
Abstract
Study Objective:
To further explore the potential of vaginal natural orifice transluminal endoscopic surgery (vNOTES) as a modality of adnexal surgery at the time of hysterectomy in a residency training program.
Design:
Retrospective pilot study.
Setting:
Charleston Area Medical Center OB/GYN Residency, a tertiary care center and residency training facility located in Charleston, WV.
Patients:
Female patients aged 18 years and above undergoing vaginal hysterectomy and adnexal surgery for benign gynecologic indications.
Interventions:
No interventions were rendered.
Main Results:
In total, 29 cases were included in the pilot study. One out of 29 (3%) was readmitted to the hospital after vNOTES. No intraoperative surgical complications occurred. Two out of 29 (7%) vNOTES attempts were abandoned for traditional total vaginal hysterectomy with traditional adnexal surgery. No postoperative wound infection, cuff dehiscence, or unintended visceral injury occurred. These are comparable with outcomes to other modalities of hysterectomy.
Conclusion:
Our study demonstrates the safety and utility of vNOTES in the setting of a residency training program. In doing so, it is the hope of this study that it will inspire the use of vNOTES in other training programs in the United States, as improved vaginal surgical skills are critical to resident education. Ultimately, the authors feel that vNOTES will improve patient satisfaction with incision-free surgery without compromising safety. (J GYNECOL SURG 37:232)
Background
Natural orifice transluminal endoscopic surgery (NOTES) was originally successfully performed and implemented in gastroenterology/general surgery circa 2004, utilizing rectal and oral access. 1 NOTES was heralded as a novel method of peritoneal access subverting the need for skin incisions. The theoretical utility of the surgical method takes advantage of the relatively rapid healing of nonkeratinized epithelium, optimizing wound healing. It took 10 years before the procedure was modified for the gynecologic theater.
For gynecologists, it is well known that the vaginal epithelium rapidly heals and vaginal surgery has been performed safely for generations. Although not without risk, vaginal surgery has demonstrated improved postoperative pain, shorter admission duration, and shorter operative times. 2 In many ways, vaginal surgery has been the conventional “natural orifice” surgery. It is a natural transition, therein, for NOTES procedures to be utilized in gynecologic surgery. To the best of our knowledge, Dr. Baekenlandt was one of the first individuals in the world to utilize natural orifice surgery in the realm of gynecology.3,4 His studies have demonstrated the feasibility of vaginal natural orifice transluminal endoscopic surgery (vNOTES)5,6 and inspired our efforts in this pilot study.
After Dr. Baekenlandt's success, a small number of other studies since that time have been done, most notably in Taiwan.7–11 These studies have immense promise, as many found vNOTES was associated with lower blood loss, shorter hospital stay, and less postoperative pain.11,12 However, beyond the small number of case series and literature reviews available, limited studies in the United States have been published on vNOTES. The population of patients in the United States13,14 is considerably different from that of Belgium and Taiwan, ranging from differences in access to care to patient profiles and comorbidities. This disparity of information germane to the patient population of the United States was an additional inspirational factor for developing our study.
It is important to mention that vNOTES is particularly useful for adnexal surgery at the time of vaginal hysterectomy, which offers safe direct visualization of adjacent anatomy. We highlight this because growing evidence suggests that salpingectomy, in particular, may reduce the risk of epithelial ovarian cancers. 15 This has been one of the main advantages of the laparoscope-assisted vaginal hysterectomy (LAVH) over total vaginal hysterectomy (TVH), which has a failure rate of salpingectomy and/or oophorectomy at the time of surgery that approaches 33%, according to opinion 701. 16 As many experienced surgeons know, adnexal surgery can be technically challenging in a traditional TVH, and is difficult to assess in the preoperative period; however, when using the vNOTES technique, this challenge is reduced due to the additional visibility granted to the surgeon as well as access to key adnexal anatomy necessary for removal. The use of vNOTES as an adjunct may encourage gynecologists to utilize TVH more often, which is particularly important due to the lower complication rates and better postoperative pain over other routes of hysterectomy such as LAVH (Table 1). 16
Results in Sum
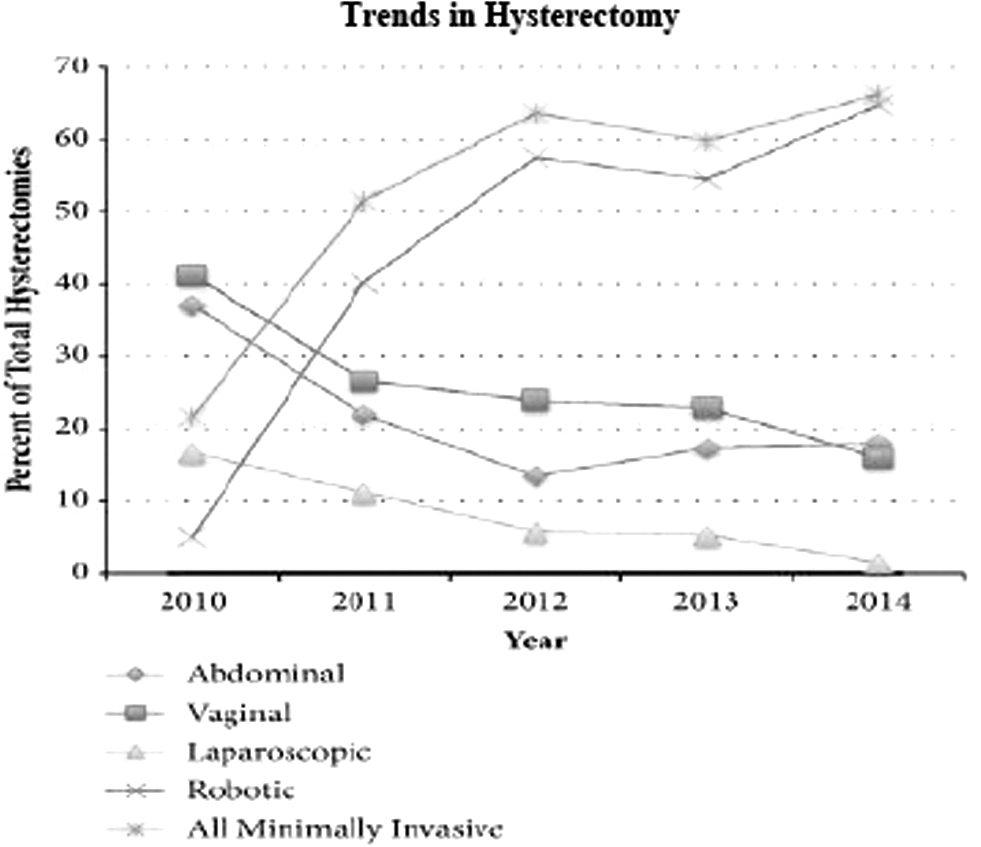
Unfortunately, it appears that the classical vaginal surgical skills in gynecology are at risk of being lost. As already mentioned, vaginal hysterectomies in OB/GYN residencies are decreasing16,17 (Fig. 1). The hallmark of gynecologic surgery appears to be slowly phasing out, this is an unsettling trend. Over time, the vaginal surgical skills that have been cultivated over many generations in our discipline may be diminished to an unrecognizable level, which will do both our young gynecologists and our patients a disservice. This is yet another potential benefit of vNOTES, wherein the vaginal skills of the experienced attending physician may be passed down to the next generation of gynecologists while simultaneously capitalizing on the laparoscopic skills of the new. The authors firmly believe that vNOTES has the potential to be at the forefront of minimally invasive surgery in select patients.
Technique
vNOTES technique varies among surgeons at our institution; however, the technique can be defined in one of two approaches:
Traditional TVH is completed. Upon completion, the vaginal wound retractor is placed within the peritoneum, taking care to assure placement of the retractor beyond the peritoneal edge anteriorly and posteriorly. It is then made taut. The single-site port is placed and the peritoneal cavity is insufflated appropriately to ∼15 mmHg. A camera, preferably with a 10 mm, 30° scope, is assembled and placed through a port site of the single-site apparatus and anatomy is visualized. From here, bipolar electrocautery and tissue manipulators are used to complete the salpingectomy and/or oophorectomy. Upon completion of adnexal surgery, the instruments are removed. The single-site port is removed along with the wound retractor, and peritoneal insufflation is naturally released (Figs. 2 and 3). The vaginal cuff is closed vaginally.
Successfully placed wound retractor after successful TVH. TVH, total vaginal hysterectomy. Appearance of single-site port applied to wound retractor. The initial steps of TVH are completed, namely colpotomy, dissection of cervical stroma, and entry into the anterior and posterior peritoneum. The first pedicle incorporating the uterosacral ligaments is clamped, cut, and ligated on either side. The anterior and posterior peritonea are optionally tagged with Vicryl. Thereafter, the vaginal wound retractor is placed within the peritoneum, and a traditional TVH is performed utilizing laparoscopic bipolar electrocautery to cauterize and transect the subsequent pedicles, including the uterine arteries. Broad and round ligaments are thereafter resected in a similar manner. The adnexal surgery is performed after extraction of the liberated uterus as already outlined.


We have included videos demonstrating the vNOTES procedure at our hospital. Please see figures two and three for images of the vNOTES procedure.
Methods
An observational retrospective review of the medical records of patients who had a vNOTES procedure at the time of hysterectomy performed at our hospital over the past 3 years was conducted. We reviewed 29 cases in sum. We measured readmission rates, surgical complications, conversion to conventional minimally invasive techniques (LAVH, TVH, and total laparoscopic hysterectomy), and conversion to open laparotomy. Complications were defined as postoperative wound infection, vaginal cuff dehiscence, and unintended visceral injuries. Descriptive statistics and univariate analysis were used as appropriate for continuous or categorical variables.
Results
In total, 29 cases were included in the pilot study. One out of 29 (3%) was readmitted to the hospital after vNOTES. No intraoperative surgical complications occurred. Two out of 29 (7%) vNOTES attempts were abandoned for TVH with traditional adnexal surgery. No postoperative wound infection, cuff dehiscence, or unintended visceral injury was reported for any patient.
The one readmission was for a vaginal cuff hematoma. This patient had a significant medical history of unprovoked PE in the past and was on lifelong anticoagulation, which she had restarted in the postoperative period in collaboration with her hematologist. She was admitted on postoperative day 5 and discharged on postoperative day 10. She received 4 U of blood and was restarted on Lovenox after reaching stability on heparin as an inpatient. She experienced no further complications.
These results are comparable with outcomes of other standard means of hysterectomy. Our overall complication rate falls within the range of 2%–3%, which is quoted in the national literature. 18
Discussion
We believe given that these findings are similar to currently accepted modalities, vNOTES is a worthwhile safe alternative to currently accepted modalities of minimally invasive hysterectomy. Our study has the unique strength of being the first of its kind to be done at a resident program with nonfellow residents being primary participants using this novel surgical technique. It also has the strength of delineating multiple viable surgical techniques with attached outcomes to further advance knowledge and studies toward the goal of developing an optimal surgical technique.
One weakness in this study is that it is underpowered. The relatively low number of cases is expected in a pilot study. The potential benefit of vNOTES justifies, in our opinion, the need to develop research on this novel surgery. In addition, outcomes were not directly compared with cases of other hysterectomy routes at Charleston Area Medical Center, limiting our ability to directly compare hysterectomy routes. As an additional weakness, this is a retrospective study, which makes it more liable for bias, confounding, and prevents causative conclusions from being drawn. A future prospective study would be a marked improvement to address this weakness, and it is our intention to develop subsequent studies on vNOTES incorporating prospective and randomized elements.
Conclusion
vNOTES is an emerging field of minimally invasive surgery with the potential to capitalize on the classical vaginal operative skills of gynecology while offering novel laparoscopic advantages to adnexal removal without having to make abdominal incisions. Although our study is certainly far from drawing an authoritative conclusion in favor of vNOTES, it demonstrates the applicability of vNOTES to our field. Developing the surgical technique in a residency is possible, and it is our hope that we inspire more research on this interesting novel surgery.
Footnotes
Author Disclosure Statement
Authors C.C., L.T., L.T., A.M., and S.B. have no conflicts of interest to disclose. Author S.B.II is faculty for an applied medical course.
Funding Information
No funding was received for this work.