
Abstract
Objective:
The aim of this systematic review and meta-analysis was to obtain an estimate of the prevalence of occult uterine malignancies of any subtype found at surgery for uterine fibroids.
Methods
: MEDLINE® was searched for peer-reviewed articles about uterine surgeries, including morcellated or nonmorcellated hysterectomies, with occult uterine malignancies. Articles selected had data on occult malignancy found during hysterectomies specifically for uterine fibroids. One author screened and extracted data, and another author resolved study-suitability questions. Search terms included occult malignancy or occult uterine pathology, AND morcellation OR hysterectomy. A Freeman–Tukey double-arcsine transformation was used to compute the weighted pooled estimate of the occult uterine malignancy prevalence and to perform back-transformation on the pooled estimate.
Results:
Of 233 articles, 53 met review criteria; 8 studies with specific data were used for meta-analysis. Of 105,890 patients, 578 had occult uterine malignancies. The pooled prevalence of uterine cancer was 0.17% (95% confidence interval [CI]: 0.00%–0.49%). With substantial heterogeneity across the studies (I2 = 93.94%; Q χ2 [7] = 115.50; p < 0.001), there were pooled prevalences of 0.54% for population-based studies and 0.12% for retrospective case series.
Conclusions:
The prevalence of occult uterine cancer of all subtypes combined found during surgery for fibroids is likely higher than estimates from previous studies that focused exclusively on leiomyosarcomas.
Introduction
Uterine fibroids are the most common benign tumors of the uterus and the most common indication for hysterectomy in the United States. 1 The estimated lifetime risk ranges from 70% to 80%, although only approximately one-third become clinically relevant.2,3
Uterine sarcomas are a rare cancer group that originate from the smooth muscle, or mesenchyme, of the uterus and comprise leiomyosarcoma (LMS), endometrial stromal sarcoma, adenosarcoma, undifferentiated sarcoma, and other rare subtypes. 4 Historically, women with large fibroids required open surgery, which is associated with overall increased morbidity and longer hospital stays.5,6 Laparoscopic electromechanical morcellation techniques were developed for large uteri, and these techniques have allowed hysterectomy through minimally invasive surgery to be performed in up to 150,000 patients annually.7–9
However, controversy over the risk of exposing the peritoneal cavity to an undetected uterine malignancy during morcellation has become a subject of contention among gynecologic surgeons. In 2014, the U.S. Food and Drug Administration issued a warning estimating that 1 in 350 women undergoing surgery for fibroids will have a sarcoma, and 1 in 458 will have an unsuspected LMS. 10 A subsequent meta-analysis by Pritts et al. 11 suggested a much lower prevalence of occult LMS, notably 1 case per 1960 surgeries when including all studies and 1 in 8300 when restricting the search to prospective data only. In another meta-analysis by the Agency for Healthcare Research and Quality (AHRQ), 12 the incidence of undetected LMS was estimated to be between 0 to 13 per 10,000 women undergoing surgery for presumed fibroids.
The primary focus in all these previous studies has been the prevalence of occult LMS lesions or occult sarcomas. However, uterine sarcomas comprise a rare subtype of uterine cancer and are much less prevalent than endometrioid adenocarcinomas. 13 The more-pertinent concern is the occurrence of occult uterine cancer of any subtype found at the time of surgery for presumed fibroids.
The objective of this literature search was to perform an updated systematic review and meta-analysis to estimate the prevalence of occult uterine malignancies, of all subtypes combined, at the time of hysterectomy or myomectomy for uterine fibroids. The prevalence of occult cervical cancer at the time of surgery for uterine fibroids was not assessed, intentionally, because the developments of cervical cancer and uterine cancer occur along completely separate physiologic pathways.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed in this systematic review.
Data sources and search strategy
MEDLINE® was primarily used to access existing literature. The search terms used were occult malignancy or occult uterine pathology, paired with morcellation or hysterectomy. The cutoff date for articles was March 25, 2019. Articles were not restricted based on language.
Study selection
The focus of this meta-analysis was to estimate the prevalence of uterine cancer of any subtype at the time of surgery for uterine fibroids. The search was focused on studies that not only looked at LMS and other uterine sarcomas but also studies that also included the more-common subtypes, specifically endometrioid adenocarcinomas. Inclusion criteria were any peer-reviewed journal articles on hysterectomies involving morcellation or nonmorcellation techniques in the context of occult uterine malignancies. The articles were narrowed down further based on whether they included data on occult malignancy found at the time of hysterectomy, specifically for uterine fibroids. Data that included preoperative malignancies were excluded, due to the review's focus on occult pathologies.
Data extraction
One author (L.J.) performed the screening and data extraction, while another author (D.L.H.) resolved any questions that arose regarding study suitability. Queried studies were exported to RefWorks and then transferred to a Microsoft® Excel® spreadsheet. Duplicates were removed prior to screening titles and abstracts for inclusion criteria.
Data synthesis and statistical analysis
The prevalence of occult uterine malignancies among women undergoing surgery for uterine fibroids and their variances were computed for each of the studies. A Freeman–Tukey double-arcsine transformation was used to compute the weighted pooled estimate and to perform the back-transformation on the pooled estimate. 14 This approach was chosen to account for studies that had zero proportions of prevalence. The scoring method was used to calculate confidence intervals (CIs) in order to provide admissible values that fell within the theoretical range. 15 The method used to estimate the parameters and to assess study heterogeneity was performed using a restricted maximum likelihood (REML) random-effects model of estimates. 16 The variance within and between studies was then used to calculate the variance of the final pooled prevalence.
Assessment of heterogeneity
Study heterogeneity was evaluated using the Q test and the inconsistency index I2. 17 A p-value of 0.05 was used for identifying statistical heterogeneity with the Q test. Forest plots were conducted to display the prevalence in each study, in addition to the combined estimated prevalences with their 95% CIs. Due to the small number of studies, publication bias was not tested, as estimates would not have been reliable for such small samples. Study characteristics, such as study design, that were hypothesized to influence the resulting prevalence, were evaluated using a REML random-effects subgroup analysis. 18 The α level for statistical significance was set at 0.05. Data were managed in IBM SPSS, version 25, and the meta-analysis was conducted in Stata software, version 16 using a metaprop package. 19
Results
The search yielded a total of 233 journal articles, of which 53 met the criteria for a full-text review. Of these, 26 were included in the final systematic review for the overarching study. Of these 26 studies, 8 provided specific data on occult uterine malignancy among women undergoing surgery for uterine fibroids and formed the basis for this meta-analysis (Table 1 and Fig. 1)13,20–26. Among the 8 studies examined, the total number of patients combined was 105,890, and there were 578 total occult uterine malignancies. The study dates across the 8 studies ranged from as early as 2000 to as late as 2015 for a total of 15 years of data combined. The 8 chosen studies were reviewed for credibility utilizing an AXIS [appraisal tool for cross-sectional studies], and the results can be seen in Table 2.
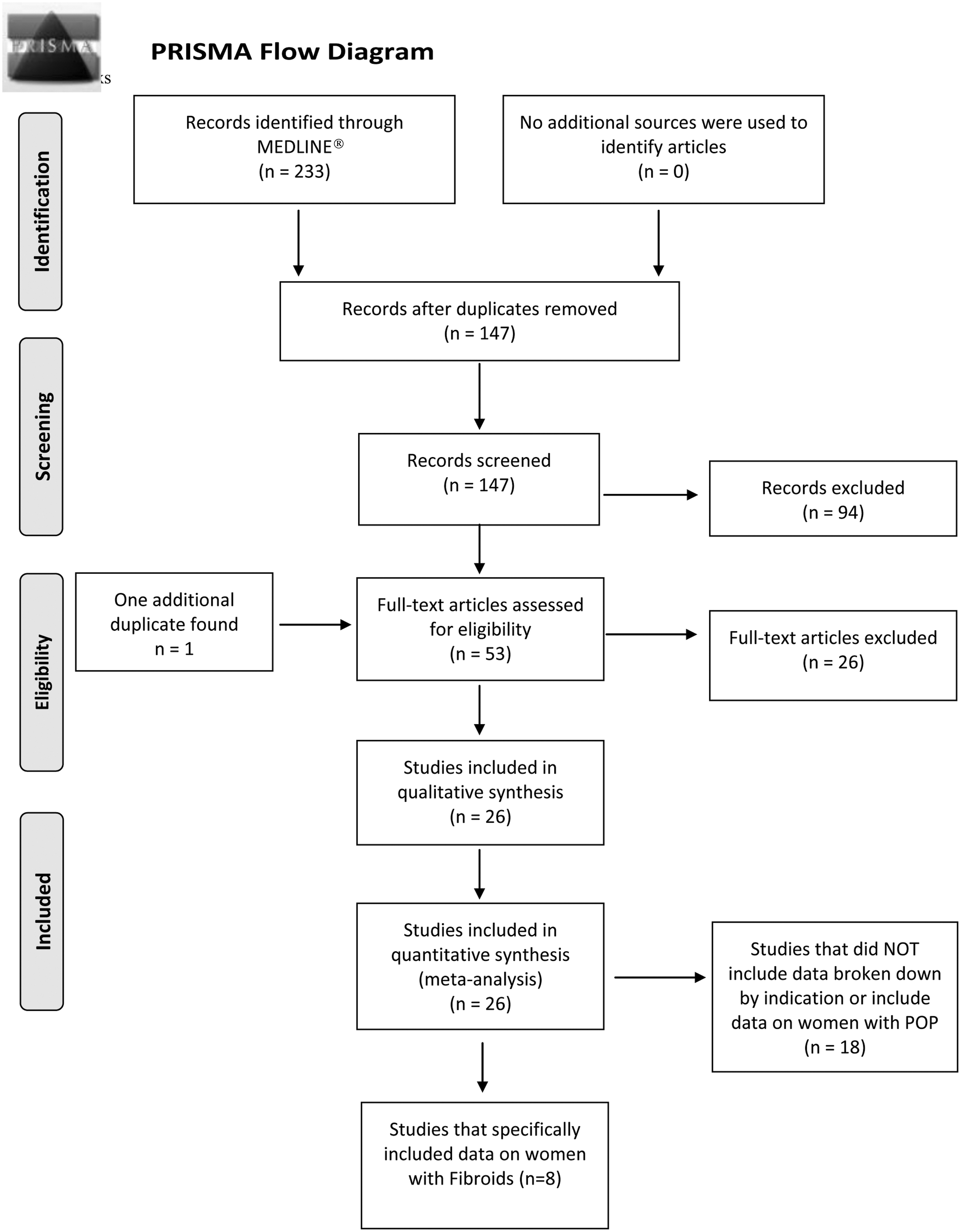
PRISMA [Preferred Reporting Items for Systematic Reviews and Meta-Analyses] study selection flow-chart. POP, pelvic organ prolapse.
Characteristics of the Selected Fibroid Studies
Assessment of Quality of Included Studies (Using AXIS Tool)
AXIS, appraisal tool for cross-sectional studies.
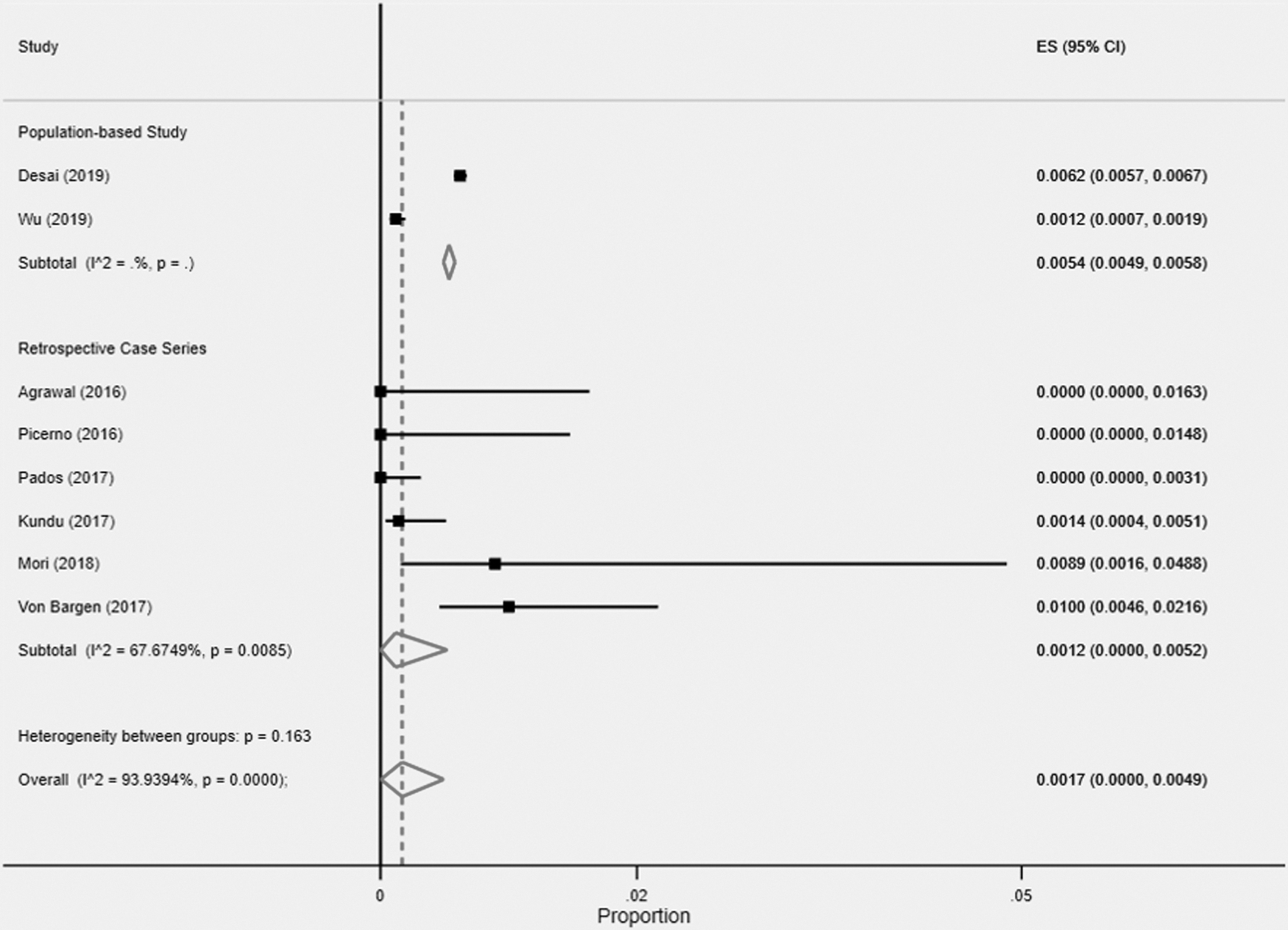
Figure 2 presents the Forest plot of the study-specific proportions with 95% CIs and overall pooled estimates with 95% Wald CIs using the Freeman–Tukey double-arcsine transformation and back-transformation. This approach was pursued due to studies with estimated proportions at 0 being excluded from the analysis, leading to a biased pooled estimate. The findings showed that the pooled prevalence was 0.17% (95% CI: 0.00%–0.49%) for the overall sample. There was substantial heterogeneity noted across the studies (I 2 = 93.94%; Q χ 2 [7] = 115.50; p < 0.001). However, due to the small number of studies, estimates of heterogeneity should be interpreted with caution.

Prevalence of total occult uterine malignancies in fibroid population. ES, effect size; CI, confidence interval.
Figure 3 is the Forest plot of the study-specific proportions with 95% CIs and overall pooled estimates for the subgroup meta-analysis comparing prevalence rates by study design. The 2 types of study designs that characterized these studies were population-based studies and retrospective case–series studies. The findings indicated that the pooled prevalence for the population-based studies was 0.54% (95% CI: 0.49%–0.58%) and for the retrospective case–series studies was 0.12% (95% CI: 0.00%–0.52%). The model indicated that there was not significant between-group heterogeneity (Q χ 2 [1] = 1.95; p = 0.163). Within-group heterogeneity did not estimate for population-based studies, likely due to there being only 2 studies in this subgroup. However, within-group heterogeneity did estimate for retrospective case–series studies, and it did find evidence of heterogeneity across the studies within this subgroup (I 2 = 67.67%; Q χ 2 [5] = 15.47; p = 0.009).
Prevalence of occult uterine malignancies by study design in fibroid population. ES, effect size; CI, confidence interval.
Discussion
The estimated risk of occult uterine cancer has varied in published studies and systematic reviews. In the current meta-analysis of 8 studies, the pooled prevalence of occult uterine cancer of all subtypes was combined to be 0.17% when focusing specifically on patients who underwent surgery for uterine fibroids. These data yielded a pooled prevalence of 0.54% for 2 population-based studies and 0.12% for retrospective case–series studies. The search included all types of surgeries for presumed benign fibroids. Because of significant heterogeneity, this pooled estimate of 0.17% should be interpreted with caution. The current authors believe the pooled estimate of 0.54% obtained from the 2 population-based studies was closer to the true prevalence than the pooled estimate of 0.12% from the 6-case series.
The largest individual study was the study by Desai et al. 13 that examined more than 200,000 women. These researchers found that the overall prevalence of occult uterine malignancy, all subtypes combined, at the time of hysterectomy for any benign indication was 0.96%. When segregated by indication, the prevalence of occult uterine malignancy at the time of hysterectomy specifically for fibroids was 0.62%. Details about the characteristics of each type of occult malignancy after uterine fibroids are in Table 3.
Characteristics of Occult Malignancies After Surgery for Uterine Fibroids
The primary strength of the current review was that a methodologically rigorous meta-analysis of studies that included all uterine malignancies was performed, as opposed to studies that only looked at leiomyosarcomas. This current review is the first meta-analysis to include all uterine malignancies (including endometrioid adenocarcinomas). This study provided a more-realistic picture of the risk of occult uterine cancer at the time of surgery for uterine fibroids. Considering that uterine fibroids are the single most-common indication for women to undergo gynecologic surgery, an accurate estimate of the risk of occult uterine cancer is crucial to preoperative counseling and surgical planning.
There were several limitations of the current review, although an attempt was made to look at occult uterine cancers regardless of subtype, occult cervical cancers at the time of hysterectomy for uterine fibroids were not included. From a statistical perspective the overall group of studies showed significant evidence of heterogeneity and suggested that the overall pooled prevalence (0.17%) may not be an appropriate estimate of the prevalence of occult uterine malignancy in the fibroid population.
As stated above, these stratified results, wherein the pooled estimate was calculated by study design, showed a more-realistic picture. Although the current authors have more confidence in the pooled estimate for population-based studies, there were only 2, and it was not possible to estimate within-group heterogeneity for this subgroup of studies. Retrospective case–series studies showed substantial within-design variances in prevalence rates. However, due to the low number of studies in this analysis, caution should be exercised. More study characteristics may need to be collected in future studies in order to assess the variances in prevalence. In addition, future studies need to include more studies specifically with larger sample sizes to enhance estimates. The search strategy used for this review also did not result in any study with prospective data, and retrospective data may tend to overestimate the prevalence of occult malignancy.11,12
An important point of discussion is the small number of studies in the current systematic review versus others. It is the number of patients and not the number of studies that matter the most in a systematic review. If a systematic review includes hundreds of studies but each study has a very small study population, it is not necessarily superior to a systematic review with a smaller number of studies but in which each study population is significantly larger in size. Although the search strategy yielded a final subgroup of 8 studies reporting data specifically on surgery for uterine fibroids, there was a total of 105,890 patients included in this review.
In the review by Pritts et al., 11 there were 133 studies but only a total of 30,193 women. In the review by the AHRQ, 12 there were 160 studies incorporating 136,195 patients. The current review turned out to be more efficient in terms of the number of studies relative to the number of patients because the search strategy incorporated the most recent study by Desai et al., 13 which is the largest individual population based study to date that attempted to estimate the prevalence of occult uterine malignancy, all subtypes combined, at the time of surgery for benign indications. It was the publication of the Desai et al. study that motivated the current authors to conduct this updated systematic review. This does present a limitation of the study: it was based heavily on the Desai et al. study accounting for a large amount of the systematic review's population and occult malignancies.
One of the central limitations on all attempts to estimate the prevalence of occult uterine malignancy at the time of surgery for benign indications is that there are few very large prospective studies. In the AHRQ review 12 it was noted that the estimates from prospective studies (0.5–2.9 cases of LMS per 10,000 surgeries) were distinctly lower than the estimates from retrospective studies (5.1–8.5 cases of LMS per 10,000 surgeries).
Another important point for discussion is the differential consequences of spreading an undetected uterine sarcoma versus spreading an undetected endometrioid adenocarcinoma (the most-common subtype). A limitation of this current systematic review is that information on preoperative procedures was not available as all studies reviewed simply chose patients based on hysterectomy for benign conditions. One of the key questions in the AHRQ review 12 focused on survival in women with undetected LMS at the time of surgery for fibroids. The study showed no statistical difference in survival based on method of removal, whether it was through morcellation or intact removal. It is unclear what the short- and long-term consequences are for women with undetected endometrioid adenocarcinomas who experience accidental spread via morcellation.
Conclusions
The prevalence of occult uterine malignancy, all subtypes found, at the time of surgery for fibroids is higher than previous estimates based on studies that focused on LMS exclusively. Based on the current stratified analyses, and the CIs in those analyses, the prevalence of occult uterine malignancy, all subtypes combined, at the time of surgery for fibroids could be as high as 58 cases per 10,000 women. Further large and well-designed prospective studies, focused on all types of uterine cancer, are needed to refine and increase the precision of these estimates.
Footnotes
Acknowledgments
The authors wish to thank Ms. Jasmine L. Hankey for her editorial assistance.
Authors' Contributions
Drs. Masghati and Howard conceptualized of the study and participated in writing the article. Mr. James searched in MEDLINE, screened abstracts and full texts, and abstracted data to enable the meta-analysis. Mr. Parks participated significantly writing the article. Dr. Howard participated in the systematic review, and supervised and coordinated the entire statistical analysis.
Author Disclosure Statement
No financial conflicts of interest exist
Funding Information
This study was funded in part by the University of Nevada Las Vegas School of Medicine.