, such as Lethaby et al. 8 and Thakar et al., 6 but did not match with the median EBL of the English et al. 9 study reporting it to be as low as 100 mL. That study found risk factors for EBL >400 mL were cases in which laparoscopic hysterectomy was performed, when surgery lasted more than 3 hours, or uterine sample weight was >250 g. Adhesive disease, low surgeon volume, being younger than 40 years of age, having a BMI >35, and the need for a preoperative transfusion were also statistically significantly associated with EBL >400 mL.
The present study, however, did not find any significant difference in blood loss whether the surgeon was a consultant or resident, or related to uterine weights, uterine size, types of anesthesia, types of incisions, weights of patient, or their diagnoses.
Various methods have been tried to reduce operative blood loss during TAH. A course of GnRH analogues 2–3 months prior to the planned hysterectomy, to shrink the size of fibroid(s) and reduce their vascularity, is the most-common approach. Although GnRH analogues are effective for reducing uterine volume and intraoperative blood loss, the significant hypoestrogenic side-effects and high costs of these agents are limiting factors for most patients. 10 Intramyometrial vasopressin injection also been used for hysterectomies for large leiomyomatous uteri with significantly lower mean total blood losses, but serious complications—such as bradycardia, cardiac arrest, and pulmonary edema—have been reported requiring intensive care units that are not available in many hysterectomy settings for operating on low-risk cases. 11
Obstetrics practice has transformed much after use of misoprostol, a prostaglandin E1 analogue, especially for postpartum hemorrhage and for miscarriages. Stimulation of uterine contractions, increased myometrial contractility, and constriction of feeder vessels of fibroids, along with increased the uterine artery resistance and reduced blood flow are the possible mechanisms for reducing blood loss during myomectomy and hysterectomy.12,13 Direct vasoconstrictor action of uterine artery has also been proposed. 14
Use of misoprostol just prior to myomectomy is widely practiced because of this agent's ease of use, minor or no side-effects, and significant reduction in EBL, and lower fall in postoperative hematocrit independent of the surgical technique applied.15,16 This agent also reduces need for postsurgical blood transfusions. Its use and availability is important in lower-resource countries, due to long shelf-life and lower costs.
In a randomized trial, reported by Biswas et al., a single preoperative dose of misoprostol produced a significant reduction of hysterectomy blood loss, higher postoperative hemoglobin levels, and less reduction of hemoglobin in the misoprostol arm of the trial. 17 However, an earlier pilot study on sublingual misoprostol reported its non-effectiveness for reducing blood loss or need for blood transfusions. 18 Yet, that trial did report a difference of blood loss of 8%. This present study with vaginal misoprostol did not produce a significant difference in blood loss in the 2 groups, but a 13% (61.5 mL) lower blood loss was recorded in the misoprostol arm of this current trial. The hemoglobin difference between preoperative and postoperative values was also not significant.
Another randomized controlled trial by Panichpongpan et al. included 70 women who received 400 μg of sublingual misoprostol preoperatively. The agent was ineffective for reducing blood loss or need for postoperative blood transfusions in patients undergoing abdominal hysterectomies. 19 All of these studies involved patients with only leiomyomatous uteri, whereas this present study included large uterus-size due to the fibroids, adenomyosis, or AUB.
The 3 above mentioned studies, used the sublingual route but the current study used the vaginal route, as misoprostol peak concentration can be reached within 30–60 minutes of administration, and the concentration is maintained for ∼2–3 hours, 13 which lasts until the last clamp is used at the end of operative time. In addition, the vaginal route has been associated with fewer side-effects of pyrexia and shivering than sublingual and oral routes. If general anesthesia is required, oral and sublingual routes can pose risks of aspiration. No serious side-effects occurred due to misoprostol use in the current study.
The strength of this study was that the patient distribution in terms of sociodemographic details and other preoperative parameters matched in both the groups, hence, the results were more reliable. No major complications occurred during the operations, as the adherence to exclusion criteria was strict. The limitation of this study was perhaps the exclusion of 3 patients from the misoprostol group leading to a result bias as the sample-size calculation was for 35 patients in each group for power of study to reach 80%. In addition, vaginal misoprostol tablets might have worked better by wetting them, which was not applied in the present study.
Further studies with higher dosages of vaginal misoprostol could be planned, and its effect on blood loss by a subgroup analysis of different causes of large uteri can help determine whether misoprostol use by sublingual or vaginal route works only for leiomyomatous uteri or for all large uteri.
Conclusions
A single vaginal misoprostol dose prior to total abdominal hysterectomy for a large-size (> 12 cm) uterus did not significantly reduce intraoperative blood loss, the drop in hemoglobin, nor the need for postoperative blood transfusion.
Footnotes
Acknowledgment
The authors would like to thank Dr. Avijit Hazra, MD, for contribution to the article as biostatitician.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
There were no funding from any sources for this trial.