
Abstract
With reference to our previous article, 1 in which a case of ruptured interstitial ectopic pregnancy was managed by laparotomy and cornual resection with ipsilateral salpingectomy. The diagnosis was confirmed intraoperatively. This case imparted the knowledge and importance of correct and timely diagnosis for optimum outcome.
Few months later, we encountered another case of interstitial tubal ectopic pregnancy, managed by laparoscopic approach with minimal intraoperative blood loss. The aim of this report is to share the steps of laparoscopic cornuostomy in a case of interstitial ectopic pregnancy for optimum outcome.
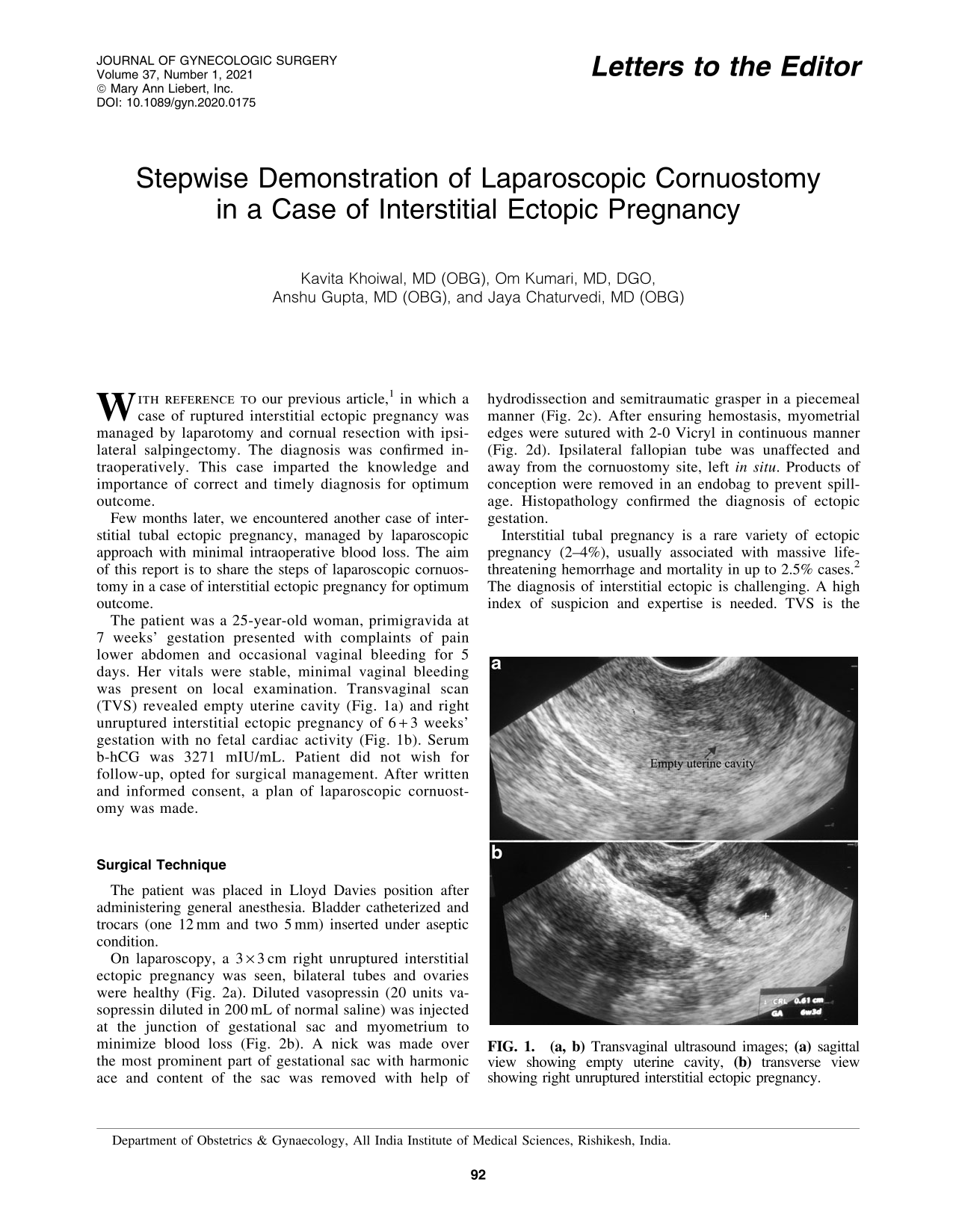
The patient was a 25-year-old woman, primigravida at 7 weeks' gestation presented with complaints of pain lower abdomen and occasional vaginal bleeding for 5 days. Her vitals were stable, minimal vaginal bleeding was present on local examination. Transvaginal scan (TVS) revealed empty uterine cavity (Fig. 1a) and right unruptured interstitial ectopic pregnancy of 6 + 3 weeks' gestation with no fetal cardiac activity (Fig. 1b). Serum b-hCG was 3271 mIU/mL. Patient did not wish for follow-up, opted for surgical management. After written and informed consent, a plan of laparoscopic cornuostomy was made.

Surgical Technique
The patient was placed in Lloyd Davies position after administering general anesthesia. Bladder catheterized and trocars (one 12 mm and two 5 mm) inserted under aseptic condition.
On laparoscopy, a 3 × 3 cm right unruptured interstitial ectopic pregnancy was seen, bilateral tubes and ovaries were healthy (Fig. 2a). Diluted vasopressin (20 units vasopressin diluted in 200 mL of normal saline) was injected at the junction of gestational sac and myometrium to minimize blood loss (Fig. 2b). A nick was made over the most prominent part of gestational sac with harmonic ace and content of the sac was removed with help of hydrodissection and semitraumatic grasper in a piecemeal manner (Fig. 2c). After ensuring hemostasis, myometrial edges were sutured with 2-0 Vicryl in continuous manner (Fig. 2d). Ipsilateral fallopian tube was unaffected and away from the cornuostomy site, left in situ. Products of conception were removed in an endobag to prevent spillage. Histopathology confirmed the diagnosis of ectopic gestation.

Interstitial tubal pregnancy is a rare variety of ectopic pregnancy (2–4%), usually associated with massive life-threatening hemorrhage and mortality in up to 2.5% cases. 2 The diagnosis of interstitial ectopic is challenging. A high index of suspicion and expertise is needed. TVS is the imaging modality of choice. Typical findings on TVS include an empty uterine cavity, a separate gestational sac >1 cm from the most lateral edge of the uterine cavity, and a thin myometrial layer (5 mm) surrounding the gestational sac. 3 Interstitial line sign, thin echogenic line extending directly up to centre of chorionic sac, is another feature on ultrasound (sensitivity 80%; specificity 98%). 4 Accurate and timely diagnosis is pivotal as medical or conservative surgical management can be opted if diagnosed early. Most of the patients underwent cornual resection or even hysterectomy in late gestation. Conventionally, interstitial ectopics have been treated with laparotomy. However, minimally invasive approach is now being preferred for past two decades. 5 Gestational age is a major determinant for route of surgery. The chances of laparotomy are more at advanced gestation whereas laparoscopic approach is more feasible at early gestation. 6
To emphasis, laparoscopic cornuostomy is a safe and effective technique in hands of expertise. A high index of suspicion, early diagnosis, and use of intramyometrial instillation of vasopressin may obviate massive hemorrhage and need of cornual resection or hysterectomy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.