
Abstract
A 23-year-old G2P0020 presented with a large anterior subserosal hematoma after dilation and evacuation at 19 weeks in the setting of anterior cervical laceration during dilator placement. Owing to hemodynamic instability and brisk vaginal bleeding soon after presentation, she underwent diagnostic laparoscopy, which confirmed the large anterior subserosal hematoma and subsequently underwent bilateral uterine artery embolization. On POD 16, she presented again with brisk vaginal bleeding and had imaging concerning for a communication between the hematoma and uterine cavity, as well as hematoma superinfection. She underwent emergent exploratory laparotomy, which revealed copious old malodorous blood in the hematoma and necrotic uterine tissue with an underlying defect. The necrotic tissue was debrided and the uterine defect was repaired. Postoperative course was subsequently uncomplicated. This is an important lesson from both a trainee and faculty perspective, as hemorrhage into the subserosal space is a rare but potentially life-threatening complication of surgical abortion that should be considered when evaluating a patient postoperatively with hemodynamic instability.
Case
Twenty three year-old G2P0020 presented to the emergency department for severe pelvic pain, postabortion hemorrhage, and hypotension after dilation and evacuation (D&E) at 19 weeks gestation a few hours prior at an outside clinic.
The D&E was complicated by suspected anterior cervical laceration, which was repaired at time of surgery. Upon arrival to the emergency department, abdominal and pelvic examination revealed a large firm suprapubic mass at the level of the umbilicus. The patient was noted to have a drop in hemoglobin from 11.3 preoperatively (reported by outside clinic) to 10.6 in the emergency room. Transabdominal ultrasonography revealed a well-contracted uterus with clearly delineated endometrium without evidence of retained products of conception, as well as 13 × 12 × 8 cm collection in the anterior lower uterine segment and cervix, suspicious for a contained hematoma within the myometrium and cervix, which did not appear to communicate with the endometrium. The collection was causing significant caudal displacement of the uterus.
Owing to worsening pain, ongoing vaginal bleeding, and hemodynamic instability, the massive transfusion protocol was activated and the patient was taken emergently to the operating room (OR) after being consented for examination under anesthesia, repair of cervical lacerations, diagnostic laparoscopy, possible hysterectomy, possible laparotomy, and possible embolization by interventional radiology (IR). She received antibiotic prophylaxis in the OR. Examination under anesthesia was difficult due to significant caudal displacement of cervix, but revealed excellent hemostasis of the repaired anterior cervical laceration. Diagnostic laparoscopy revealed a 14 cm anterior uterine hematoma contained within the myometrium and serosa, extending into bilateral broad ligaments. The hematoma appeared to be stable in size, not expanding, and there was no active bleeding into the peritoneal cavity. Vaginal bleeding had subsided. We suspected a false passage was made within the myometrium with an instrument at time of the D&E resulting in hemorrhage and extravasation of blood into the surrounding myometrium. Because of concern for massive hemorrhage if an attempt was made to drain the hematoma and identify the source of bleeding, a decision was made to not evacuate the hematoma to allow continued tamponade of the bleeding site. The patient became hemodynamically stable with blood product replacement.
The patient was transferred directly to IR and underwent emergent bilateral uterine artery embolization. Total blood loss was estimated to be 2500 mL based on the estimated volume of the hematoma (2 L) and the estimated volume of vaginal bleeding (500 mL). In total, she received 3 U of packed red blood cells (pRBCs) and 2 U of fresh frozen plasma in the OR, 5 U of cryoprecipitate in the postanesthesia care unit due to a fibrinogen of 178, and an additional 2U pRBCs, 2U platelets, and 5U cryoprecipitate on POD 1. She remained hemodynamically stable with no further bleeding, had significant improvement in pain, and was discharged home in stable condition on POD 1.
On POD 14, she presented to the clinic for follow-up and was found to have malodorous dark brown bloody discharge on pelvic examination. No active vaginal bleeding was noted. Transvaginal ultrasonography (Fig. 1) revealed continued presence of anterior uterine hematoma with thin lower uterine segment and possible communication between the hematoma and endometrium. In addition, possible air or gas seen within the hematoma raised suspicion of infection. She was sent to the emergency department for further evaluation, where computed tomography (CT) scan (Fig. 2) confirmed these findings. Given lack of other infectious symptoms and minimal bleeding at time of evaluation, the patient was discharged home with strict return precautions and the plan for outpatient follow-up.
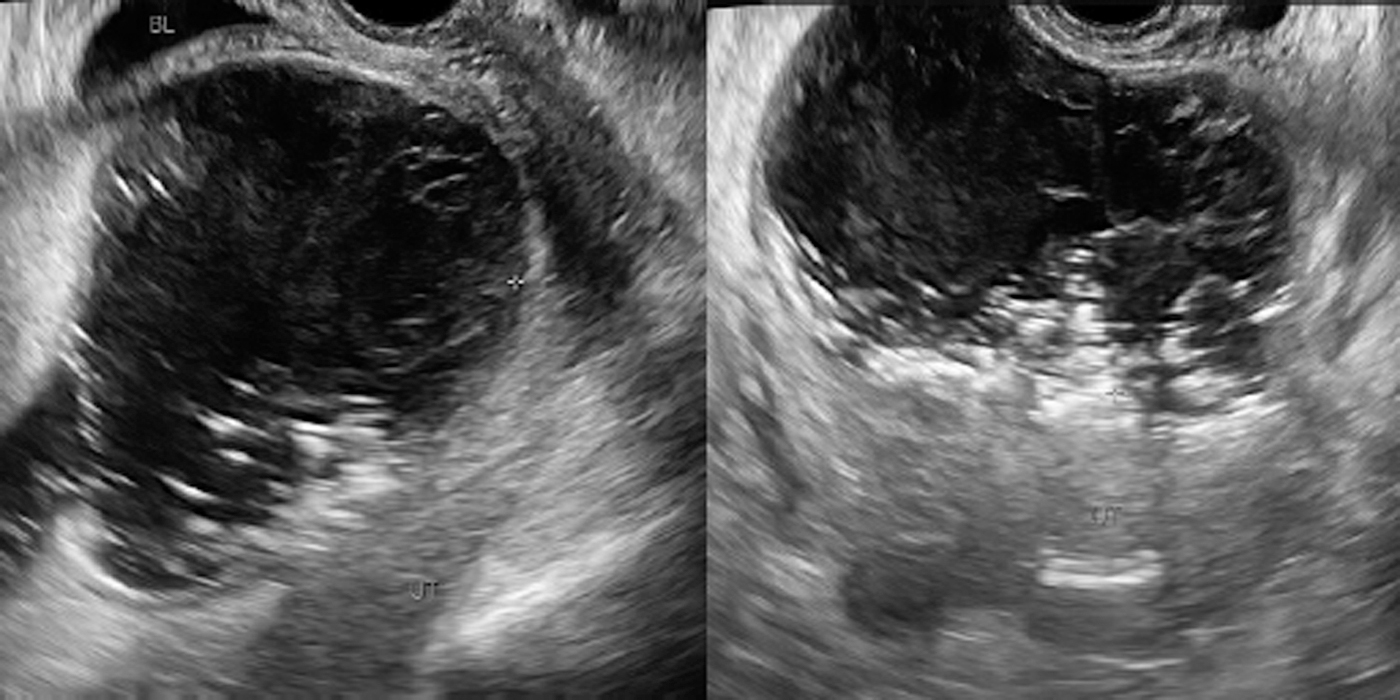
Postoperative day 14 transvaginal ultrasound.
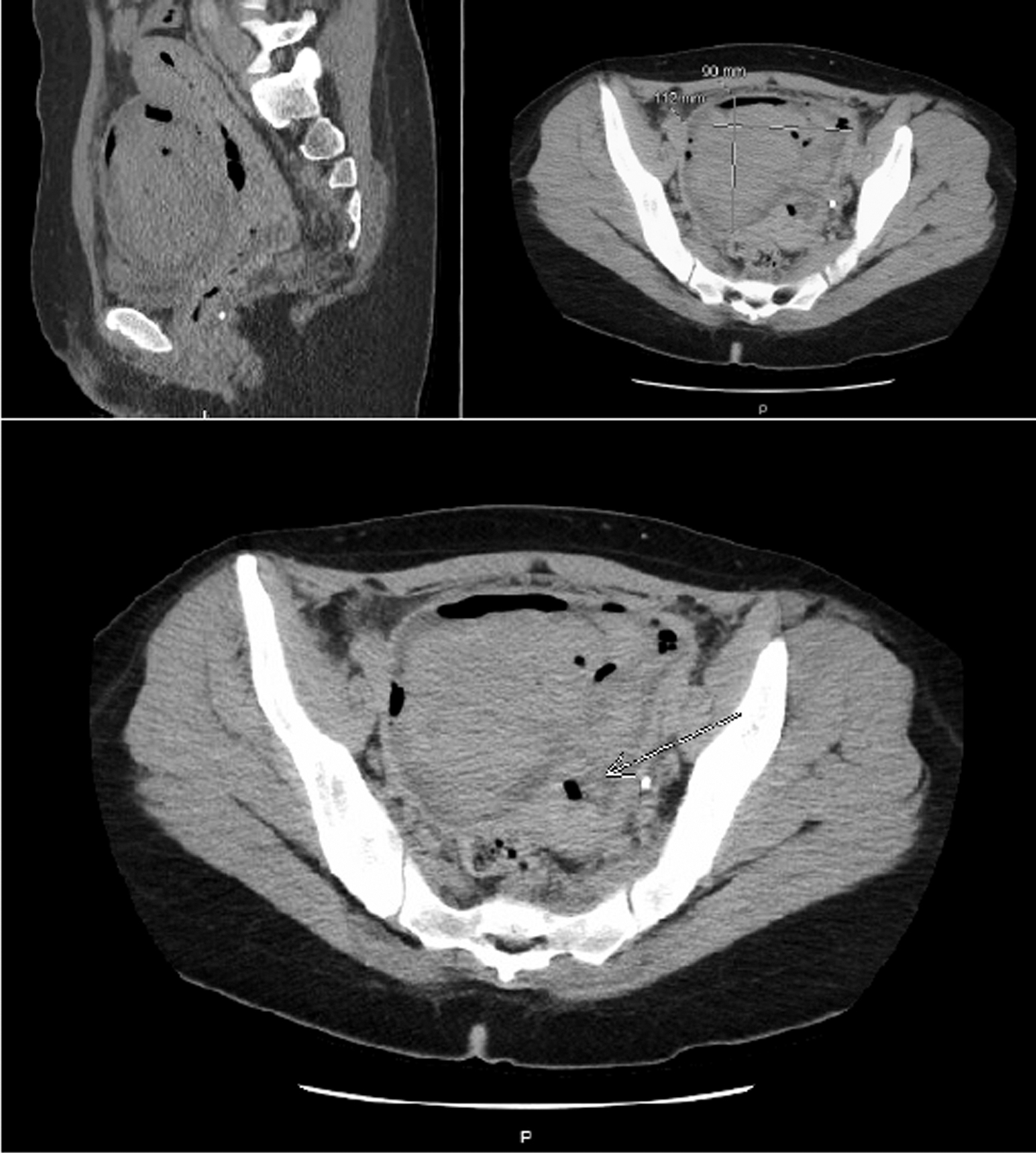
Postoperative day 14 CT scan. Arrow pointing to possible communication between hematoma and endometrial cavity. CT, computed tomography.
She subsequently presented to the emergency department on POD 16 with sudden onset brisk vaginal bleeding after attempted tampon usage. She reported no other bleeding in the interim since her discharge from the hospital. She underwent emergent exploratory laparotomy, and was found to have a large necrotic hematoma of the anterior lower uterine segment. The hematoma was opened revealing malodorous old blood with an underlying uterine defect and surrounding necrotic uterine tissue. The hematoma was evacuated and necrotic tissue debrided, leaving a 6 × 5 cm uterine defect (Fig. 3), which was repaired. The patient received an additional 2U pRBCs and 24 hours of gentamicin/clindamycin. She was discharged on POD 2 in stable condition. Her postoperative recovery course was uncomplicated.

Intraoperative image from postoperative day 16 exploratory laparotomy.
Review
Although the overall morbidity and mortality rate from induced abortion is low (markedly lower than that same rate for full-term pregnancy and childbirth 1 ), cervical laceration and/or uterine perforation are some of the possible complications seen. In general, higher incidences of these complications are reported in previous studies, before improvements in methods that include cervical preparation. Cervical lacerations have been reported in 0.1%–2.1% of second trimester abortions2,3 and uterine perforation in 0.2%–0.5%.2,3 Postabortion hemorrhage, defined as >500 mL blood loss, has been shown to occur in 0.1%–2.1% of D&E procedures.2,3 Although atony is the most common cause of postabortion hemorrhage,2,4 uterine perforation and cervical laceration are also potential causes of hemorrhage and should be considered at the time of diagnosis. There is very little literature available regarding subserosal hematoma as a complication of surgical abortion. One case report from Japan discusses a retroperitoneal hematoma under the broad ligament after dilation and curettage (D&C) as a result of lateral cervical laceration, which manifested clinically as worsening abdominal pain. 5 As this is a rare occurrence, the authors are not aware of any larger studies describing this phenomenon.
Trainee's Perspective
Typically, trainees are taught to consider uterine perforation in the setting of clinical signs of intraperitoneal bleeding after D&C and to consider cervical laceration in the setting of ongoing vaginal bleeding not responsive to uterotonics. Although this patient ultimately did have heavy vaginal bleeding on POD 16, her primary symptoms at initial presentation were worsening lower abdominal pain (no peritoneal signs) and hemodynamic instability. This case was an unusual presentation in which a presumed high-cervical/low-uterine perforation caused a contained subserosal hemorrhage. Because the blood did not spread intraperitoneally, she did not display typical signs of intra-abdominal hemorrhage. In addition, because the bleeding did not initially manifest vaginally, the extent of hemorrhage was underestimated.
This is an important lesson from a trainee perspective, as recognizing the contained subserosal hemorrhage was critical in preventing further morbidity. Although rare, knowledge of this possible complication after surgical abortion will help with early recognition and appropriate treatment in the future. In addition, the possibility of uterine necrosis and dehiscence due to a superinfected subserosal hematoma is another important lesson to be learned, as early recognition and management could prevent subsequent hemorrhage and/or infection. Given the subsequent superinfection and necrosis, it is important to retrospectively consider hematoma drainage as an alternative intervention at the time of initial diagnosis, as that may have prevented the subsequent complications. However, given the acuity of the hematoma formation and patient's hemodynamic instability, the risks of further hemorrhage at the time of diagnostic laparoscopy, in the setting of an already high blood loss, likely outweigh the benefits of hematoma evacuation at that time.
In addition, patient counseling after this incident is an important learning point. The patient was counseled extensively regarding the importance of avoiding pregnancy in the near future, as she is at high risk of pregnancy complications, likely similar in nature to someone who has recently had a myomectomy or cesarean section, given that the uterine defect extended through the entire anterior lower uterine segment wall. Even if she were to delay pregnancy an appropriate amount of time, there is some evidence that uterine artery embolization predisposes to miscarriage and postpartum hemorrhage, among other outcomes during pregnancy. 6
Faculty's Perspective
Although most residency training programs offer extensive training in management of postpartum hemorrhage, exposure and instruction in management of postabortion hemorrhage and complications may be limited, especially in medical centers with a lower volume of uterine evacuation procedures. However, training in management of postabortion hemorrhage and complications is crucial. Ob/Gyn physicians may not only be responsible for managing complications from their own uterine evacuation procedures, but are also often responsible for the care of patients who present to emergency departments with postabortion complications related to procedures performed at family planning facilities in the community. Transfer of patients from outside facilities presents an additional challenge in that less information may be available and a broader consideration of potential complications must be considered.
This case was unique in that the postabortion hemorrhage was largely contained within a defect in the uterus. Some of the clinical findings often associated with uterine perforation and postabortion hemorrhage were absent (ultrasonography revealing free fluid/blood in the peritoneum, large volume of vaginal bleeding, peritoneal signs on clinical examination). Despite the lack of heavy vaginal bleeding, the patient's hemodynamic stability decompensated rapidly, indicating significant blood loss and the need for transfusion and emergent surgical exploration. Recognition of the need for emergent intervention, even in the absence of typical findings after uterine evacuation, is a critical element of training.
Regardless of a residency program's clinical and didactics curriculum related to abortion training, instruction in the diagnosis and treatment of postabortion complications and hemorrhage is an important component of residency training.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.