
Abstract
Objective:
To evaluate the efficacy of intraperitoneal subdiaphragmatic instillation of ropivacaine on shoulder tip pain (STP) or upper abdominal pain postoperatively after gynecological laparoscopic surgery.
Design:
It was a parallel-arm randomized controlled trial conducted in a private tertiary care center between October 2017 and January 2020. A total of 118 participants in two study groups were analyzed.
Materials and Methods:
Women in the study group (Group A) received 40 mL of 0.2% ropivacaine, sprayed under the diaphragm immediately after the creation of pneumoperitoneum. Women in the control group (Group B) did not. Postoperative STP was assessed by using the visual analogue scale at 1, 4, 12, and 20 hours after surgery. The pain scores and requirement of postoperative analgesia were compared between the two groups.
Results:
Incidence of STP or upper abdominal pain was significantly higher in the control arm at 12 hours (Intervention arm: 7.4% vs. Control arm: 21.9%; p = 0.039) and at 20 hours (Intervention arm: 3.7% vs. Control arm: 17.2%; p = 0.035) post-surgery. Number needed to treat was calculated as 6.9. An individual in the intervention arm was found to be 75% more protected from the incidence of pain after adjusting for time and individual level clustering (adjusted incidence rate ratio: 0.25, 95% confidence interval: 0.10–0.68, p = 0.006) than the control arm.
Conclusion:
Intraperitoneal subdiaphragmatic instillation of ropivacaine in fertility-preserving laparoscopic surgeries among high-risk patients reduces the incidence of postoperative STP or upper abdominal pain. (J GYNECOL SURG 37:315)
Introduction
Postoperative pain is a common complaint after laparoscopic surgeries. 1 Postoperative pain has a direct impact on patient comfort, duration of hospital stay, and health care costs.2,3 The most frequently reported sites of pain are generalized abdomen, port-site, upper abdomen and shoulder tip pain (STP). Of all the types of pain, STP and upper abdominal pain tend to be most severe and distressing for the patient. 4 Both the STP and upper abdominal pain are pain of a diaphragmatic origin. The cause of STP is due to carbon dioxide (CO2) pneumoperitoneum, and various theories have been proposed to explain the mechanism of pain. One of the theories is that residual pockets of gas leads to loss of suction support of the liver and thereby causes pain. 5 Another explanation is that pneumoperitoneum induces stretching on the peritoneum and the diaphragmatic muscle fibers, which leads to irritation of the phrenic nerve endings. Local hypothermia, peritoneal drying, and diaphragmatic irritation from carbonic acid has also been suggested as another cause for STP. 6
Being the most typical unpleasant post-laparoscopic experience, multiple strategies have been tried over the years to reduce the STP. Many studies have attempted to assess the effect of reduced abdominal stretching by creating a low-pressure pneumoperitoneum instead of a standard pressure with mixed results.7–11 Irrigation of the peritoneal cavity with saline and bicarbonate solutions to remove residual CO2 pockets also showed diverging results.12,13 The pulmonary recruitment maneuver can mechanically remove residual CO2 and reduce pain, but the effects were only observed immediately after the operation and disappeared later. 14 Placement of an intraoperative drain, although advantageous, was found to be associated with adverse clinical outcomes. 15
Intraperitoneal instillation of local anesthetics with adjuvants for postoperative pain reduction was started in the early 1990s during laparoscopic surgery with mixed results. 16 Local anesthesia with ropivacaine was found to be safe and effective in gynecological surgeries as well. 17 It has the added advantage of reducing morphine requirement, and postoperative nausea and vomiting in addition to earlier discharge and activity resumption. 18 But the effectiveness of intraperitoneal anesthesia has not been conclusively proven. 16 This might be due to the inclusion of a more number of patients who are less prone to STP. We identified a high-risk group of patients who are more likely to experience STP and upper abdominal pain in our pilot study (unpublished) of 50 cases of laparoscopic surgeries. Twelve patients had STP/upper abdominal pain, and they were young, nulliparous, with low body mass index (BMI) and no previous abdominal surgeries. The cutoff of 30 years was chosen empirically, because these women tend to have less previous exposure to any peritoneal insults. The lax abdomen of parous women is less likely to cause diaphragmatic stretching leading to STP. Malignancies were also excluded, as they may be associated with peritoneal pathology that can alter study results. No previous studies on postoperative pain management have focused on this specific group of patients. Therefore, this study explores the priori hypothesis that intraperitoneal sub-diaphragmatic instillation of ropivacaine will be efficacious on STP and upper abdominal pain postoperatively. The study also aims at quantifying the amount of analgesic needed and exploring the incidence of postoperative nausea and vomiting among the two study groups.
Materials and Methods
It was a parallel-arm randomized controlled trial conducted in a private tertiary care center in Kerala, India. The study duration extended between October 2017 and January 2020. The patient recruitment was initiated after getting approval from institutional ethical committee. The study population were women undergoing fertility-preserving laparoscopic surgeries at the institute, such as laparoscopic myomectomy, ovarian cystectomy, conservative surgeries, adnexectomy, and adhesiolysis. Women eligible for inclusion were those <30 years of age, nulliparous and undergoing abdominal surgery for the first time. Individuals with a known history of hypersensitivity to ropivacaine or malignancies were excluded.
Sample size and sampling
As no similar studies were matching our setting, we used the findings from a study by Pappas-Gogos et al. for the sample size estimation. 19 The mean (standard deviation [SD]) pain scores at 12 hours post-surgery in the intervention and control group were 4.65 (0.81) and 5.3 (1.5). With a power of 80% and an α error of 5%, the sample size was estimated to be 54 in each group. The sample size was calculated by using OpenEpi Version 3.01. 20 Since we adopted coin-tossing randomization, we had to continue the study up to 118 patients to reach the minimal sample size of 54 in each group. Inclusion and exclusion criteria were applied to all the eligible participants before we arrived at the final 118 individuals.
Study procedure
Informed consent was obtained from all patients before data collection. All patients received premedication with oral diazepam 10 mg and omeprazole 20 mg with domperidone 10 mg. General anesthesia was used for all the cases. Anesthesia was induced by using 2 mg/kg intravenous (IV) propofol and after endotracheal intubation, maintained with IV vecuronium 4 mg, nitrous oxide, and oxygen. It is supplemented with IV butyrophenone 0.06 mg/kg. Toward the end of the procedure, IV ondansetron 4 mg was given as a prophylactic antiemetic. Muscle relaxation was reversed with IV neostigmine 2.5 mg and IV glycopyrrolate 0.5 mg. The peripheral oxygen saturation (SpO2), electrocardiogram (ECG), non invasive blood pressure (NIBP), and end tidal carbon dioxide (ETCO2) were monitored intraoperatively. Pneumoperitoneum was created by using a Veress needle in both groups. The site for the primary port insertion was chosen to be intra-umbilical in pelvic masses <12 weeks in size and 4 cm supraumbilical in cases with masses larger than 12 weeks size. Primary port insertion was done with a 10 mm reusable pyramidal tip trocar. Two ancillary 5-mm trocars lateral to the right and left epigastric vessels and a midline suprapubic trocar were inserted under direct visualization. The abdominal capacity of each patient was noted in the form of a total volume of CO2 gas required to achieve pneumoperitoneum with an intraabdominal pressure of 15 mm Hg.
Randomization was done at the level of the participant by using a simple coin-tossing method at the preoperative room, before shifting the patient to the operation theatre, by the circulating nurse.
Those in the study group (Group A) received intraperitoneal subdiaphragmatic ropivacaine, and those in the control group (Group B) did not receive any medication. Forty milliliters of 0.2% ropivacaine was sprayed under the diaphragm by using a 20 mL syringe. It was injected by using a 30 cm-long laparoscopic injection needle with a tip diameter of 1 mm under direct vision at the beginning of the surgery. Trendelenburg position was given to the patient after the instillation. In both the groups, laparoscopic surgery was performed according to the standard protocol followed in the hospital. 21 At the end of the surgery, the ancillary trocars were removed under vision, and the primary trocar was removed after completely evacuating CO2 by opening the trocar valve. Postoperatively diclofenac 100 mg rectal suppository was inserted prophylactically for all patients. The patients were shifted to the recovery room where the heart rate, blood pressure, oxygen saturation, and pain scores were monitored carefully. As a routine hospital protocol, surgeries were performed in the afternoon, and all patients were given tablet paracetamol 650 mg prophylactically the next morning (14–15 hours postoperatively). None of the patients in this study received opioids as postoperative analgesia.
The postoperative pain was charted by the patients using the visual analogue scale (VAS) on a score of 0 to 10 at 1, 4, 12, and 20 hours. VAS provides a simple technique for measuring subjective experience. It has been established as a valid and reliable technique in a range of clinical and research applications. 22 It is easy to use and score. 23 In the VAS, a score of 0 meant no pain and 10 denoted excruciating pain. Those patients with mild pain (Score 1–3) were not administered any analgesics. Those with more severe pain were given analgesics in the postoperative recovery room in addition to the routine analgesia as described earlier. Injection diclofenac 75 mg intramuscular or injection paracetamol 1 gm IV for patients complaining of severe pain (scores ≥7) was administered. Tablet paracetamol 650 mg was given to patients with moderate pain (Score 4–6) after starting oral intake. The onset and dose of rescue analgesia were recorded. Also, the associated nausea and vomiting was evaluated for all patients. Patients were considered to have completed the study if the VAS questionnaire was returned. All eligible cases were included for statistical analysis.
As a hospital protocol, all the patients were discharged on the first postoperative day (≈20 hours postoperatively), if they were hemodynamically stable and free of symptoms such as pain, shortness of breath, fever, or bleeding per vagina.
Data entry and analysis
Data entry was done in Microsoft Office Excel 2016, and statistical analysis was done by using STATA version 12.0. Age, BMI, duration of surgery, abdominal capacity, and pain scores at various time points were treated as continuous variables and were summarized as mean (SD) or median (interquartile range) depending on the distribution of the data. Categorical variables such as parity, type of surgery, presence of drain, port closure, self-reporting of STP or upper abdominal pain, and analgesic need were summarized as proportions.
At various time points, pain scores were compared between the groups by using the Mann–Whitney U test. Association of presence of STP or upper abdominal pain and need for analgesic with intervention at various time points were assessed by using the Chi-square test. A multilevel generalized linear modeling was attempted to calculate the incidence rate ratios (IRRs) of pain adjusted for clustering at the participant level. IRRs were also adjusted for possible confounding by other independent variables.
Results
Characteristics of the study population
Out of 126 eligible patients, 8 were excluded, and the remaining 118 were randomized into two groups. We did not have any post-randomization exclusions (Fig. 1). The mean (SD) age and BMI of the study population were 25.7 (5.4) years and 23.4 (3.8) kg/m2. The study groups were comparable in terms of sociodemographic and other surgical variables. Majority of the women in the study groups had not conceived earlier (98.1% in the intervention arm vs. 95.3% in the control arm). One woman in the intervention arm and three in the control arm had a history of a previous abortion. There were no significant differences between the two groups in terms of method of peritoneal entry, number of laparoscopic ports, type of uterine manipulator, and choice of energy source. Sociodemographic and disease characteristics of the study population compared across the two groups are summarized in Table 1.

CONSORT 2010 diagram showing the flow of patients in the study.
Sociodemographic and Disease Characteristics Compared Across the Two Study Groups for the Study Population (N = 118)
Independent Student's t-test.
Chi-square test.
Mann–Whitney U test.
BMI, body mass index; IQR, interquartile range; SD, standard deviation.
Pain scores and STP
Pain scores at various time points were not found to be significantly different between the groups. Figure 2 graphically brings out the distribution of pain scores across the two groups at various time points.
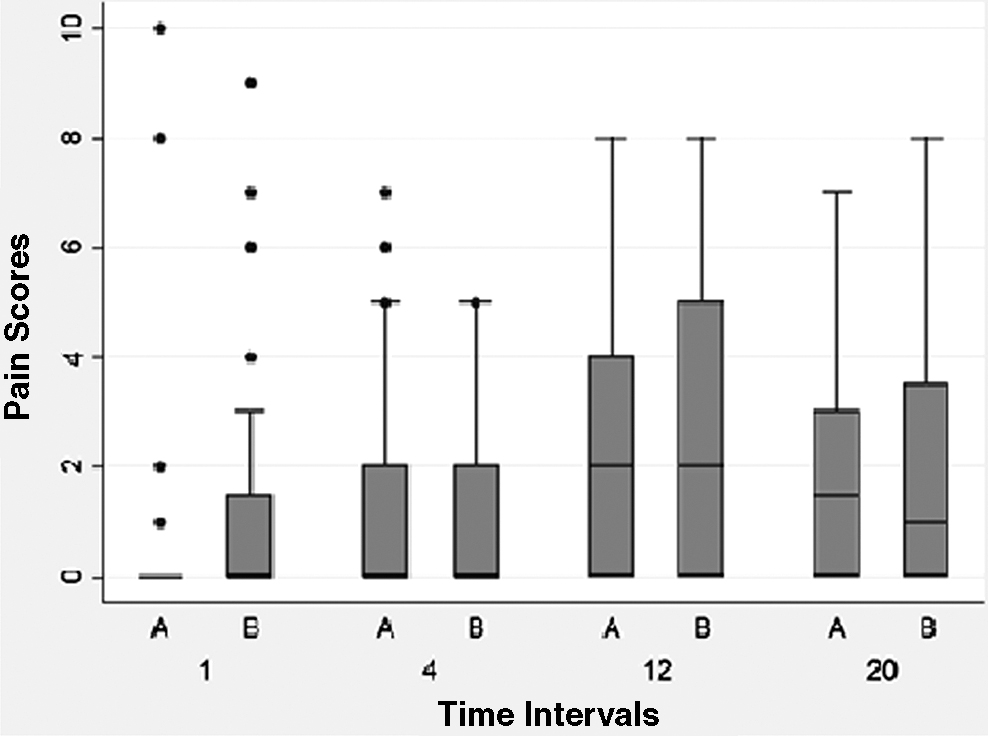
Box and whisker plot of the pain score at the four different time points in the study compared between the two study groups. Group A: intervention and Group B: control, for the study population (N = 118).
We observed that 35 (65%) individuals in the intervention arm and 43 (67%) individuals in the control arm self-reported pain at the end of 12 hours post-surgery and 33 (61%) individuals in the intervention arm and 35 (55%) individuals in the control arm self-reported pain at the end of 20 hours post-surgery. Among these individuals, the incidence of STP or upper abdominal pain was significantly higher in the control arm at 12 hours (Intervention arm: 7.4% vs. Control arm: 21.9%; p = 0.039) and at 20 hours (Intervention arm: 3.7% vs. Control arm: 17.2%; p = 0.035) post-surgery. Other pain locations reported were generalized abdominal and port site pain, which were not found to be significantly different between the groups at any of the study points (Table 2).
Clinical Outcomes at Various Time Frames Postsurgery Compared Across the Two Study Groups for the Study Population (N = 118)
Bold values are statistically significant.
Mann–Whitney U test comparing the median scores at each time point between the two study groups.
Chi-square test comparing the proportions at each time point between the two study groups.
The study observed nausea and vomiting among its participants at various time points and found out that individuals in the control arm developed it first. At 12 hours post-surgery, one (1.8%) in the intervention arm and 5 (7.8%) in the control arm developed nausea. Similarly, one (1.8%) in the intervention arm and 2 (3.1%) in the control arm developed vomiting at the end of 12 hours. Comparison of these difference between the groups was found to be insignificant. Control arm participants demanded more analgesia when compared with the intervention arm participants. They received paracetamol/diclofenac as mentioned in the methodology. However, these differences were not found to be statistically significant. Outcomes across the two groups among the study participants are tabulated in Table 2.
Taking the incidence of STP in the control arm as 21.88% and that in the intervention arm as 7.4%, the number needed to treat (NNT) was calculated as 6.9.
Results of multilevel regression modeling
The null model keeping only the outcome variable showed a 55% (95% confidence interval [CI]: 32.2%–76.4%) clustering at the participant level. Cluster adjusted univariate model showed a significant association between two-time points—12 hours (unadjusted IRR: 9; p = 0.003) and 20 hours (unadjusted IRR: 6.5; p = 0.014) with the incidence of STP (Table 3). Individuals who received the intervention were found to be at a lower risk of development of pain in the defined time interval (unadjusted IRR: 0.27; p = 0.008). The type of surgery was not significantly associated with the onset of pain.
Unadjusted and Adjusted Incidence Rate Ratios of Shoulder Tip Pain, Calculated for the Study Population After Adjusting for Patient and Time Clustering Using the MEGLM Modeling (N = 118)
Bold values are statistically significant.
Only the final model with the lowest akaike information criterion and likelihood ratio in the multilevel Poisson regression is presented under the adjusted prevalence ratio column.
CI, confidence interval; IRR, incidence rate ratio.
The final model revealed that time and intervention contributed significantly to the incidence of pain. An individual in the intervention arm was found to be 75% more protected from the incidence of pain after adjusting for time and individual-level clustering (adjusted IRR: 0.25, 95% CI: 0.10–0.68, p = 0.006) than the control arm. We also learned that the incidence rate of pain varied with the time post-surgery and was maximum at 12 hours post-surgery (adjusted IRR: 9, 95% CI: 2.09–38.79, p = 0.003). The risk for pain decreased thereafter (adjusted IRR at 20 hours: 6.5, 95% CI: 1.47–28.80, p = 0.014).
Discussion
This prospective randomized controlled trial evaluated the use of intraperitoneal subdiaphragmatic instillation of ropivacaine for reduction of postoperative STP or upper abdominal pain in the first 20 hours after fertility-preserving laparoscopic surgeries. All previous studies evaluating the effect of intraperitoneal local anesthesia on the reduction of postoperative STP or upper abdominal pain have included all types of patients. However, the focus of the current study was only young, nulliparous women who have not undergone any previous abdominal surgery, which was identified as a high-risk group in a pilot study conducted by the authors.
Our results showed a significantly lower incidence of STP or upper abdominal pain in the ropivacaine group as compared with the patients without ropivacaine instillation. The previous studies on the topic have showcased conflicting results. Kandil and El Hefnawy 6 and Niknam et al. 24 have found no significant difference across the groups, whereas Ingelmo et al. 25 have reported a significant decrease in the incidence of STP. NNT was calculated as 6.9 in our study, which signifies ∼7 extra patients need to be treated with ropivacaine to prevent the incidence of STP or upper abdominal pain.
As far as the pain scores are concerned, there was no significant reduction in the mean STP or upper abdominal pain scores, thus showing no effect on the severity of the pain. This may be due to the small quantity of ropivacaine instilled and due to the fluid shifting from the subdiaphragmatic space to the lower abdomen after reversal of Trendelenburg position, thus showing an all or none effect. This was in accordance with the findings by Lepner et al. 26 and Joris et al., 27 where no difference was found in the severity of shoulder pain.
Cochrane review by Kaloo et al. showed a low to moderate evidence that there was no difference in the incidence or severity of STP after subdiaphragmatic instillation of a local anaesthetic. 16 However, a meta-analysis by Choi et al. showed beneficial effects on postoperative abdominal, visceral, and shoulder pain scores, thus showing reduced severity. 28
Most previous studies show a difference in findings based on the time of pain score assessment. Pain scores were not different at the primary end-point of 6 hours, whereas McDermott et al. recorded a difference at 10 and 30 minutes post-surgery. 29 Similarly, Bisgaard et al. noted a difference in overall pain to up to 2 hours, after which the scores were comparable with the control group. 30 Overall mean postoperative shoulder pain scores reported by our patients on VAS were highest in the 12th hour after surgery. Similar to our study, Phelps et al. found in their study that STP peaked at around 12 hours postoperatively. 31 A meta-analysis by Sao et al. showed that patients treated with intraperitoneal local anesthesia have a statistically significant reduction of STP scores within the first 6 hours but not after 24 hours. 32 In our study, patients were operated in the afternoon, and they were mobilized the next morning, which is ∼12 hours post-surgery when they complained of maximum STP or upper abdominal pain. This timing of onset of STP or upper abdominal pain after mobilization can be explained by assuming that a more upright position allows residual CO2 to collect under the diaphragm and by the theory of loss of suction support of liver and stretching of ligaments causing pain. 5
Certain other studies have looked at any difference in the timing of administration and concluded that pre-emptive anesthesia with ropivacaine before the creation of pneumoperitoneum has a significantly better effect than administration after surgery.33,34 We administered the local anesthetic after the creation of pneumoperitoneum but not at the end of surgery like suggested by Karaaslan et al. 35
In our study, we did not find a significant difference in requirement of analgesia between the two groups. Use of ropivacaine did not affect the required doses of analgesics, neither oral nor injectables. The overall analgesic requirement in our study might have been less due to routine intraoperative use of butyrophenone, administration of rectal diclofenac suppository immediately post-surgery and oral paracetamol on the next morning. The evidence on analgesia use is fairly positive compared with other variables. Multiple studies have shown ropivacaine instillation to decrease the postoperative requirement of analgesia.25,35,36 The Cochrane review by Kaloo et al. also showed an association between subdiaphragmatic local anesthetic and reduced analgesic requirement. 16 The incidence of nausea and vomiting was also found to be similar between the groups, probably due to the reduced quantity of ropivacaine. Also, butyrophenone used during anesthesia is known to provide additional antiemetic action, which might have confounded the results.
The limitations of this study are that the pain scoring is highly subjective, and there may be interpatient variation in perception and threshold of pain. The routine administration of intraoperative butyrophenone resulted in an overall reduction in the number of patients requesting for additional analgesia across both groups, resulting in low numbers, which made comparison impossible. The criteria used for selecting patients were empirical and not established ones. Limiting participants to the particular age group and parity makes it not possible to generalize the findings to the general population. Also, instillation of intraperitoneal ropivacaine could have hydrated the diaphragm and avoided peritoneal drying, which can be a cause of STP and upper abdominal pain. The clinical utility of this study in terms of the difference in pain scores and the analgesic requirement is limited.
The strength of our study was that our technique of instillation of local anesthetics is simple and easy to replicate for all surgeons.
The STP or upper abdominal pain is one of the distressing symptoms of laparoscopic surgeries. Our study demonstrated a significant reduction in the incidence of STP but not the severity of pain or requirement of analgesics. Future studies with a larger study population and with a placebo control arm are required to prove its clinical utility.
Conclusion
Intraperitoneal subdiaphragmatic instillation of ropivacaine in fertility-preserving laparoscopic surgeries among high-risk patients reduces the incidence of postoperative STP or upper abdominal pain.
Declaration of Patient Consent
Written informed consent was obtained from the patients for publication of the original article.
Ethics Committee Approval
The study “Intraperitoneal subdiaphragmatic Ropivacaine instillation for prevention of STP after laparoscopic surgery in high risk patients: A Randomized Controlled Trial” was approved by the institutional ethical committee. Date: September 30, 2017. No.: IEC-PH-2017-GYN-001.
Footnotes
Author Disclosure Statement
The article has been read and approved by all the authors, the requirements for authorship as stated in the guidelines have been met, and each author believes that the article represents honest work. The authors declare that they have no conflict of interest.
Funding Information
No external funding was received for this article from any source.