
Abstract
Objective:
To assess the ease of vaginal cuff closure with barbed suture and polyglactin suture in total laparoscopic hysterectomy (TLH).
Design:
A prospective observational study.
Materials and Methods:
All women who underwent TLH for benign conditions from September 2018 to June 2020 were included in the study. Vaginal cuff closure was performed laparoscopically with either unidirectional barbed suture or with polyglactin suture. Time taken for vaginal cuff closure with barbed suture or polyglactin suture was noted during surgery. Vault was examined at the time of discharge and at 6 weeks during which postoperative vaginal cuff complications such as infection, discharge, bleeding, and dehiscence were assessed.
Results:
A total of 120 patients undergoing TLH were included, out of which polyglactin was used in 65 cases and barbed suture in 55 cases. The median time taken for vaginal cuff closure was 16.2 (14–18) minutes in the polyglactin group and 9.5 (8.2–11.4) minutes in the barbed suture group, and the difference was statistically significant (p < 0.001). In the polyglactin group, the incidence of composite vaginal cuff complication was 6.15% compared with 5.45% in the barbed group (p > 0.99). The median duration of hospital stay was 3 (2–3) days in both the groups.
Conclusion:
Barbed suture makes laparoscopic vaginal cuff closure faster without any increase in the rate of postoperative complications. Hence it can be an effective alternative over polyglactin for vaginal cuff closure in TLH.
Introduction
Minimally invasive surgeries have emerged as an alternative to open methods due to their superiority in terms of faster recovery, shorter hospital stay, less blood loss, and lesser morbidity. In January 1988, Harry Reich at Pennsylvania performed the first laparoscopic hysterectomy (LH). 1
In the United States, 43.4% of hysterectomies are performed by laparoscopy, 2 whereas in the United Kingdom, ∼54.4% of hysterectomies are performed by this route. 3 Similar data are not available for India, however, at our institute, ∼50% of hysterectomies are performed laparoscopically. One of the major technical challenges while performing LH lies in vaginal vault closure by intracorporeal suturing that requires good hand–eye co-ordination and dexterity, especially with flat two dimensional visions. Hence it is prudent to devise novel suture materials or devices that minimize the technical difficulty.
Barbed suture is a relatively newer type of suture that does not require knot tying and has been used abundantly by other surgical branches. The presence of barbs on its surface helps in piercing into the tissue and to hold them in place. These can be an attractive alternative over conventional sutures as these create consistent wound tension across the suture line due to its inherent ability to self-anchor to tissues. Moreover, the knotless nature could ease the technical difficulty associated with suturing in laparoscopic procedures. A systemic review and meta-analysis performed by Iavazzo et al. 4 in 2014 (in which three randomized controlled trials [RCTs], nine case series, and four case reports were included) concluded that it takes much less time to close vaginal vault with barbed suture as compared with conventional sutures. However, the evidence is not robust enough due to small number of studies with methodological shortcomings. Only two RCTs have compared these two suture materials for vaginal vault closure after total laparoscopic hysterectomy (TLH) and rest of the published literature is retrospective. We conducted this prospective observational study to assess the ease of vaginal cuff closure using either barbed suture or polyglactin suture and also compared the postoperative vaginal cuff complications.
Materials and Methods
Study protocol was reviewed and approved by Institutional Ethics Committee AIIMS/IEC/2018/656.
Participants and setting
We included all consenting women who underwent TLH for benign conditions from December 2018 to June 2020. Those patients in whom vaginal cuff closure was performed vaginally, those in whom TLH was converted to laparotomy, and where intraoperative visceral injury occurred were excluded from the study.
Outcomes
The primary outcome was the time taken for vaginal cuff closure with barbed suture and polyglactin suture. Secondary outcomes studied were hospital stay and composite postoperative vaginal cuff complications up to 6 weeks after surgery. The postoperative complications assessed included vaginal cuff dehiscence, infections, vaginal granuloma, and bleeding.
Surgical technique
All laparoscopic hysterectomies were performed in a standardized manner by experienced laparoscopic surgeons (each having performed at least 100 laparoscopic procedures). Uniform techniques were used for patient positioning, uterine manipulator placement, peritoneal cavity entry, CO2 insufflation, and laparoscopic port placement. In surgery-naive women, peritoneal entry was done through supraumbilical incision followed by 11–12 mm camera port placement. In women with prior abdominal surgeries, Palmer point was used for primary peritoneal entry. Subsequently, three lateral accessory ports of 5 mm were created in a controlled manner under direct vision. Initial steps of hysterectomy include coagulation and transection of adnexal structures or infundibulopelvic ligaments. After mobilization of bladder flap, skeletonization and desiccation of uterine arteries were completed in the usual manner. Colpotomy was performed with Harmonic® scalpel shears (ETHICON; Johnson & Johnson, USA), taking support over the vaginal colpotomizer ring for defining cervicovaginal junction. Vaginal cuff closure was done with polyglactin (1-0 polyglactin; ETHICON) or unidirectional barbed sutures (V-LOCTM 180: Covidien 30 cm) depending on the surgeon's preference and availability of suture material in the hospital. The suture was folded, held on to laparoscopic needle holder, and introduced into the pelvic cavity through the primary port. All cuff closures were done by intracorporeal suturing from ipsilateral ports. With barbed suture, after the initial bite at one of the angles, the needle traversed the closed loop present at the other end of the thread and tightened. The rest of the suturing was done in a continuous running manner to the other end of the vault and couple of back bites was taken to bury the end of the suture. In both the groups while suturing, needle pierced full thickness of vagina incorporating the vaginal mucosa also. Suturing with polyglactin was done either in a continuous running manner with intracorporeal knot tied at both ends or by applying interrupted stitches after securing angles separately. With both the sutures, uterosacral ligaments were suspended with both the angles. Time taken for vaginal cuff closure was noted in real time. The time of vaginal vault closure was determined starting from the beginning of first stitch till the cutting of last stitch. Demographic details including age, body mass index (BMI), parity, the indication of surgery, associated comorbidities, and history of previous abdominal surgery were obtained.
Follow-Up
Examination of vaginal vault was done on the day of discharge and 6 weeks after surgery to assess the vault for cuff complications such as infection, bleeding, and cuff granuloma.
Based on the suture material used in vaginal cuff closure, these patients were divided into two study groups for comparison of the outcomes. Group one included patients in whom vaginal cuff closure was performed with polyglactin suture, whereas group two consisted of patients in whom vaginal cuff closure was performed with barbed suture.
Data collected were entered in Microsoft Excel sheet. All the analyses were performed by using Statistical Package for Social Sciences (SPSS) software 21. Continuous data were checked for normality of distribution by various methods. Student's t-test was used to analyze normally distributed data and Mann–Whitney U test was used for non-normally distributed continuous data. For categorical variables, chi-square test was used at a two-sided significant level of 0.05 for testing the differences between the two groups. The study was powered to detect 15% difference in the mean.
Results
Between December 2018 and June 2020, a total of 141 laparoscopic hysterectomies were performed. Owing to the COVID-19 pandemic, recruitment of participants was hampered from March to June 2020. After excluding 21 cases, 120 women who satisfied the inclusion criteria were included in the study (Fig. 1). Barbed suture was used in 55 and polyglactin was used in 65 women. Among 65 cases in the polyglactin group, interrupted suturing was used in 21 cases and continuous suturing was done in 44 cases. The rest of the surgical steps were similar in all cases.
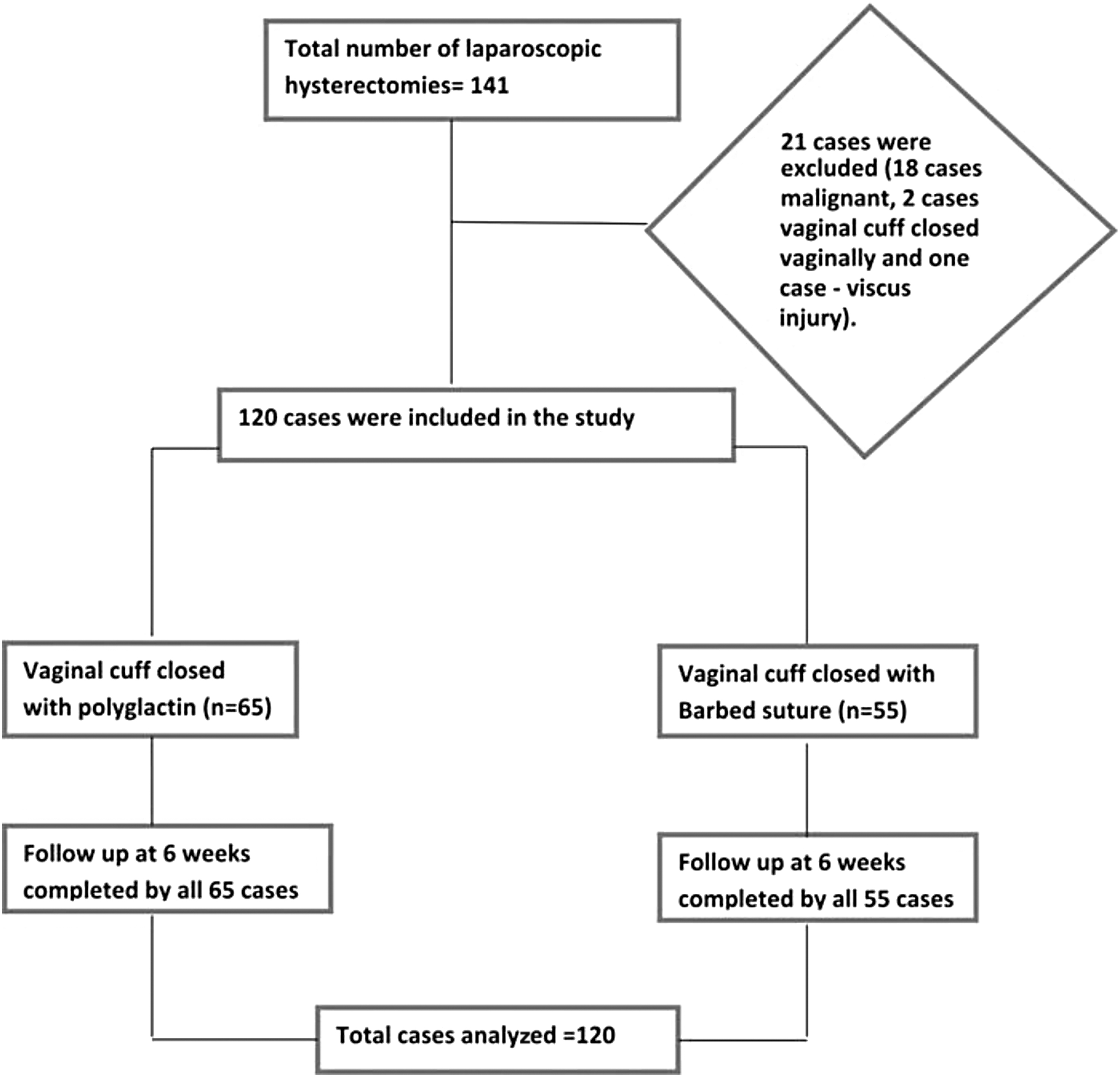
Flow chart of study participants.
Age, BMI, parity, prevalence of comorbidities, and previous surgeries were comparable between the two groups (Table 1). The most common indication for hysterectomy was fibroid uterus in both suture groups: 50.8% in the polyglactin group and 60% in the barbed suture group. Other indications for TLH in both suture groups were also comparable.
Demographic and Other Patient Characteristics
BMI, body mass index; SD, standard deviation.
The median time taken for vaginal cuff closure was 16.2 (14–18) minutes in the polyglactin suture group and 9.5 (8.2–11.4) minutes in the barbed suture group, and the difference was statistically significant (p < 0.001) (Table 2). In the subgroup analysis of the polyglactin group, the median time taken for vault closure with interrupted suturing and continuous suturing group was 15 (7.35–24.0) minutes and 16.2 (8.31–20.15) minutes, respectively, and the difference was not statistically significant (p > 0.99) (Table 2).
Primary and Secondary Outcomes
Median values with interquartile range.
Composite vaginal cuff complication rate was 6.2% with the polyglactin suture group compared with 5.5% in the barbed suture group, and there was no statistically significant difference between the two groups (p > 0.99) (Table 2). There was no case of vaginal vault dehiscence in both suture groups in this study. Two patients (3.6%) in the barbed suture group had postoperative vault infection compared with none in the polyglactin group. Vaginal bleeding was seen in one patient each in both groups. Vaginal cuff granuloma was seen in three cases (4.6%) of the polyglactin group and none in the barbed suture group. The median duration of hospital stay was similar: 3 (2–3) days in both the suture groups.
Discussion
The aim of our study was to assess the ease of vault closure by comparing the time taken for laparoscopic vaginal vault suturing with barbed suture and polyglactin suture. We found that vaginal cuff closure was accomplished in a significantly less time with barbed suture. Similar findings were reported by Boglio et al., 5 Morgan-Ortiz et al., 6 Kim et al., 7 and Khoiwal et al. 8 Einarsson et al. 9 in their RCT found no significant difference in the time taken with either suture material (9.6 ± 4.8 minutes vs. 10.4 ± 5.2 minutes). However, they used Lapra Ty Clips with both types of sutures to secure their ends instead of knotting. In another RCT, Lopez et al. 10 also demonstrated the nonsuperiority of barbed suture over polyglactin. In both of these RCTs, continuous closure of vaginal vault in the polyglactin arm was done, whereas in the index study, interrupted closure was done in one-third of cases of the polyglactin group.
In our study, postoperative vaginal cuff complications were few, which were comparable between the two groups (6.5% in the polyglactin group vs. 5.4% in the barbed suture group). There was no case of vaginal vault dehiscence in this study. Compared with this study, Boglio et al. 5 observed higher incidence of postoperative vaginal bleeding in both groups (15% vs. 10.4% in polyglactin and barbed suture, respectively). Similar observations were made by Kim et al. 7 and Karacan et al., 11 and also Zhou et al. 12 have reported very high composite vaginal cuff complication rates (54.6% in the polyglactin group and 28.6% in the barbed group) and vaginal cuff granuloma between the two groups (polyglactin: 27.3% vs. barbed: 8.2% and p = 0.03). Medina et al. 14 detected higher rate of postoperative vaginal bleeding in the polyglactin group than the barbed suture group (32.5% vs. 18.8%, p = 0.03).
Compared with the published literature, we observed least postoperative vaginal cuff complications in this study that demands possible explanations. We performed colpotomy in all cases with Harmonic scalpel shears (ETHICON, Johnson & Johnson, USA), whereas most studies already mentioned used monopolar hook for colpotomy. Harmonic has the least lateral thermal damage, whereas monopolar current has the maximum lateral thermal spread, and this might have contributed to differences in the postoperative cuff complications. In addition, this study was not adequately powered to detect difference in the postoperative complications and hence the results regarding postoperative complications must be interpreted with caution.
The median duration of hospital stay in our study was 3 (2–3) days in both polyglactin and barbed groups and is in keeping with few other published studies.11–14 The longer hospital stay after LH is not uncommon in Indian setting. Almost all of patients could be discharged a day after the surgery, however, it was delayed as most of our patients hailed from rural and far-flung places with poor access to health care facilities in the vicinity.
Strengths and limitations
The biggest strength is the prospective nature of this study. Most of the previous studies are retrospective in nature where data were collected from chart reviews, medical records, and review of surgery videos in some studies. In this study, all the parameters were recorded in real time and there was no loss of data. However, selection bias cannot be ruled out due to lack of randomization of participants. One might argue that interrupted closure with polyglactin suture inherently takes more time, hence the difference in the primary outcome. However, we did not find any difference in the time taken for vault closure using either continuous or interrupted stitches with polyglactin suture. However, this must be viewed with caution as this study was not powered for a subgroup analysis.
Conclusion
Use of barbed suture significantly reduces the vaginal cuff closure time in LH, whereas the postoperative complication rate was similar between the two groups. It can be safely assumed that barbed suture simplifies the laparoscopic closure of vaginal vault and is as safe as conventional polyglactin suture.
Footnotes
Authors' Contributions
P.S.M. contributed to study design, recruitment, follow-up, data collection, entry of data into software, and writing the article. S.S. carried out study design, statistical analysis, interpretation of results, and writing the article. M.G. carried out study design and review of the article. C.S. was involved in recruitment, follow-up, and article review. P.S. contributed to study design and article review. M.J. performed study design, recruitment, and review of article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.