
Abstract
Objective:
The aim of this research was to present and analyze the epidemiologic characteristics, clinical presentations, and treatment approaches to patients with diagnosed adnexal torsions.
Materials and Methods:
This retrospective analysis included 71 patients, each with a confirmed diagnosis of adnexal torsion, who were treated at the University Hospital Dr. Peset, in Valencia, Spain, between 1997 and 2018.
Results:
The patients' average age was 31.56 years (range: 7–760. In the 71 cases analyzed, 7 (9.9%) were pregnant at the moment of the diagnosis; in 44 (62%), the torsion was located on the right side;and in 46 (64.8%), ovarian masses were found. Only 1 (1.41%) of these cases were malignant. Torsion was treated with laparoscopy in 54 (76.1%) of the 71 patients. Conservative surgery was performed in 38(53.5%) of the cases. Adnexal torsion recurrence occurred in 7 (9.9%) patients.
Conclusions:
Adnexal torsion is considered a gynecologic surgical emergency. Diagnosis is challenging and requires a high index of clinical suspicion. Frequently, the diagnosis is performed through surgery. Early surgical intervention helps conserve ovarian function and avoid other complications. Laparoscopic conservative surgery is the chosen surgical approach. (J GYNECOL SURG 37:357)
Introduction
The term ovarian torsion refers to the complete or partial rotation of the ovary on its support elements, which entails a decrease or complete loss of its blood supply. This has the potential to lead to infarction, hemorrhagic necrosis, and gangrene. If a fallopian tube twists along with the ovary, this is known as adnexal torsion. This pathology can affect females of all ages 1 and is considered a surgical emergency that requires a prompt diagnosis to preserve ovarian function and avoid other associated morbidity. However, reaching the diagnosis is frequently challenging because symptoms are relatively nonspecific and can generate confusion with other gynecologic surgical emergencies such as, among others, rupture of an ovarian cyst, a tubo-ovarian abscess, or an ectopic pregnancy.
The incidence of adnexal torsion is not well-known. A systematic review estimated that ovarian torsion represents 2.7% of gynecologic emergencies requiring surgery. 2 In decreasing order of frequency, gynecologic emergencies are: ectopic pregnancy, corpus luteum rupture with hemorrhage, pelvic inflammatory disease (PID), appendicitis, and ovarian torsion. 3 The right ovary appears to be more likely to twist. Some hypotheses suggest that this circumstance can be explained because the right utero-ovarian ligament is longer than the left one and/or that the presence in the left side of the sigmoid colon reduces space availability for the torsion to occur.4,5
The primary risk factor for ovarian torsion is an ovarian mass. In 3 series of patients with ovarian torsion, 86%–95% had ovarian masses.6–8 Hence, although ovarian torsion can occur in females of all ages, it is more likely in women of reproductive age, pregnant women, and women undergoing ovulation induction. The presence of an ovarian physiologic cyst or neoplasm predisposes the patient to have rotation on the axis of the infundibulopelvic and utero-ovarian ligaments. Masses are also more likely to become fixed in a twisted position. The risk of torsion increases as the size of mass increases until it enlarges enough to be fixed in the pelvis. Nevertheless, it is important to remember that ovarian torsion can occur also in nonpathologic ovaries. The most-common symptom of this pathology is pelvic pain, 9 which, as its main feature, starts suddenly and the vast majority of patients seek assistance within the first 3 days since its onset. Moreover, nausea and vomiting are present in most cases.4,5 Despite this typical clinical presentation, symptoms are nonspecific making diagnosis of adnexal torsion complicated. Actually, although analytic and imaging techniques can help achieve a diagnostic hypothesis, ovarian torsion can only be confirmed by surgery.
There are 2 aspects to take into account in the treatment of ovarian torsion. First is the technique by which the surgery is performed: laparoscopic or laparotomy. Second is the concrete procedure to address the torsion: conservative surgery or aggressive surgery. Currently, treatment via laparoscopic surgery is commonly used. The aim of this technique is not only an intraoperative evaluation that allows confirmation of the torsion, but also an appraisal of the viability of the ovary.
It is important to emphasize that most torsed ovaries are potentially viable. An ovary is not considered viable when the adnexa appears necrotic or when it does not return to a viable appearance after being untwisted. Nonetheless, it has been proven that evaluation of adnexal necrosis by surgeons is relatively poor.10,11 When an ovary is viable the treatment of the pathology distinguishes between premenopausal and postmenopausal women and between benign and malignant masses. On the one hand, in premenopausal women with viable ovaries and benign masses, the purpose of the surgery is detorsion and ovary conservation, while performing a cystectomy. On the other hand, premenopausal women with suspected malignant mass or postmenopausal women, should undergo salpingo-oophorectomy to correct the pathology.
Recurrence of adnexal torsion may occur, but the true rate of recurrence is unknown. Surgical techniques—such as plication of the utero-ovarian ligament, suturing the ovary to the pelvic sidewall, or suturing the ovary to the posterior wall of the uterus—have been described. 12 Currently, the preferred timing for oophoropexy—the applicable surgical method and patient prototype—when to apply these surgical techniques is still controversial. 12
The current study presented and analyzed the descriptive epidemiology of patients with adnexal torsion diagnosed and treated, between 1997and 2018, at the University Hospital Dr. Peset in Valencia, Spain.
Materials and Methods
This was an observational, descriptive, and retrospective study to analyze the characteristics and epidemiologic aspects in patients with surgically proven adnexal torsions. The study included all patients who had diagnoses of, and treatments for, adnexal torsion since 1997 until 2018 at the University Hospital Dr. Peset. The analyzed aspects were for each patient: age at the moment of torsion; any previous surgeries; type of torsion; presence or not of adnexal mass; pregnancy when diagnosed, undergoing or not undergoing ovulatory induction; main symptom; consultation, treatment, complications, and recurrences. The analyzed information and the results were obtained with SPSS version 20 and Microsoft Excel 2010.
Results
The 71 women included in the study were diagnosed with, and treated for, adnexal torsion. The average age at diagnosis was 31.56 years (age range: 7–76). The distribution by decades is shown in Figure 1. Among all patients, 7 (9.9%) of were pregnant when they were diagnosed and 3 (4.2%) were in ovulation induction treatment (Table 1). With respect to other prior personal background medical information, only 15 patients (25.4%) had pelvic surgery before: 7 (9.9%) had adnexal surgeries; 5 (7%) had uterine surgery; 5 (7%) had appendix surgery; and 1 had (1.5%) adnexal and appendix surgery (Table 2). The main reason for medical consultations for all patients was acute pelvic pain, and the vast majority were treated in the first 24–72 hours since their pain started.
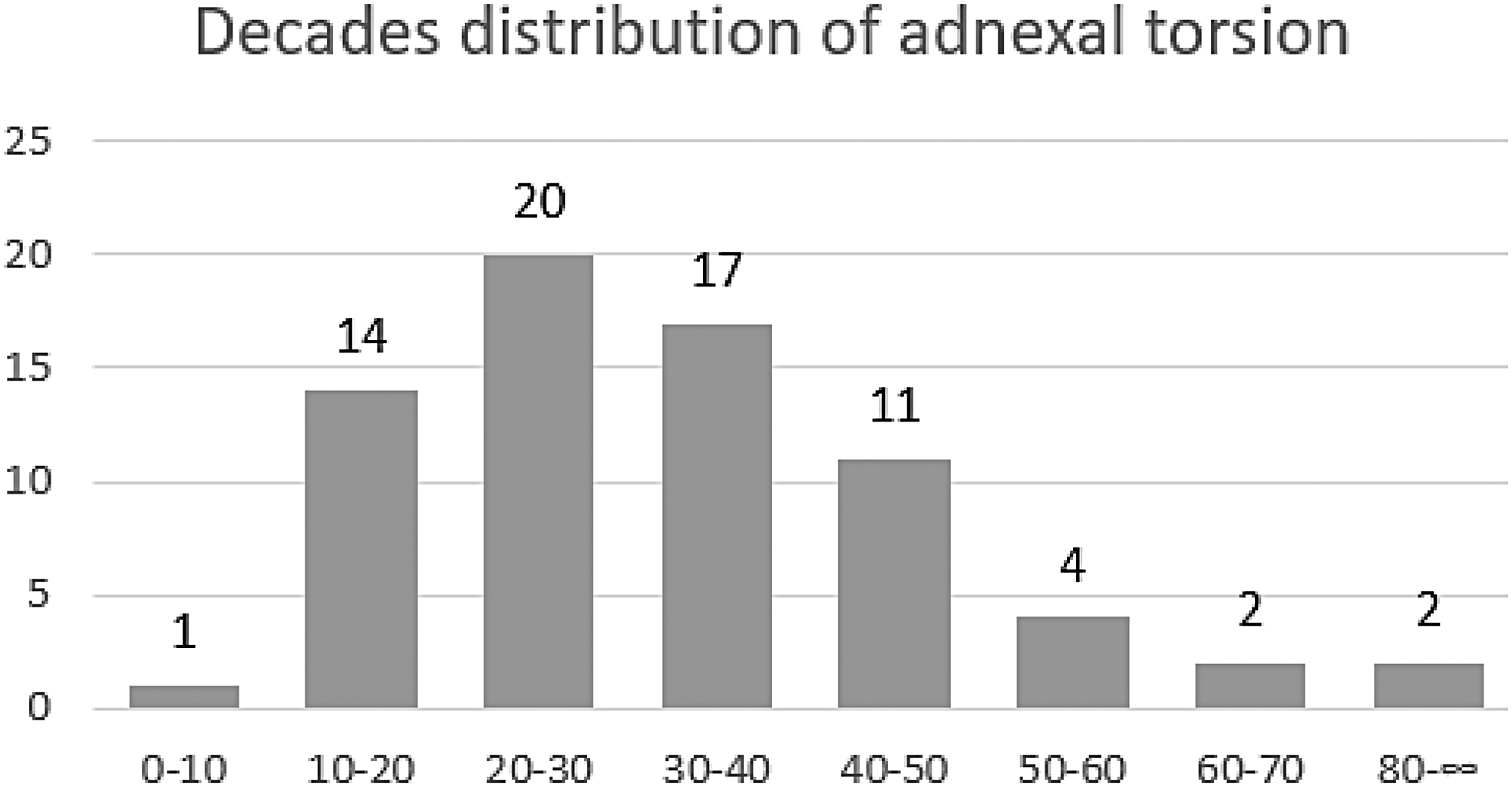
Decades distribution of adnexal torsion.
Clinical Characteristics of the Patients
yrs, years.
Surgical Backgrounds of the Patients
The right ovary was the most frequently twisted one, followed by the left ovary and right adnexal torsion. In the right ovary, right fallopian tube, right adnexa, and right hydatid, right-sided ailments were diagnosed in 44 (62%) patients (Table 3). Among the 71 patients, 46 each (64.8%) showed, concomitantly with the torsion, an ovarian mass. The main type of mass detected was a teratoma; features of other masses are detailed in Table 4. Only 1 (1.41%) of the 71 cases analyzed had a malignant mass. This patient sought medical assistance for abdominal pain and underwent an adnexectomy. The diagnosis was an undifferentiated carcinoma, type C, of the fallopian tube, and required radical ovarian surgery and chemotherapy.
Twisted Elements
Adnexal Masses: Histologic Diagnoses
Laparoscopic surgery was used more often than laparotomy surgery for treatments. In 38 (53.5%) of the 71 cases, conservative surgery was performed consisting of detorsion of the adnexa with or without a cystectomy. The surgical procedures performed are listed in Table 5. Significant complications following surgery affected to 2 (2.8%) of the 71 patients, who had, in both cases, hemoperitoneum. One hemoperitoneum was isolated, and was resolved conservatively, while the other one was associated with thrombosis and pelvic thrombophlebitis and required surgery. Other patients in the study had less-significant complications, such as fewer, anemia, or seromas of the surgical wounds.
Treatment of Adnexal Torsion
Finally, recurrence of adnexal torsion occurred in 7 (9.9%) patients. Five of these patients received their first surgery in the current author's hospital, while the remaining 2 had their first episode of adnexal torsion managed in another hospital. In 4 of these patients, surgical techniques were performed to reduce the risk of recurrence. In all of the cases, preventive surgery was performed following the second episode of adnexal torsion. In the first case a bilateral pexy of the utero-ovarian ligament to the round ligament was performed, using the “hot dog in a bun” technique; the second patient received “hot dog in a bun” unilaterally; in the third case, fixation of the left ovary to the abdominal wall was performed; finally, the fourth patient was treated with a posterior uterine pexy. During a medical follow-up, the patient with fixation to the abdominal wall had a third adnexial torsion noted, requiring an anexectomy. The remaining 3 patients with recurrences did not receive surgery to reduce the risk of recurrence due to ovarian necrosis in the second episode.
Discussion
Adnexal torsion is a serious pathology, and it is considered a gynecologic surgical emergency. The diagnosis is challenging and requires confirmation at the slightest suspicion of its occurrence. A fast diagnosis can allow conservative surgery and avoid severe morbidity in terms of systemic repercussions and problems with fertility.
Adnexal torsion largely affects women of reproductive age. Regardless of the fact this condition can affect women in all age groups, ∼70% of the cases occur in women in reproductive age. 13 In the current study, the average age of diagnosis was 31.6 years (age range: 7–76), which is similar to the reported literature. Furthermore, 52 (73.2%) women were under age 40 and only 8 (11.27%) were over age 50; data that is in line with other studies.7,14,15 Adnexal torsion in pregnant women is estimated to be 12%–18%e of the total cases of torsion7,16 and occurs mainly in the first trimester. In the current series, 7 (9.86%) of the patients were pregnant when they were diagnosed, which is not different from the data provided by the literature. All pregnant women diagnosed with adnexal torsion were in the first trimester of gestation.
Clinical presentation of adnexal torsion is variable and requires differential diagnosis with regard to ectopic pregnancy, corpus luteum rupture with hemorrhage, PID, and appendicitis. The literature describes a sudden onset of severe pelvic pain as the main symptom. 9 Frequently, it is associated to nausea and vomiting, fever, vaginal bleeding, and leukocytosis. 4 In the current study, 100% of the patients sought medical assistance due to pelvic pain.
The mechanism of torsion occurs typically by rotation of the infundibulopelvic and utero-ovarian ligaments. This process is more likely to happen in the right ovary, because the utero-ovarian ligament seems to be longer than left one and may make ovarian torsion more likely; in addition, the presence in the left side of the sigmoid colon makes torsion more difficult. As cited elsewhere, 4 the current study's data showed that the right side 44 (62%) was dominant in ovarian and adnexal torsion.
It is believed that the principal risk factor in the pathogenesis of adnexal torsion is the presence of an ovarian mass that encourages ligament rotation. In the current study, 54 (64.8%) patients each had an ovarian mass when she was diagnosed, with a teratoma the most-frequent kind of mass present. These results align with a recent study made in pregnant and nonpregnant women in which the principal masses found in the latter group were also teratomas. 17 Furthermore, regarding malignant masses, this case series had an incidence of 2% or less in adnexal torsions.6,18 This percentage reaches 3%–20% in postmenopausal women. 19 In accordance with these data, in the current analysis, only 1(1.41%) of the 71 patients each had a malignant histology, and the rate of malignant masses in postmenopausal women was 1 of 4 (25%).
Adnexal torsion is difficult to diagnose. Clinical suspicion and imaging techniques can facilitate the diagnosis, but a precise diagnosis is provided by surgery. Ii is vital to diagnose as soon as possible, because a delayed diagnosis can lead to serious complications, such as adnexectomy, thrombophlebitis, or peritonitis. Currently, the laparoscopic approach is the “gold standard” for diagnosis and treatment of adnexal torsion. Laparoscopic surgery provides many benefits, including: shorter hospital stays; less morbidity; fewer postoperative complications; and better recovery than laparotomic surgery. 18 In the current series, 54 (76.1%) of the patients underwent laparoscopy, with similar results to those obtained in a series of cases with a similar number of patients. 9
It is important to emphasize that the majority of adnexal torsion cases can be addressed with conservative surgery. Therefore, the approach to treatment of adnexal torsion has changed. A few years ago the standard treatment was adnexectomy, due to fear of thromboembolism. Nevertheless, currently, conservative techniques are the mainstay of treatment. In the current study, 38 (53.2%) of 71 patients had conservative surgery: detorsion with or without cystectomy. This percentage is close to the one indicated in the study just cited above.9. However, this result was far from the result obtained by Tsafrir et al., who had 86.4% of patients undergoing conservative surgery, although that study had fewer cases. 20 Significant complications after surgery affected only to 2 (2.8%) of the 71 patients analyzed, with both having postsurgical hemoperitoneum. Their adnexal torsions had been treated conservatively. It should be noted that one of the patients presented with thrombosis and pelvic thrombophlebitis associated with the hemoperitoneum. This clinical situation showed that, although the risk of embolic events is low with conservative management, there is a possibility of such events occurring.
Recurrence of adnexal torsion can occur in some patients. However, the exact percentage of patients who experience recurrence is not entirely known. In the current series, 7 (9.9%) patients had recurrences of adnexal torsions. In all of these patients, conservative surgery was performed for the first event and the recurrences happened in the same sides. These data resemble the 11% of recurrences described in a different study by Tsafrir et al. 18 Additionally, this is in line with the fact that the risk of recurrence is higher in adnexal torsions treated conservatively and in which the ovaries are normal. 21 Practicing oophoropexy is an alternative to decrease the risk of recurrence. However, there is a lack of consensus on indications for, and approaches of, this technique; hence, it is not universally recommended.
Some researchers consider that fixing the ovary to the pelvic side wall or to the uterus can cause excessive tension and impede correct fallopian tube functioning. In our study one of the 2 patients who underwent this surgical approach experienced a recurrence a few months later and required adnexectomy. Plication of the utero-ovarian ligament is preferred by some researchers, given that it is performed easily and seems to conserve anatomical relationships. To our knowledge there are no published studies comparing long-term results of the different oophoropexy methods and there is no consensus on the preferred method. In the current authors' oophoropexy is performed when a patient has a second recurrence.
Conclusions
Surgical technique is established based on the suspected cause and the experience of the surgeon. Studies comparing different techniques and long-term results are required. It can be affirmed that adnexal torsion is a pathology that every gynecologist has to take into account when women with pelvic pain of recent appearance and acute abdomens seek medical assistance. To defer the diagnosis and treatment of this clinical condition can cause severe consequences. Laparoscopic surgery is the standard method to achieve a definitive diagnosis and treatment. It is mandatory to be as conservative as possible with the surgical procedures applied, to preserve the ovarian function, especially in patients in the reproductive-age group. Addressing recurrences requires further studies.
Footnotes
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
No funding was received for this study.