
Abstract
Objective:
The present prospective randomized study compared the effects of a minimal-residue low fiber diet for 3 days preoperatively with fasting alone on surgical vision and efficiency during laparoscopic hysterectomy and myomectomy, as well as patient outcomes after these procedures were completed.
Materials and Methods:
The present study included 281 patients who underwent surgery between April 2012 and June 2015. Prior to surgery, the patients were assigned to 1 of 2 groups: (1) a fasting-alone group or (2) a minimal-residue diet group. The primary outcome was the visual quality of the surgical field.
Results:
Overall exposure of the surgical field was evaluated as “good” or “excellent” in 100 of 139 (71.9%) patients of the fasting-alone group and in 108 of 142 (76.0%) patients of the minimal-residue diet group, which was not statistically significant (p = 0.79).
Conclusions:
A preoperative minimal-residual diet does not improve the quality of surgical vision, compared to fasting alone. Accordingly, it may be reported that fasting alone is a safe and preferable alternative with no added complications in minimally invasive gynecologic surgery, such as laparoscopic hysterectomy and myomectomy. (J GYNECOL SURG 37:485)
Introduction
Superiority of surgical vision could be the most important advantage of minimally invasive surgery. However, the narrow and small size of the pelvis, compared to the abdomen, provides a limited working area, which makes minimally invasive gynecologic surgery difficult. In addition, when the small intestine and a bulging rectosigmoid colon fill the pelvis, surgical vision is blocked and visual superiority is lost; surgery then becomes prone to complications.
According to the latest guidelines and reviews, preoperative mechanical bowel preparation does not improve surgical vision and patient outcomes in minimally invasive gynecologic procedures; therefore, attention has turned to low-fiber diets.1–3 Diet plays an important role in bowel function. A high-fiber diet (such as complex carbohydrates, beans, peas, etc.) increases production of hydrogen and other gases. 4 In contrast, a minimal-residue diet seems to leave minimal colonic fecal residue and decreases production of gases entrapped in feces, reduces their mass and weight, and prevents abdominal distension. 5
To the best of the current authors' knowledge, the benefits of a preoperative minimal-residue low-fiber diet prior to advanced minimally invasive gynecologic surgery have not been studied. In this prospective study, the goal was to compare the effects of 3 days of a preoperative minimal-residue diet on surgical vision and efficiency during laparoscopic hysterectomy and myomectomy procedures as well as patient outcomes after these procedures were completed.
Materials and Methods
This prospective, randomized, single-blinded, case-controlled cohort study was conducted between April 2012 and June 2015 at the Gynecology Department of Mediguven Hospital in Salihli, Manisa, Turkey. The study was approved by the hospital's institutional review board. Each woman was informed of the experimental design of the study and provided informed consent to participate. All patients were operated on by the same surgeon, who was experienced in minimally invasive surgery and blinded to the patients' dietary status. The study group comprised a total of 281 patients who underwent minimally invasive surgery. Of the 281 patients, 127 underwent total laparoscopic hysterectomy (TLH) and 154 underwent laparoscopic myomectomy (LM).
Inclusion criteria were women ages 18–80 with benign or premalignant gynecologic indications. Exclusion criteria included known pregnancy or malignancy, severe endometriosis (stages III or IV, according to the classification of the American Society for Reproductive Medicine, 1997), and clinically significant systemic conditions that hinder operations. Patients were grouped according to age, body mass index (BMI), parity, smoking status, history of abdominopelvic surgery, duration of operation, estimated blood loss (EBL), conversion to laparotomy, length of hospital stay, and complications.
An objective visual grading system based on anatomical pelvic landmarks was developed for this study (Table 1). Immediately after each surgery, the surgeon completed a self-administered questionnaire to evaluate the intraoperative quality of vision, assess the ease of intraoperative bowel manipulation, and rate the overall level of difficulty in performing the procedure. Using a 5-point Likert scale (excellent, good, fair, poor, and very bad), the surgeon assessed the quality of vision after initial laparoscopic port placement following placing of the patient in the Trendelenburg position, the quality of small-bowel handling with laparoscopic instruments, the quality of rectosigmoid colon handling with laparoscopic instruments, and the need for additional exposure maneuvers.
Grading System for Assessing Quality of Vision
Grading was performed immediately after Trendelenburg positioning maneuver at an angle of 30° and at anteversion of the uterus via a manipulator.
Patients were randomized by a computer program into 1 of 2 groups upon admittance: (1) a fasting-alone group or (2) a minimal-residue diet group. Patients in the fasting-alone group had a normal diet before surgery. Patients in the minimal-residue diet group were restricted to a low-fiber diet and clear fluids for 3 days before surgery (Table 2), with patients scheduled for morning surgery fasting from midnight and those scheduled for afternoon surgery fasting from 6:00
Minimal-Residue Low-Fiber Diet (Foods and Drinks Allowed)
Laparoscopic surgery was performed under general anesthesia, and no preanesthetic medication was prescribed. The direct trocar insertion technique was used for laparoscopy with a 10-mm port, and 3 additional 5-mm ports were inserted for introduction of the surgical instruments. A Clermont–Ferrand uterine manipulator (Karl Storz, Tuttlingen, Germany) for TLH and a Tintara uterine manipulator (Karl Storz) for LM were used to permit anterolateral uterine movements and organ exposure. All patients were positioned using the Trendelenburg maneuver at an angle of 30°, and intra-abdominal pressure was set to 12 mm Hg in all operations after trocar insertion. If the rectosigmoid colon obstructed the surgical field from the posterior aspect, it was suspended from the epiploic appendixes via suspension sutures to the left upper quadrant of the abdomen. The 5-mm midline trocar was changed to a 10-mm trocar before morcellation if needed. All morcellation procedures were performed laparoscopically using a cold knife, and all specimens were removed through the vagina.
The primary outcome was the overall vision quality of the surgical field after initial laparoscopic port placement. Secondary outcomes included quality of small bowel and rectosigmoid colon handling with laparoscopic instruments, the need for additional exposure techniques, duration of surgery, amount of blood loss, postoperative hospital stay, conversion to laparotomy, and complications. The total time of operation was defined as the time from skin incision to skin closure. Postoperative patient care was the same in both study groups. Before hospital discharge, patients had to tolerate a normal diet, be fully mobile, and be satisfied that they could manage at home. All patients were followed-up regularly on days 10, 42, and 180. Complications encountered during the procedures were classified as vascular injury, urinary-tract injury, intestinal-tract injury, or minor complications.
Statistical analysis was performed using SPSS software (version 16.0, SPSS Inc., Chicago, USA). Continuous parametric variables were expressed as mean (± standard deviation); nonparametric variables were expressed as median and range. Categorical variables were summarized using frequencies and percentages. Data were analyzed using Student's t-test, a Mann–Whitney-U test, a χ 2 test, and a Fisher's exact test. For all statistical analyses, a p-value <0.05 was considered significant.
Results
The flow diagram of this study is shown in Figure 1. During the 3 years of the study, 312 participants were enrolled, and 291 were randomized: 143 to the fasting-alone arm, in which 139 patients completed the study; and 148 to the minimal-residue diet arm, in which 142 patients completed the study. General characteristics of the patients, including age, BMI, and history of abdominopelvic surgery are detailed in Table 3, and no significant differences were noted between the 2 groups.
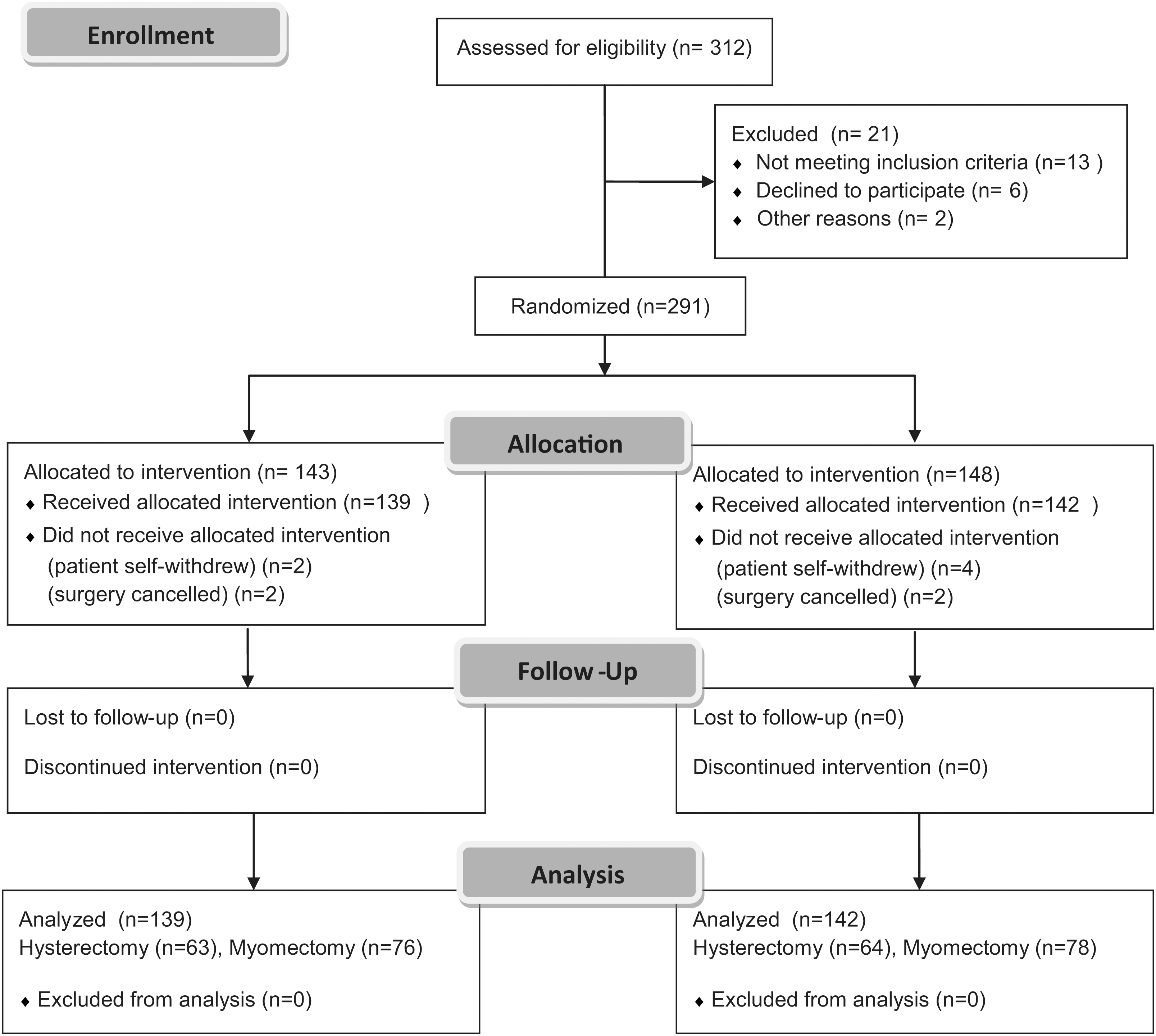
Study flow diagram.
Demographic and Surgical Characteristics of the Patients
Student's t test.
Mann–Whitney-U test.
χ 2 test.
BMI, body mass index; min, minutes, d, days.
Surgical parameters are also given in Table 3. Duration of surgical procedures and EBL were also similar in both groups. No significant difference was observed between the 2 groups with regard to hospital stay, conversion to laparotomy, and complications. Neither small-bowel nor rectosigmoid colon injury occurred during surgery in either group. In 2 cases, conversion to laparotomy was required. One participant from the fasting-alone group required blood transfusion after LM; a second patient required readmission for a ureteral fistula after TLH. One patient from the minimal-residue diet group required transfusion after TLH, a second patient required transfusion after LM, and a third patient in this group required readmission for vaginal vault dehiscence after TLH.
The maximum EBL was 1000 mL in TLH and 1100 mL in LM. Median hospital stay was 24 hours. The overall exposure of the surgical field was evaluated as “good” or “excellent” in 100 of 139 patients of the fasting-alone group and in 108 of 142 patients of the minimal-residue diet group. No statistically significant difference was found between the two groups (p = 0.79). Additionally, there was no significant difference in the quality of small-bowel and rectosigmoid colon handling between the 2 groups. However, the need for additional exposure via suspension suture was significantly more frequent in the fasting-alone group (p < 0.01). No cases required placement of additional ports to improve visualization of the operative field (Table 4).
Evaluation of the Surgical Field
Discussion
With advances in technology over the past 20 years, minimally invasive gynecologic surgery has gained popularity worldwide. As successful surgery relies on adequate vision and exposure, quality of vision has increased in the last decade with high-resolution and 3-dimensional imaging systems. Despite all these technical developments, there are some difficulties in gynecologic operations. The surgical field is restricted due to the narrow structure of the pelvis, together with the small intestines and the bulging rectosigmoid colon that fill the pelvic cavity.
Bowel manipulation during minimally invasive surgery is technically feasible with retractors, sutures, or suspension systems; however, each of these options has its own limitations. Laparoscopic retractors require insertion of extra ports, suspension systems require application of specialized equipment, and suspension suturing requires skill. Yet, the theoretical utility of bowel cleansing before surgery is related to its ability to increase the surgical field and improve the quality of surgical vision. Mechanical bowel preparation (MBP) before elective gynecologic surgery empties the bowel and decreases its caliber; however, several researchers have failed to state the benefit of MBP.6–8 Moreover, MBP is uncomfortable for the patient and exposes the patient to risks of dehydration and electrolyte imbalance.
A minimal-residue low-fiber diet could be an alternative way to decrease the redundancy of bowel caliber. Consumption of a high-fiber diet retards intestinal gas transit by decreasing bolus propulsion to the rectosigmoid colon. Moreover, a high-fiber diet increases gas production by colonic flora. 9 The most important consequence of gaseous retention in minimally invasive surgery is the decreased quality of surgical vision due to a distended bowel. There is no ideal diet for bowel preparation that has been validated yet; however, there is acceptance that the low-fiber diet is defined as a diet with a total daily fiber intake of <10 g.10,11 The recommended minimal-residue low-fiber diet shown in Table 2 was tolerated easily by the patients in this study.
This randomized study compared a preoperative minimal-residue diet with fasting alone in laparoscopic gynecologic surgery for benign conditions, aiming to evaluate the vision quality of the surgical field. The only statistically significant result was the higher rate of need for suspension of the rectosigmoid colon via suspension sutures in the fasting-alone group compared to the minimal-residue diet group. This finding may have been due to gaseous retention in the rectosigmoid colon, which was thought to be less-common in the minimal-residue group due to a low-fiber diet. The quality of vision—which was the primary outcome of the study—and the quality of small-bowel and rectosigmoid colon handling were similar between both groups. Furthermore, all the other evaluated parameters were similar between the 2 groups.
There are no reports comparing a preoperative minimal-residue low-fiber diet with fasting alone during minimally invasive gynecologic surgery in the current literature. Won et al. compared a low-fiber diet and a low fiber-diet + MBP with fasting alone in minimally invasive gynecologic surgery. 8 These researchers concluded that there was no clinical difference in the surgical quality of view and bowel handling between the 3 groups in that study. Moreover, the researchers emphasized that there was more patient discomfort in the MBP and minimal-residue diet groups than in the fasting-alone group. 8
The current study should be carefully considered for advanced gynecologic operations such as deep pelvic endometriosis surgery with bowel resection. Although MBP was found to be unnecessary for enhancing colonic anastomotic integrity and insignificant for the healing process in rat models,12,13 many surgeons would prefer not to leave solid stool directly in the line of bowel anastomosis in minimally invasive surgery. 14
The present study had the following limitations. First, a larger sample size would have yielded more-reliable results. Second, the current authors' grading system, which includes plain objective criteria, has not been tested and validated elsewhere. Future studies evaluating the quality of vision with the inclusion of similar objective criteria would yield valuable observations that might support the present study. Third, the study was designed according to scoring provided by a single surgeon. However, the scoring would certainly have a wider variability if multiple surgeons were involved in a future study. Finally, adverse effects and patient discomfort due to a minimal-residue diet were not assessed. However, the possibility of electrolyte imbalance is not expected with a minimal-residue diet, as opposed to MBP. The current authors' minimal-residue low-fiber diet—which consists of a wide range of food and beverages—was tolerated easily and no patient in the minimal-residue diet group was withdrawn from the study.
Conclusions
A preoperative minimal-residual diet for 3 days did not improve the quality of surgical vision, compared to fasting alone. Accordingly, it may be reported that fasting alone is a safe and preferable alternative with no added complications in minimally invasive gynecologic surgery for benign conditions.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
This research did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sectors.