
Abstract

Subject
Vaginal cuff dehiscence with subsequent evisceration of abdominal content was described as early as 1864 by Hyernaux, 1 according to Croak et al. 2 In modern literature, vaginal cuff dehiscence with evisceration is described as intraperitoneal content prolapsing through a separated incision at the vaginal cuff. 3 Dehiscence is thought to occur in <1% of vaginal cuffs—with laparoscopic/robotic closure having the highest rates and vaginal closure having the lowest rates.3,4 Evisceration of abdominal content is not present with every dehiscence; however, this is a surgical emergency when it is present. Eviscerated bowel content could lead to bowel injury and devastating sequelae, such as incarceration, strangulation, necrosis, perforation, peritonitis, or sepsis.5,6
Review
Because of its rarity, vaginal cuff dehiscence is difficult to study. Risk factors for cuff dehiscence and evisceration include poor wound healing (because of malnutrition, smoking, or infection), prior vaginal surgery, conditions that increase intra-abdominal pressure, coitus, and the presence of an enterocele.2–4 Postmenopausal status can increase the risk of this complication due to a hypoestrogenic state, atrophy, and decreased tissue integrity related to a patient's hormonal status. 3 It is estimated that 67% of cases with dehiscence occur spontaneously. 4 Typically, patients present within 24 hours of experiencing symptoms, such as abdominal or pelvic pain, or vaginal soreness, bleeding, or discharge.2,3 Many patients have seen physicians within a few months prior to the occurrences. 2 Treatment of dehiscence with evisceration involves emergency abdominal or vaginal surgery, with possible bowel resection depending on the degree of bowel involvement and compromise.
While previous reports have described acute presentations of eviscerated abdominal content through dehisced vaginal cuffs as surgical emergencies, this report is unique as this was not an acute presentation. This is the first-known report of eviscerated tissue through a vaginal cuff that was asymptomatic, nonemergent, and incidentally found. The patient gave her consent for publication of this report.
Case
A 45-year-old woman, gravida 2 para 2002, presented 2 years after having a total vaginal hysterectomy, anterior/posterior repair, and needle bladder-neck suspension for pelvic organ prolapse (POP) and stress urinary incontinence. She presented with symptoms of a vaginal bulge and seepage of fluid from her suprapubic incision. On transfer-of-care intake examination, she was noted to have recurrent stage III vaginal vault prolapse with an intact vaginal cuff.
An additional workup was indicated for evaluation of her abdominal-wound seepage. Computed tomography (CT) with intravenous contrast revealed an area of fat descending between the rectum and vagina consistent with POP with an enterocele (Fig. 1A), as well as a suspected vesicocutaneous fistula arising from the right anterior lateral aspect of the urinary bladder and terminating within the adjacent skin surface (Fig. 1B). Given the CT findings, an office cystoscopy was performed showing an intact bladder without evidence of a fistulous opening. The patient was given an oral agent that stains urine blue to investigate if there was a fistulous tract, given the discrepancy between the CT report and the cystoscopic findings. She denied having any blue-stained discharge from the wound, confirming that a fistulous tract was unlikely.
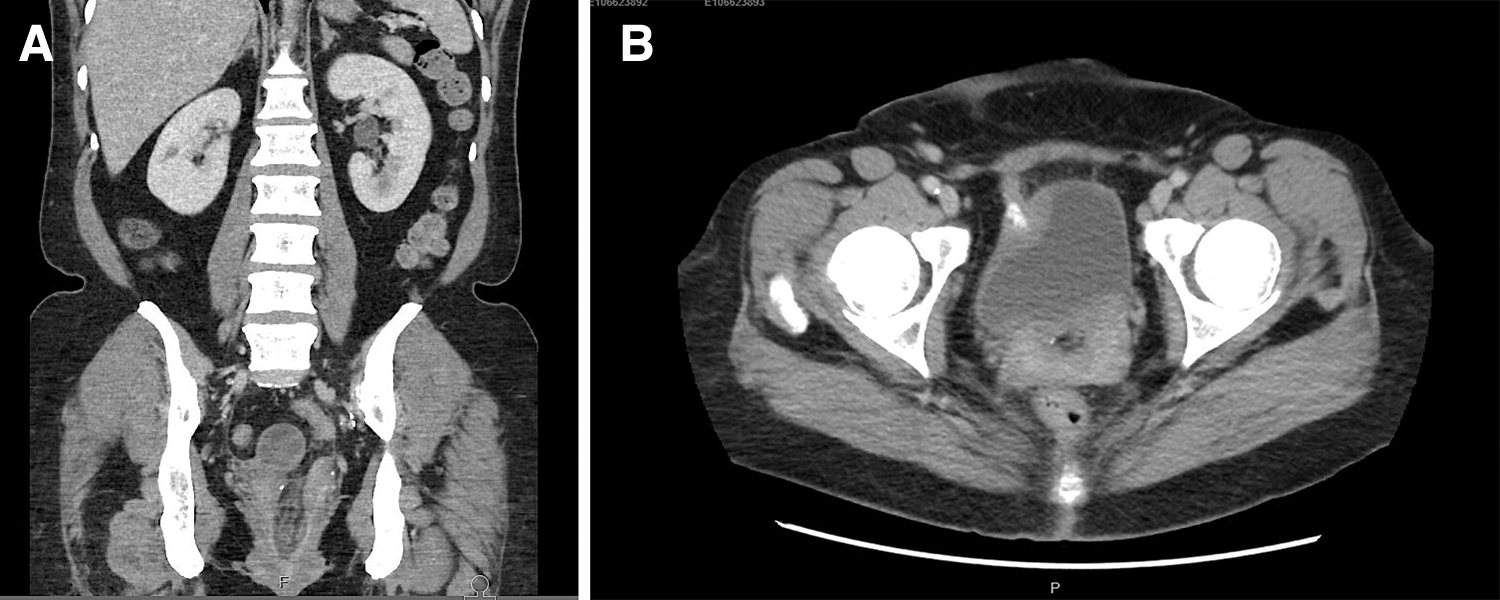
Computed tomography images.
A 2-step operative procedure was planned to: (1) resect the source of the suprapubic drainage and (2) then repair the recurrent prolapse. The procedures were performed in stages due to the tract appearing chronically inflamed and wanting to remove any site of potential infection prior to inserting a new permanent foreign body.
A thin but intact vaginal cuff was confirmed during the suprapubic wound exploration, and what appeared to be a sinus tract was excised (Fig. 2). At her 6-week postoperative appointment, she reported resolution of suprapubic wound drainage and recovered uneventfully. The examination at this time again confirmed an intact vaginal cuff.

Removed sinus tract from superficial wound.
Three months later, she presented for the second procedure, which was a robotic-assisted laparoscopic sacrocolpopexy for repair of her recurrent prolapse. Examination under anesthesia revealed a well-epithelialized dehisced vaginal cuff with evisceration of abdominal content without evidence of infection (Fig. 3). At that time, it was unclear if the prolapsed tissue was a loop of bowel versus other abdominal content. A colorectal surgeon was consulted intraoperatively to determine the source of the eviscerated tissue and to ensure no bowel compromise.

Dehisced vaginal cuff with protruding eviscerated tissue. A yellow urinary catheter is in the urethra. Color images are available online.
Upon laparoscopic insufflation of the abdominal cavity, flatulence was noted to be escaping through the vaginal defect, further confirming that there was vaginal cuff dehiscence. Inspection of the bowel showed a loop of adipose tissue attached to the sigmoid colon in 2 places and prolapsing through the dehisced vaginal cuff. The tissue was divided from the colon with a laparoscopic electrothermal bipolar sealer/divider and removed transvaginally. Pathologic investigation revealed “nodular benign adipose tissue with acute and chronic inflammation.”
The vaginal cuff epithelium was noted to be healthy-appearing, viable and of normal thickness. The cuff was isolated and trimmed to create fresh edges. The edges were reapproximated with figure-of-eight sutures of 0 polyglactin for closure in one layer. Following transvaginal closure of the healthy-appearing vaginal cuff, a decision was made to proceed with the planned sacrocolpopexy with a Y-mesh attached with delayed absorbable sutures.
Results
This patient recovered well postoperatively without any known complications. Two years after her surgeries, she has been sexually active without any issues. She denies any having complaints of gastrointestinal or genitourinary etiology and denies having any symptoms of POP.
Discussion
This is the first-known report of eviscerated tissue through a vaginal cuff that was asymptomatic, nonemergent, and found incidentally. This appears to be a departure from the conventional teaching that vaginal cuff dehiscence with evisceration of bowel content is a surgical emergency.
Discovery of vaginal cuff dehiscence and further evisceration is typically noted in patients presenting with new-onset symptoms. This patient, interestingly, did not report symptoms that suggested cuff dehiscence or warranted an additional work-up. She denied having anything in her vagina (intercourse, toys, or tampons) for at least 2 years prior to her repair surgeries. She denied having any “popping” sensation, abnormal discharge, increased pressure, or pain between her first and second surgeries. The only vaginal spotting she reported having was for a few days after the wound-revision surgery, as was expected.
Interestingly, this patient was examined thoroughly multiple times during the months leading up to the discovery of the dehiscence with evisceration. Moreover, the well-epithelialized vaginal cuff around the site of the defect suggested that the dehiscence occurred at least several weeks prior to the POP-repair surgery. In this case, the prolapsing structure was deceptive in appearance, which was likely due to the chronic inflammation from the evisceration. Notably, in the literature, the distal ileum is cited as the most frequently eviscerated abdominal organ,3,4 although other parts of bowel being eviscerated have been reported. A 1965 report described symptomatic cuff dehiscence with ultimately eviscerated and strangulated appendiceal epiploica. 7
Several risk factors might have predisposed this patient to develop vaginal cuff dehiscence. She is a daily smoker (she reported smoking half of a pack per day for 20 years), likely contributing to weakened epithelium and difficulty with tissue healing. 3 She experienced a wound complication from her initial surgery with needle bladder-neck suspension, which could have also affected her overall tissue wound healing although the cuff itself was not tampered with during the wound revision. Interestingly—and consistent with the surgical findings—the radiologic report documented an area of fat between the rectum and vagina, consistent with the type of eviscerated tissue noted. This could suggest why the eviscerated tissue was colonic epiploica.
Uniquely, this patient was involved in a motor-vehicle accident with trauma to her jaw between the postoperative examination after her wound revision and the salvage prolapse repair surgery. Perhaps the stresses from the accident could have contributed to her thin vaginal cuff dehiscing and the abdominal content protruding. This accident ultimately delayed her scheduled second surgery, potentially allowing time for the dehiscence with evisceration to become chronic in nature.
The patient did have protective factors against vaginal cuff dehiscence with evisceration. Given her age, she likely was not postmenopausal, although tests were not performed to investigate this. She had no other signs or symptoms that could have indicated an autoimmune or connective-tissue disorder work-up, decreasing the likelihood of an innate tissue defect affecting the repair.
Despite the unexpected finding of vaginal cuff dehiscence and abdominal content evisceration during the POP repair, a decision was made to proceed with a robotic-assisted laparoscopic sacrocolpopexy as planned given that there had been no evidence of bowel compromise. Given her recurrent POP, she would likely benefit from the durability of sacrocolpopexy with mesh, compared to native-tissue repair. Understandably, there is a lack of literature on mesh placement during asymptomatic, nonemergent vaginal cuff dehiscence with evisceration. One case report described successful use of mesh to prevent further recurrent vaginal cuff dehiscence with evisceration. 8 Separate from her dehiscence with evisceration, this patient's smoking status could have contributed to her having a higher risk of mesh exposure.
This case illustrates a patient with vaginal cuff dehiscence and asymptomatic chronic abdominal content evisceration without bowel compromise, infectious morbidity, or any additional postoperative complications. A strength of this patient's presentation and management included close interdisciplinary collaboration to identify and repair the defect as soon as possible. A consideration could include performing a pelvic examination specifically following the motor-vehicle accident although this did not seem warranted as she did not report having any pelvic symptoms. Awareness of risk factors for dehiscence and evisceration could lower provider thresholds for performing vaginal examinations despite the absence of suspicious symptoms.
Trainee's Perspective
This case provides further evidence that performing an examination under anesthesia at the start of a gynecologic surgery can reveal additional findings, affecting management. Recently, consent for, and incorporation of, a pelvic examination under anesthesia as part of a procedure has been under scrutiny and discussed in the media. 9 This case is a prime example of why a pelvic examination under anesthesia is a necessary and automatically incorporated step within the ultimate gynecologic surgery being agreed upon and performed. The findings revealed on this first step of the procedure led to intraoperative consultation with a colorectal surgeon to assess bowel integrity for the patient's benefit and safety. While this examination under anesthesia first and foremost benefited the patient, simultaneously, the examination also provided learning opportunities for residents and fellows who were caring for this patient. Palpation of the abnormality at the vaginal cuff initiated the discussion between the house staff and the attending physician regarding this patient's diagnosis and the surgical team's plan of action. This case provided an opportunity for the house staff to be a part of this intraoperative complex decision making.
Another timely topic applicable to this case is the evaluation of patients having annual pelvic examinations. While an annual pelvic examination remains a shared decision between an asymptomatic, nonpregnant patient and her gynecologist, there may be added value in the case of a patient after hysterectomy. 10 This patient was noted to have a thin vaginal cuff on prior examinations, and a dehisced vaginal cuff with eviscerated tissue would have remained undiagnosed without the scheduled second surgery.
Faculty's Perspective
This case certainly presents an unexpected surgical presentation of an atypical vaginal cuff dehiscence and highlights the need for surveillance of the atrophic prolapsed vaginal cuff. Awareness that dehiscence can occur remote from hysterectomy, and without symptoms, should factor into the paradigm for observation of the prolapsed posthysterectomy vaginal cuff.
Footnotes
Acknowledgments
The authors would like to thank the Yale School of Medicine and the Yale New Haven Hospital.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was obtained for the preparation of this case report.