
Abstract
Objective:
The objective of this study was to evaluate the effect of an Enhanced Recovery After Surgery (ERAS) protocol on patient experience after discharge from laparoscopic hysterectomy.
Materials and Methods:
Patients having laparoscopic hysterectomies by high-volume surgeons (>10 hysterectomies per year) at an urban tertiary-care hospital were divided into 2 cohorts: (1) a perioperative ERAS protocol adopted by the institution or (2) standard perioperative care according to the patient's surgeon. At the postoperative visit, each patient completed a validated questionnaire of self-reported recovery scores in domains of daily functional activities
Results:
There were 40 patients in the ERAS group and 44 in the standard perioperative care group, and 100% follow-up through the 2-week postoperative visits. Patients in both groups had similar rates of same-day discharges (88% versus 73%; p = 0.09). Both groups reported similar physical activity scores (1.38 versus 1.33; p = 0.79), days of first bowel movements (2.69 versus 2.71; p = 0.94), and days of opioid use after surgery (3.13 versus 2.64; p = 0.48). ERAS patients had fewer unplanned patient contacts than the standard care group (15% versus 50%; p < 0.01). There were no readmissions. Patients took few opioids, with 90% of all patients using <10 opioid tablets post surgery (5-mg oxycodone equivalents).
Conclusions:
Same-day discharge, patient-reported recovery experience, and opioid requirements did not differ between the ERAS protocol versus standard perioperative care. The ERAS protocol decreased unplanned patient contacts.
Introduction
Enhanced Recovery After Surgery (ERAS) is an evidence-based approach to perioperative care that has been shown to hasten recovery and attenuate the stress response to surgery. 1 ERAS pathways consist of a set of interventions developed through a multidisciplinary approach, including preoperative, intraoperative, and postoperative phases with the goal of reducing postoperative morbidity and improving return to function by maintaining normal physiology.1–4 The basic principles of ERAS include preoperative patient education, avoidance of fasting and bowel preparation, multimodal analgesia, euvolemia, normothermia, nausea/vomiting prevention, opioid minimization, early oral intake, and early mobilization.1–4
While the literature to date supports quality evidence for individual components of the ERAS pathway, there are few data on the effect of an ERAS protocol on patient-reported recovery experience after laparoscopic hysterectomy.4,5 As ERAS protocols were first developed for open colorectal surgery, 1 many ERAS protocols and reviews focus on patients undergoing laparotomy.6–12 Studies looking at the minimally invasive approach in gynecology have previously focused on length of stay and the feasibility of same-day discharge.13–16 While implementation of ERAS protocols has been encouraged in gynecologic surgery, 2 the lack of patient reported outcomes and recovery data impedes the ability to inform patients about expectations for recovery after laparoscopic hysterectomy.
The primary objective of this study was to evaluate the effect of an ERAS protocol on patient-reported outcomes after discharge from laparoscopic hysterectomy. Secondary outcomes included same-day discharge rates, unplanned patient contacts, and analgesic requirements at home.
Materials and Methods
This was an institutional review board (IRB)–approved prospective cohort study comparing patients undergoing laparoscopic hysterectomy by high-volume surgeons at a single institution (Cedars–Sinai, Los Angeles, CA, from August 2018 to May 2019. An ERAS protocol (Appendix Table A1) was implemented after 2 years of collaboration with the nursing, pharmacy, anesthesia, and obstetrics and gynecology departments. The goal was to measure the success of implementation with 2 surgeons and then expand this to the rest of the department if successful. This study began as a test-of-change through the Cedars-Sinai clinical transformation center, which does quality-improvement projects, and was converted into a research study after IRB approval (Cedars-Sinai IRB Pro00054861).
Two surgeons in the minimally invasive gynecologic surgery division of Cedars–Sinai implemented the ERAS protocol in practice, while the remainder of the obstetrics and gynecology department continued their own surgeon-specific “standard” perioperative care. As these minimally invasive gynecologic surgeons are high-volume, the standard perioperative care cohort was chosen from other high-volume surgeons in the department (high volume = > 10 laparoscopic hysterectomies per year). Patients were included consecutively over a 9-month period in both groups immediately after adoption of the ERAS protocol.
For the study, the patients were divided into 2 cohorts: (1) a group undergoing surgery with the ERAS protocol adopted by the institution and (2) a group undergoing standard perioperative care according to each patient's surgeon. Inclusion criteria were planned laparoscopic hysterectomy, high-volume surgeon, and surgeon use of the electronic medical record. Exclusion criteria included emergent surgery, preoperative opioid dependence, conversion to laparotomy, concurrent nonpelvic surgery, concurrent bowel resection, and use of robotic assistance. Robotic use was excluded due to the fact that few of Cedars–Sinai high-volume surgeons were using it at the time.
A power calculation was performed using patient-reported scores of functional status as a primary outcome. It was calculated that, to detect a 20% difference in patient-reported scores with an 80% power and an α of <0.05, it was necessary to have at least 40 patients in each cohort. Statistical analysis was performed with an unpaired t-test and a Mann–Whitney-U test for continuous variables, and a χ 2 test for categorical variables.
To evaluate patient experience, at the postoperative visit, each patient was given a novel composite questionnaire created from 2 validated questionnaires of self-reported recovery scores in domains of daily functional activities. The questionnaires were combined and shortened for patient ease-of-use on their own. The current authors developed this 20-question survey (Fig. 1) modified from the PoRI [Post-Operative Recovery Index] 17 and the PROMIS [Patient-Reported Outcomes Measurement Information System] 18 that covered 4 major domains of functional status: (1) physical activity; (2) bowel habits; (3) appetite and diet; and (4) and pain interference as well as pain medications. The survey was distributed and completed at the initial postoperative visit. The modified survey used a Likert scale of 1–5 to capture the patient's response in which a lower score meant a better functional status.
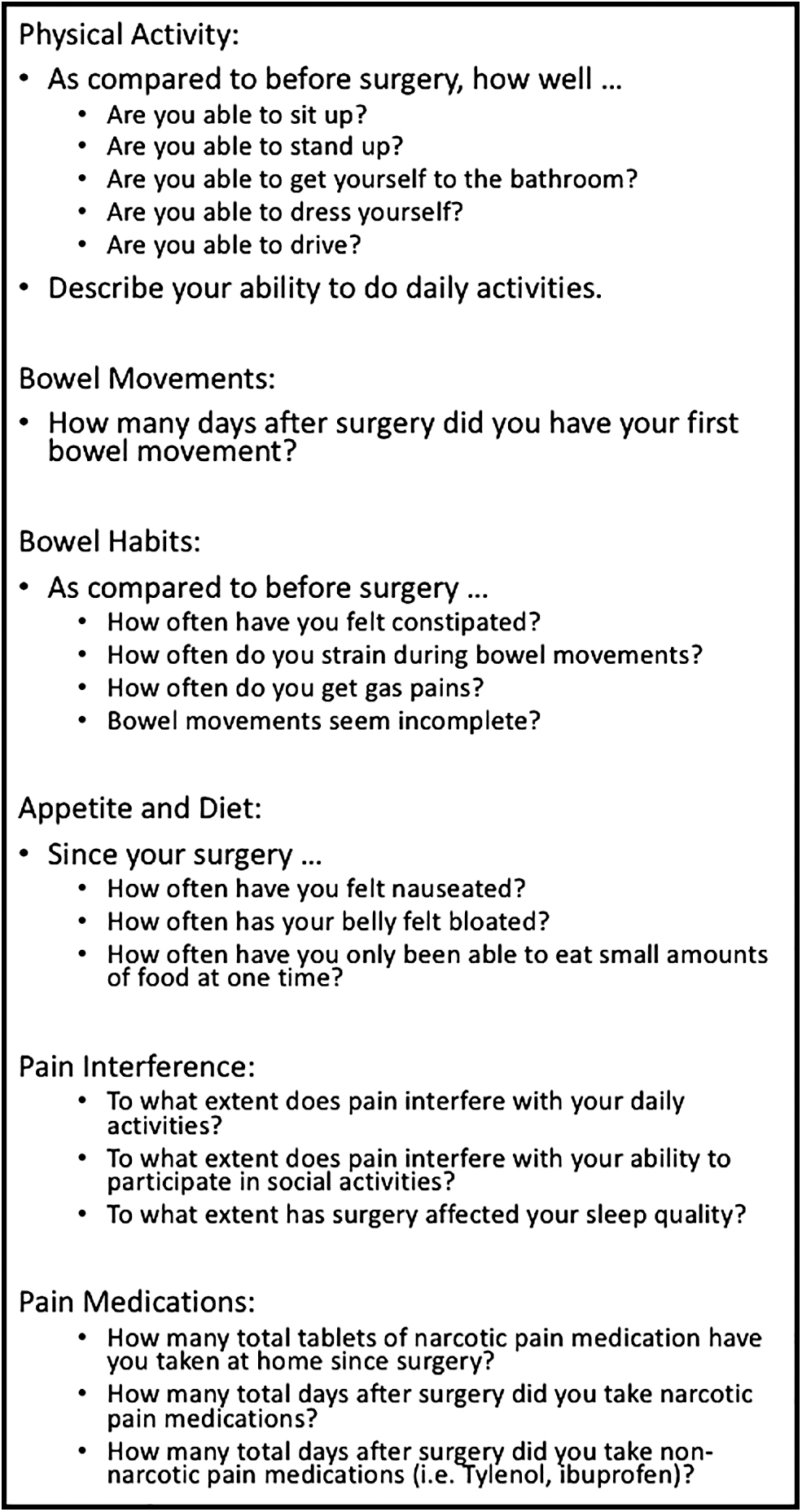
Image of survey given to patients. This postoperative patient survey was modified from 2 existing validated postoperative questionnaires (the Post-Operative Recovery Index and the Patient-Reported Outcomes Measurement Information System) that cover 4 major domains of functional status: (1) physical activity; (2) bowel habits; (3) appetite and diet; and (4) pain interference, as well as analgesic use.
Results
There were 40 (47.6%) women who underwent laparoscopic hysterectomy with an ERAS protocol and 44 (52.4%) women who underwent laparoscopic hysterectomy with standard perioperative care according to each patient's surgeon from August 2018 to May 2019. There was 100% follow-up through the postoperative visit and questionnaire completion, with a median follow-up on postoperative day (POD) 9 for the standard group and POD 13 for the ERAS group. Women in the ERAS group were younger (ages 47 versus 59; p < 0.01) and were more likely to undergo surgery for fibroids with higher uterine weights (405 g versus. 125 g; p < 0.01) and longer operating room (OR) time (172 versus 149 minutes; p = 0.04). Uterine fibroids, abnormal uterine bleeding, endometriosis, nonmalignant neoplasia, and malignancy were the most-common reasons for surgery (Table 1).
Demographics
Mean (standard deviation).
Abnormal uterine bleeding other than fibroids, endometriosis, or nonmalignant neoplasia.
ERAS, Enhanced Recovery After Surgery; BMI, body mass index; EBL, estimated blood loss; OR, operating room; min, minutes.
There was no difference in postanesthesia care unit time (3.75 versus 3.82 hours; p = 0.85), same-day discharge (88 versus 73%; p = 0.09), readmission rates (0 versus 0; p = 0.95), direct costs ($5254 versus $5416; p = 0.62), opioid tablets used (5.36 versus 4.16 oxycodone 5-mg equivalent tablet; p = 0.28), or opioid days used (3.13 versus 2.64 days; p = 0.48) between the ERAS and the standard perioperative care groups (Table 2).
Perioperative Metrics
Mean (standard deviation).
ERAS, Enhanced Recovery After Surgery; PACU, postanesthesia care unit; hrs, hours.
ERAS patients used nonopioids, such as ibuprofen and acetaminophen, for more days (10.05 versus 4.95 days; p < 0.01). Overall, patients took few opioids, with 90% of all patients using <10 opioid tablets after surgery (5-mg oxycodone equivalents; Fig. 2).

Total opioid use at home. Both patient groups used a low number of opioids, with 90% of patients using fewer than the equivalent of 5 tablets of 5-mg oxycodone. ERAS, Enhanced Recovery After Surgery.
There was a statistically significant difference in unplanned patient contacts of 15% in the ERAS group versus 50% in the standard group (p < 0.01), with a contact defined as an unplanned patient portal message, phone call, clinic visit, urgent-care visit, or emergency room visit. Unplanned patient contacts measurements were adjusted for patients with malignancy indications in case this was a potential confounder. Patients without malignancy in the control group (n = 33) still had statistically higher unplanned contacts than patients in the ERAS group (42% versus 15%; p = 0.04). The unplanned patient contacts in both groups were all for clinical concerns, such as pain control, wound care, and constipation. None of the unplanned contacts were for pathology results.
There was no difference in any of the postoperative functional outcomes on the questionnaire including physical activity, PODs until first bowel movement, bowel-habits score, appetite and diet score, and pain interference scores (Table 3).
Postoperative Functional Outcomes
ERAS, Enhanced Recovery After Surgery; SD, standard deviation; POD, postoperative day.
Discussion
Same-day discharge, patient-reported recovery experience, and opioid requirements of patients did not differ between patients in an ERAS protocol versus a standard perioperative care group. However, unplanned patient contacts were significantly lower in the ERAS group. Patients overall reported favorable functional outcomes and low pain interference after laparoscopic hysterectomy whether they were assigned to an ERAS protocol or not. Opioid usage was low across both groups.
The current study findings that patients had fewer unplanned contacts in the ERAS group is in contrast to prior studies 19 showing that unplanned contacts were higher after implementation of an ERAS protocol for minimally invasive hysterectomy. Specifically, the researchers found that unplanned contacts (phone calls, clinic visits, or emergency-room visits) went from 42% before ERAS implementation to 75% after ERAS implementation (p < 0.01). Those researchers recommended further research on ways to minimize unplanned patient encounters. It has been shown previously that patient engagement with preoperative education and setting expectations and goals for postoperative care has been associated with improved outcomes, decreased postoperative complications, superior pain control, and shorter recovery times.20,21
Preoperative patient education and engagement is typically the first step in an ERAS protocol. To enhance patient engagement, the current study's ERAS protocol included a written preoperative patient education packet specific to laparoscopic hysterectomy that set expectations prior to surgery. This packet was given to each patient with instructions to read through it carefully and follow the instructions provided. This extensive education might also explain why ERAS patients took nonopioid pain medication longer than standard-care patients, as they were educated to use alternate nonsteroidal anti-inflammatory medications even if they did not feel acute pain.
Notably, patients in both groups used low amounts of opioid pain medication, which was in line with prior studies22,23 showing that median use of opioids after laparoscopic hysterectomy was 37.5 morphine mg equivalents, which were equivalent to 5 tablets of 5-mg oxycodone. While preoperative medications, such as gabapentin, acetaminophen, and celecoxib, have been reduced total opioid usage in total abdominal hysterectomy, 24 these practices have not been studied adequately with respect to laparoscopic hysterectomy. As patient opioid usage is already low after standard perioperative care in laparoscopic hysterectomy, there might be a floor in which adjuvant perioperative analgesia will not be able to minimize opioid usage further.
Finally, same-day discharge was not statistically different between the 2 groups. Same-day discharge after laparoscopic hysterectomy has been shown to be safe and feasible for more than a decade, has been adopted widely, and is not necessarily dependent on an ERAS protocol.13–16
The biggest strength of this study was its prospective nature; the study was adequately powered to detect a difference in the primary outcome. These patients underwent a uniform procedure by high-volume faculty surgeons at a single institution who function with the same trainees, equipment, and nursing staff in the OR and recovery areas, which removed the heterogeneity that can be associated with care in different locations over different timeframes. This was the first study to explore functional outcomes of patients after discharge, which had not been evaluated up until this point.
A limitation of this study was the differences in the 2 cohorts. Due to the rollout of the ERAS implementation at the institution, it was not feasible to make the groups more uniform while performing a prospective study. Because of this barrier, most ERAS studies to date are either retrospective or compare a current cohort to a historical cohort, which brings in other limitations and heterogeneity to perioperative care. Given that most ERAS components, including the changes in fasting requirements, have been the standard of care for many years, there is no longer equipoise to justify a randomized controlled trial on this topic. Furthermore, standard perioperative care introduces heterogeneity into the non-ERAS cohort because standard care is not protocol-based and generally resides in the mind of the surgeon as the proper management. At Cedars-Sinai, even fasting recommendations and postoperative follow-up differed between standard care surgeons.
While the groups had some differences, they did not nullify all of the conclusions in the study based on the many factors that were controlled for in this prospective cohort. Malignancy was controlled for in case this was a compounding factor for unplanned patient contacts—it was not. All of the unplanned patient contacts were related to clinical matters—none were related to pathology results in either group. Furthermore, as the study was powered to examine differences in patient's functional outcomes, it is unknown if the significant differences seen in patient contacts was a true finding. Previously published reports on unexpected patient encounters 19 examined a similar number of patients retrospectively and after implementation of an ERAS protocol.
Conclusions
These data suggest that patients do well after laparoscopic hysterectomy, and it is uncertain if ERAS elements can improve functional outcomes and reduce opioid requirements further. Additionally, the findings on functional outcomes, first bowel movements, and opioid usage after laparoscopic hysterectomy can guide counseling and prescription habits further for surgeons.
Patient-reported recovery experience and opioid requirements of patients did not differ between patients in an ERAS protocol versus. standard perioperative care, while unplanned patient contacts were significantly decreased with the robust preoperative patient-education packet.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
There was no funding for this study.
Appendix
ERAS Protocol
| Stage of procedure | Anesthesia | Surgeon | Patient |
|---|---|---|---|
| Preoperative | • Celebrex® 200 mg PO once • Acetaminophen 1000 mg PO once • Scopolamine 1.5 mg TD once per anesthesia discretion (age <65) | • ERAS patient-education material given at initial surgical consultation • No mechanical bowel preparation • Prescriptions given prior to day of surgery | • Light meal up to 6 hours before surgery, clear liquids up to 2 hours before surgery |
| Intraoperative | • Warming of patient • Dexamethasone, 4-mg, IV once upon induction of anesthesia • Toradol,® 30-mg, IV once at the end of the case • Goal-directed fluid management • Propofol as main anesthetic agent |
• Wound infiltration with 0.25% bupivacaine with epinephrine prior to incision • No drains • No NGT |
— |
| Postoperative | — | • Scheduled NSAIDs • Narcotics only for breakthrough pain • No PCA • Foley catheter removed immediately with no voiding requirement |
• POD 0 ambulation • POD 0 regular diet • Expectation for discharge same day |
| Discharge | — | • PoRI/PROMIS recovery tool questionnaire |
Celebrex® is the brand name for celecoxib; Toradol® is the brand name for ketorolac.
ERAS, Enhanced Recovery After Surgery; PO, per os (by mouth); TD, transdermal; IV, intravenous; NGT, nasogastric tube; NSAIDS, nonsteroidal anti-inflammatory drugs; PCA, patient-controlled anesthesia; POD, postoperative day, PoRI, Post-Operative Recovery Index; PROMIS, Patient-Reported Outcomes Measurement Information System.