
Abstract
Objective:
To compare the quantity in morphine milligram equivalent (MME) of opioids prescribed at hospital discharge after gynecologic surgery before and after passage of comprehensive New Hampshire state legislation (HB 1423) regulating opioid prescribing.
Design:
A retrospective chart review was performed on all patients undergoing gynecologic surgery between January 1, 2016 and June 30, 2016 (before legislation) and between April 1, 2017 and September 30, 2017 (after legislation) at a single tertiary care center.
Materials and Methods:
The primary outcome was MME prescribed at hospital discharge. Secondary outcomes included discharge without opioids, prescriptions ≤37.5 and ≥200 MME. Type of gynecologic surgery and benign versus oncologic diagnoses were analyzed. A logistic regression model was conducted to determine variables associated with a prescription of ≥200 MME.
Results:
Seven hundred seventy-four patients underwent gynecologic procedures during the identified time periods; 349 patients before legislation and 423 patients after legislation. Significantly fewer mean MME were prescribed after legislation (173 MME vs. 78.5 MME, p < 0.001). This was true for laparotomy with hysterectomy (231 MME vs. 111 MME; p < 0.001), laparotomy without hysterectomy (275 MME vs. 141 MME; p = 0.04), laparoscopic hysterectomy (143 MME vs. 62 MME; p < 0.001), other laparoscopy (133 MME vs. 59 MME; p < 0.001), and vaginal hysterectomy (232 MME vs. 89 MME; p = 0.002) and among those with a cancer diagnosis (178.5 vs. 67.9; p < 0.001). The number of patients discharged without a prescription for opioids significantly increased after legislation (4.4% vs. 9.8%; p = 0.005). In multivariate analysis, surgery before legislation (odds ratio [OR] 14.56 [95% confidence interval 8.22–25.82]), having a laparotomy with hysterectomy (OR 5.85 [2.47–13.85]) or laparotomy without hysterectomy (OR 6.35 [2.35–17.13]) were predictive of a prescription ≥200 MME.
Conclusion:
After opioid prescribing legislation in New Hampshire, significantly fewer opioids were prescribed on hospital discharge after gynecologic surgery. This reduction was seen regardless of type of gynecologic surgery or cancer diagnosis. (J GYNECOL SURG 37:291)
Introduction
The incidence of opioid overdoses and overdose deaths has increased twofold for the past decade, leading to a national crisis in the United States. Rural areas have been especially impacted by the opioid epidemic and New Hampshire has had some of the highest overdose death rates in the nation. 1 Opioids prescribed by health care providers have contributed to the epidemic. In 2017, of the 47,600 overdose-related deaths, 17,029 were attributable to prescription, rather than illicit, opioids. 2 There is increasing evidence that opioids are prescribed in excess after surgery with excess medications becoming a source for potential diversion and illicit use.3,4 In New Hampshire in 2016, there were 64.3 opioid prescriptions written for every 100 people. 5
There is limited evidence to support when, and at what doses, opioids should be prescribed after surgery. Recent studies show that prescribing practices vary widely after common general surgeries even within a single institution.6–8 One study found that opioids were overprescribed postoperatively with 70% of prescribed opioid pills going unused after five common general surgeries. 6
Emerging evidence suggests that outpatient opioid prescriptions after gynecologic surgeries also vary widely and are often more than the patient requires for adequate pain control.9–11 Griffith et al. demonstrated that patients used between 30% and 45% of the prescribed opioid after hysterectomy. 10 As-Sanie et al. reported that patients used half of the prescribed opioids after benign hysterectomy with a median excess of 110 morphine equivalents. 11 A recently published study in the gynecologic oncology literature found that patients reported using 43% of their prescribed opioid pills after minimally invasive hysterectomy. 12
In efforts to reduce the total amount of prescribed opioid per capita, many states have enacted legislation regulating opioid prescribing, ranging from laws specifically focusing on prescriptions for chronic pain to requiring utilization of prescription drug monitoring programs (PDMPs). 13 By the end of 2017, 26 of states had laws specifically limiting prescriptions for acute pain, most of which were passed in 2017. 14 The impact of state-specific regulations on opioid prescribing practices for acute pain in the postoperative period remains unknown. 15 On January 1, 2017, New Hampshire enacted HB 1423 mandating a five-step approach for providers to prescribe opioid narcotics for acute pain, as shown in Table 1. 16 Before this legislation, New Hampshire did not have any legislation restricting provider prescribing practices for treating acute pain with opioids. Of note, except in prescriptions written in the emergency room or acute care clinics, the New Hampshire regulation did not limit the morphine milligram equivalents (MME) that could be prescribed in either a single prescription or for a given time period, but rather concentrated on patient-informed consent and provider education. In addition, patients with cancer-related pain were specifically excluded from this legislation.
New Hampshire 2016 Health Bill 1423
The primary objective of our study was to determine the impact of state legislation on opioid prescribing practices at hospital discharge after benign and oncologic gynecologic surgery, measured in morphine milligram equivalents at a single tertiary care center. Secondary objectives included elucidating the percentage of patients who did not require a postoperative opioid prescription, the percentage of patients prescribed >200 and ≤37.5 MME amounts of opioids at the time of discharge and comparing opioids prescribed after benign surgery to oncologic.
Materials and Methods
We conducted a retrospective analysis of patients who underwent gynecologic surgery at an academic medical center during two time periods, between January and June 2016 (before the passage of comprehensive New Hampshire state legislation regulating the prescription of opioids for acute pain) and between April and September 2017 (after the legislation was passed). IRB approval was obtained from the Dartmouth College Committee for the Protection of Human Subjects on December 1, 2018.
Patients were identified as undergoing gynecologic surgery by the physician's current procedural terminology coding system, 4th edition (CPT-4). Those undergoing gynecologic surgery during the study period for either benign indications or cancer diagnoses were included. Patients were excluded if they died before hospital discharge or did not have surgery.
The primary outcome, outpatient opioid prescription provided at the time of hospital discharge, was extracted from the electronic medical record (EMR) and included all prescriptions for codeine, fentanyl, hydrocodone, hydrocodone/acetaminophen, hydromorphone, meperidine, methadone, morphine, oxycodone, oxycodone/acetaminophen, oxycodone/naloxone, tramadol, and oxymorphone written at the time of discharge from the hospital after the identified surgery. These prescriptions were then converted to morphine milligram equivalents. 17 Postoperative opioid prescription data were available on all patients.
Secondary outcomes included the percentage of patients discharged from the hospital without a prescription for opioids and the percentage of patients who were prescribed ≤37.5 MME (the equivalent of five tablets of 5 mg oxycodone) and ≥200 MME at the time of discharge (about 26 tablets of 5 mg oxycodone).
To delineate differences in prescribing patterns after different types of gynecologic surgery, procedures were categorized into five distinct categories based on CPT-4 codes: laparotomy with hysterectomy, laparotomy without hysterectomy, laparoscopic hysterectomy, other laparoscopic procedures, and vaginal hysterectomy (Table 2). Cancer diagnoses were verified with pathologic confirmation on chart review. A subgroup analysis of the outpatient prescription opioids prescribed to patients with gynecologic cancer, verified by pathologic confirmation, was then conducted, for ovarian cancer, endometrial cancer, and other gynecologic cancer diagnoses.
Current Procedural Terminology Codes for Included Gynecologic Procedures
The EMRs were reviewed to collect demographic and clinical characteristics of patients, including age, race, ethnicity, body mass index (BMI; kg/m2), smoking status, preoperative alcohol use, preoperative illicit drug use, and preoperative medication-assisted treatment for opioid dependence. Intraoperative events included length of surgery and estimated blood loss (EBL). Information on length of stay, type of admission (same-day surgery, 23-hour observation, and inpatient admission), surgeon, and surgeon's board certification (general OB/GYN, gynecologic oncology and female pelvic medicine and reconstructive surgery) were also collected. Cancer diagnosis was verified by pathology review.
Descriptive and comparative statistics—including Student's t-test, chi-squared analysis and Fisher's exact test (two-tailed)—were used to compare demographic variables and MME between the pre- and postlegislation groups. A logistic regression model was conducted to further identify risk factors associated with patient discharge with a prescription for opioids ≥200 MME. Variables associated with the outcome of discharge with a prescription of >200 MME were first identified for potential inclusion in the final model based on bivariate analysis (p < 0.05). We tested for associations between the attending physician and change in MME prescribed, but these associations were not significant and attending surgeon was not included in our final model. These variables were then added to the regression analysis model in a stepwise manner using likelihood ratio testing. The likelihood ratio test statistic was used to compare the chi-squared distribution of the model and a p-value was calculated. Only variables with a p-value of <0.05 based on likelihood ratio testing were included in the final model; therefore, some variables identified on univariate analysis were not included in the final regression model as they did not significantly impact the analysis. The goodness-of-fit of the model was confirmed with the Hosmer–Lemeshow test (p > 0.05). Adjusted odds ratios and 95% confidence intervals (CI) were calculated. Statistical analysis was performed using STATA 11.0 (StataCorp, College Station, TX).
Results
Patient characteristics
This retrospective analysis included 774 patients who underwent gynecologic surgery with 19 attending surgeons during the identified time periods. Of this cohort, 349 patients underwent surgery with 15 attending surgeons before January 1, 2017 and 423 patients underwent surgery with 16 attending surgeons after passage of the legislation. Two patients from the prelegislation time period were excluded due to death before hospital discharge. Race, BMI, cancer diagnosis, operative time, EBL, length of hospital stay, attending surgeon did not differ significantly between patients undergoing surgery before and after legislation (Table 3). Mean patient age was 2.6 years older in the postlegislation group (52.4 years vs. 55.0 years; p = 0.019). No significant difference was seen in type of gynecologic surgery performed between the pre- and postlegislation. The only significant difference identified between the pre- and postlegislation cohorts was receiving a prescription for opioids in the 30 days before surgery (18.5% vs. 11.3%; p = 0.007), which may have represented a prescription given to the patient at their preoperative visit for postoperative use or a prescription to manage pain symptoms before their surgical procedure.
Demographics and Clinical Characteristics, Intraoperative Events, and Postoperative Complications (N = 772)
Opioid risk score was not collected on patients before the 2017 legislation.
MAT, medication-assisted treatment; SD, standard deviation.
Morphine milligram equivalents prescribed
The MME prescribed at the time of hospital discharge significantly decreased after adaptation of HB 1423, from 173.0 (± 155.3) MME to 78.5 (± 65.0) MME (p < 0.001). This decrease in MME prescribed was observed across all types of gynecologic surgery, including laparotomy with hysterectomy (231.3 ± 134.8 vs. 111.4 ± 69.6; p < 0.001), laparotomy without hysterectomy (275.2 ± 280.7 vs. 141.3 ± 141.7; p = 0.04), laparoscopic hysterectomy (143.4 ± 69.5 vs. 61.8 ± 47.5; p < 0.001), other laparoscopy (132.5 ± 85.5 vs. 58.6 ± 40.8; p < 0.001), and vaginal hysterectomy (231.5 ± 305.2 vs. 88.6 ± 44.3; p = 0.002) (Fig. 1). After adaptation of this new legislation, a much higher percentage of patients were discharged with prescriptions of ≤37.5 MME (4.94% vs. 39.0%; p < 0.001) and significantly fewer patients were discharged with large prescriptions defined as ≥200 MME (31.5% vs. 4.91%; p < 0.001). Significantly more patients were also discharged without any opioid prescription (4.43% vs. 9.82%; p = 0.005). Finally, the maximum mean MME for a single patient decreased significantly (1950 vs. 480; p < 0.001).
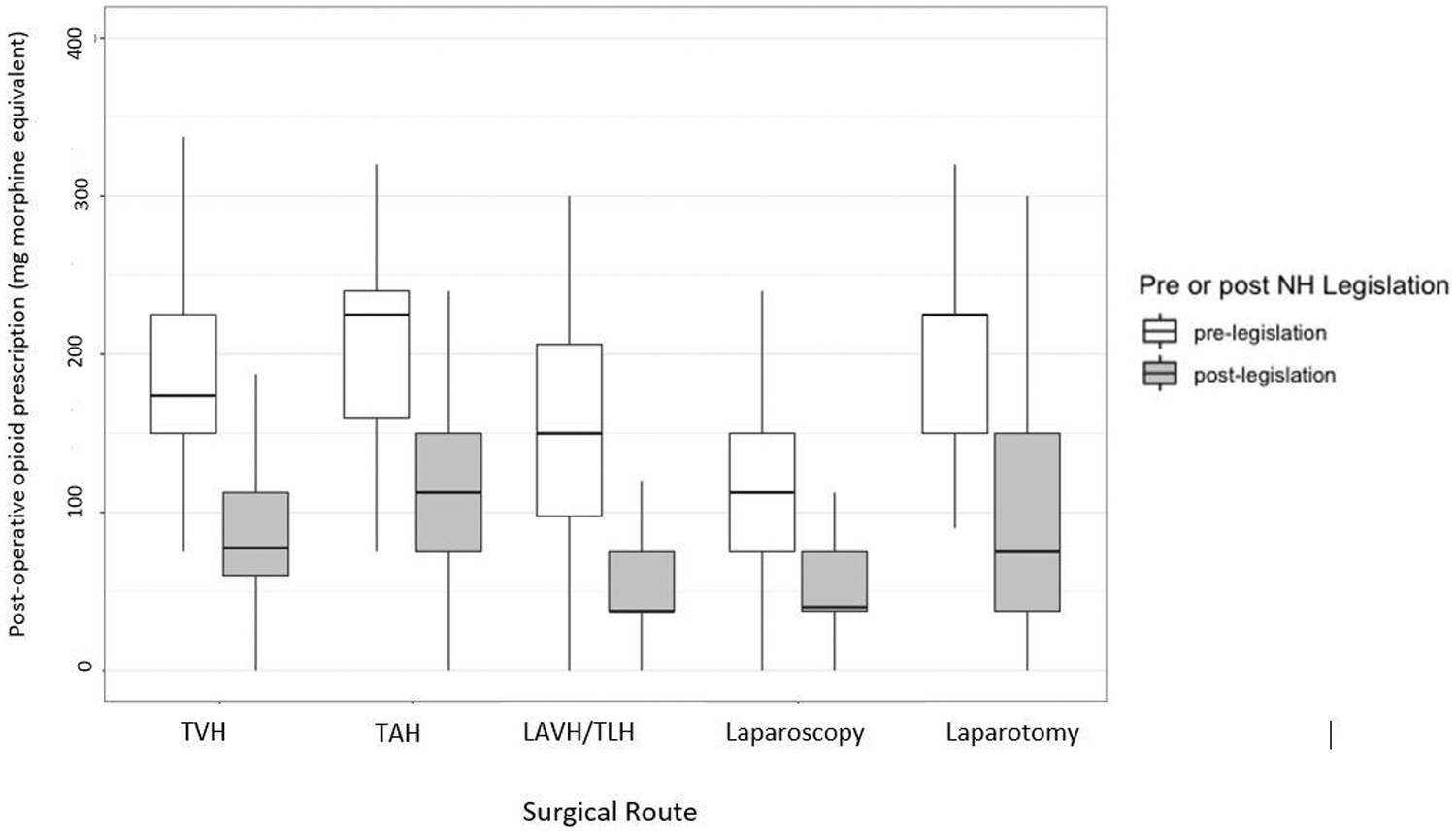
Box plot of morphine milligram equivalents of opioids prescribed at discharge after gynecologic surgery before and after passage of New Hampshire state legislation. LAVH/TLH, laparoscopically assisted vaginal hysterectomy/total laparoscopic hysterectomy; TVH, vaginal hysterectomy.
Subgroup analysis of patients with a verified gynecologic cancer diagnosis
Among patients who underwent gynecologic surgery for a cancer diagnosis, there was a significant decrease in the MME prescribed postlegislation adaptation. Before the legislation, the mean opioid discharge prescription among patients with cancer was 180.9 (± 14.5) MME compared with a mean prescription of 66.6 (± 5.8) MME after legislation (p < 0.001). The decrease in opioid prescribing was observed in all three categories of gynecologic cancer surgery, including ovarian cancer [245.9 (± 226.5) MME vs. 107.7 (± 96.7); p < 0.001], endometrial cancer [131.1 (± 71.6) vs. 51.2 (± 41.8); p < 0.001], and other gynecologic cancers [306.9 (± 326.3) vs. 52.5 (± 38.6); p = 0.02] as shown in Figure 2.
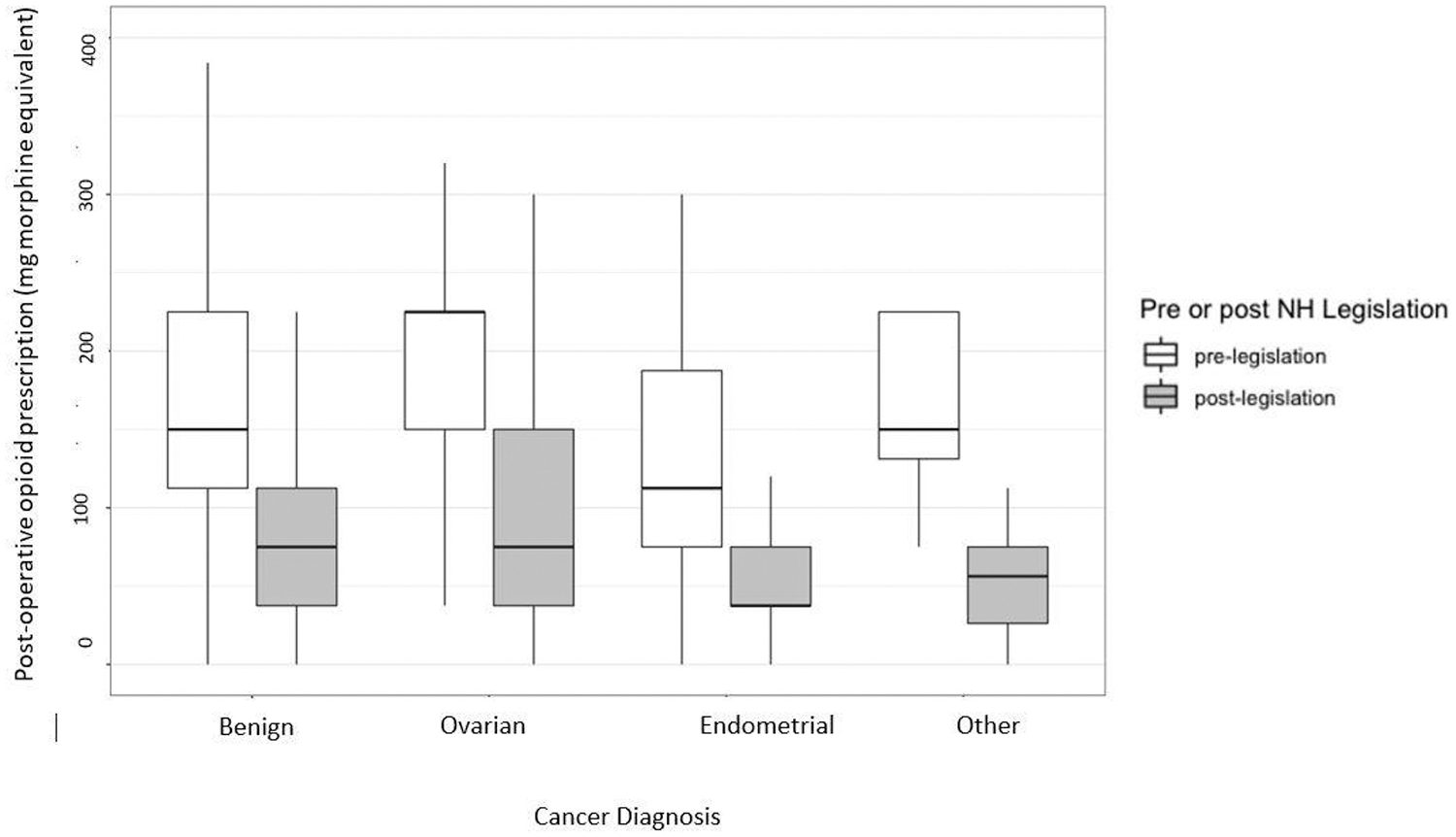
Box plot of morphine milligram equivalents of opioids prescribed at hospital discharge after gynecologic surgery for confirmed gynecologic cancer before and after passage of state legislation.
Regression analysis
Multivariable logistic regression was performed to determine potential factors that may predict a large postoperative opioid prescription of ≥200 MME. After adjusting for having surgery before the legislation, age, type of surgery, cancer diagnosis, and type of discharge, receiving a large postoperative opioid prescription was associated with having surgery before legislation (OR 14.56 [95% CI 8.22–25.82]), having a laparotomy with hysterectomy (OR 5.85 [95% CI 2.47–13.85]) or laparotomy without hysterectomy (OR 6.35 [95% CI 2.35–17.13]). Both individual surgeon and subspecialty of the surgeon were explored as factors that might potentially impact the final model; however, neither did and these variables were not included in the final model.
Conclusion
In this retrospective review of 774 patients who underwent gynecologic surgery in a single tertiary care setting, we observed a significant decrease in the mean amount of MME prescribed after passage of state-specific legislation on provider opioid prescribing practices, NH HB 1423. After adaptation of this legislation, there was a 55% decrease in the MME prescribed at the time of hospital discharge after any gynecologic surgery. With this legislative mandate bringing opioid prescribing practices into focus for all providers, fewer patients were discharged with large opioid prescriptions, defined as >200 MME. More notably, significantly more patients were also discharged without any opioids. These trends in decreased opioid prescribing were also seen in a cohort of patients who underwent gynecologic surgery for a confirmed cancer diagnosis. It should be noted that some predictors that were not significantly associated with the outcome occurred rarely (5% or fewer cases). Statistical power to detect significant associations for these variables were, therefore, limited.
In the past decade, many states have passed legislation regulating the prescription of opioids, but the impact of these laws has not been well studied. Likewise, it is known that postoperative prescriptions vary widely, including after gynecologic surgery, but little is known what influences prescribing practices. This study indicates that state legislation impacts postoperative opioid prescriptions after gynecologic surgery, in a state particularly affected by the opioid abuse epidemic.
This effect was observed across patients undergoing surgery for a range of indications, including for oncologic diagnoses. We choose to include oncologic patients as we hypothesized both the state legislation and significant attention given in the state of New Hampshire to opioid prescriptions would be noticed in both oncologic and benign patient populations. In New Hampshire, as well as many states with opioid prescribing legislation, cancer patients are often excluded from opioid-prescribing laws given the chronic and complex nature of cancer-related pain; however, we included this population as we felt that changes in practice would be notable in both the cancer and benign populations.
Further study is needed to determine how many prescriptions provided at the time of hospital discharge are filled by the patient, as well as how many pills are taken. It would be helpful to follow patients to their postoperative visit to evaluate for adequacy of pain control, postoperative activity, as well as assess changes in quality of life score.
Unlike other states, including neighboring Vermont, New Hampshire state law does not limit the amount of opioids prescribed at one time, allowing the provider and patient to practice shared decision-making. Furthermore, reviewing the risks and benefits of opioids using an opioid consent form provides providers an avenue for setting expectations and providing patient education regarding expected pain and recovery after surgery. This proactive discussion in the preoperative period likely affects the amount of MME that patients expect to receive and use postoperatively.
Larger studies and analyses are also needed to examine if these significant decreases in opioid prescribing practices can decrease the prevalence of opioid addiction, opioid overdoses, and overdose deaths attributable to prescription opioids. A commonly voiced concern is that decreasing prescribed opioids per capita will lead to a shift in illicit opioid consumption and subsequent increase in overdose deaths. According to the CDC, both the opioid prescribing rate and opioid-related deaths decreased in the state of New Hampshire in 2017. 5 These trends will need to be followed to ensure that the decrease in provider prescribing is having positive, not negative, impacts on opioid addiction rates and opioid-related deaths.
The strengths of this study include that all opioids were prescribed by providers in the EMR rather than using handwritten prescriptions, allowing for accurate data collection. The number of attending surgeons was stable between the two time periods. Often, prescriptions were written by a resident trainee under the supervision of an attending, and we were able to track this in the EMR. We chose to analyze the data by attending surgeon as attending preferences are specified to residents. We also used a washout period before and after passage of HB 1423 to allow for practice changes in anticipation of impending legislation and adjustment of new practices after legislation.
As this study was designed to examine provider prescribing practices and due to the retrospective nature of this analysis, we were able to measure written prescriptions; however, we were not able to measure filled prescriptions. Although the literature suggests that opioids may be commonly overprescribed in the postoperative period, we were not able assess the adequacy of patient perceptions of postoperative pain control after discharge. Changes in societal perception of opioids and thus impacting patient preferences for pain control during the study time may provide confounding factors in this study. As this legislation included multiple components that were enacted simultaneously, we were unable to examine if one aspect of the legislation may have been more influential than another aspect.
In a state particularly devastated by opioid abuse, legislation mandating providers obtain continuing medical education on opioids, obtain informed consent for the prescription of opioids, conduct a risk assessment for opioid addiction, query a PDMP database, and document counseling around nonopioid pain management, was associated with a decrease in the amount of opioid prescribed at hospital discharge after gynecologic surgery. Furthermore, significantly more patients were discharged without a prescription for opioids. Given that there is evidence that opioids are often overprescribed after gynecologic surgery, this is an important observation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Dr. Wilkinson-Ryan is supported, in part, by a career development award. Funding and resources provided by p-30CA023108, the Norris Cotton Cancer Center and the Dartmouth-Hitchcock Cancer Faculty Fellows Program.