
Abstract
Objective:
The aim of this review and meta-analysis was to assess spontaneous pregnancy rates after excision of deep infiltrating endometriosis (DIE) in patients with infertility.
Materials and Methods:
An electronic-based search was performed on PubMed, Embase, Scopus, Web of Science, and the Cochrane Database from the last 10 years. All studies, including surgical resection of DIE (>5 mm depth confirmed on pathology) and pregnancy rates published in English, French, Spanish, and Italian during the last 10 years were reviewed. Studies with only ovarian involvement were excluded. A meta-analysis was performed to calculate pooled pregnancy rates, using a random-effects model with inverse-variance weighting. The 95% confidence intervals (95% CIs) for the pregnancy rates were calculated with Wilson Score with continuity correction (WSCC). Studies with extreme heterogeneity and influence were excluded.
Results:
Fourteen articles fit the inclusion criteria (for estimation of overall pregnancy rates) for a total of 587 patients with a mean age of 32.4 years (2 prospective studies and 12 retrospective studies). DIE locations included the intestinal and genitourinary tracts, and other nonvisceral locations. Infertility was defined as preoperative infertility of
Conclusions:
Resection of DIE improves pregnancy rates in patients with infertility. The spontaneous pregnancy rate after surgical resection is 30%. (J GYNECOL SURG 38:24)
Introduction
Deep infiltrating endometriosis (DIE) is defined as the presence of endometriotic nodules with 5 mm or more of invasion below the peritoneum. 1 DIE occurs in 1% of reproductive-age women. 2 Surgery for DIE has proven to be effective for treating pain symptoms refractory to medical management. 3 However, the impact of surgery on reproductive outcomes is less clear.
When patients with DIE wish to conceive, there is a strong debate regarding whether surgical resection will improve pregnancy potential or if assisted reproductive technology (ART) will be necessary. Some researchers have suggested that surgical resection alone has a favorable impact on the ability to conceive.4,5 However, some experts prefer ART prior to attempting surgical management. No consensus currently exists on the management of endometriosis patients with infertility, but recent European Society of Human Reproduction and Embryology (ESHRE) guidelines stated that there was insufficient evidence to recommend surgical resection of DIE prior to ART. 6 This is mainly due to the absence of randomized clinical trials. While the available evidence is lacking, delaying surgical excision of DIE may lead to both symptom and disease progression, with potentially worse perioperative outcomes. 7 In addition, it might be difficult to compare spontaneous to ART pregnancy in observational studies, as the infertility itself could create a confounding factor.
The presence of DIE, both ovarian and extraovarian, has been linked to lower pregnancy rates and possible lower implantation rates with ART.8,9 Surgical removal of ovarian endometriomas, although this may alleviate pain symptoms, is correlated with lower ovarian reserve, requiring more-aggressive ovarian stimulation. 10 However, in cases where no ovarian disease is encountered, it is less clear whether or not DIE affects ART pregnancy rates.9,11
In patients with infertility who have pelvic pain, there is often a strong concern that proceeding with surgical resection of DIE will compromise future pregnancy by decreasing ovarian reserve or creating tubal occlusions through adhesions. Nevertheless, surgical resection may offer a multitude of advantages, including treatment of pain and improvement in a patient's quality of life.12,13
The aims of this study were to review the available literature on pregnancy rates after surgery for DIE in patients with infertility and to report spontaneous pregnancy rates postoperatively.
Materials and Methods
Search strategy
A systematic review of pregnancy rates after DIE surgery was conducted by searching PubMed, Embase, Scopus, Web of Science, and the Cochrane Database of Systematic Reviews
Terms used to conduct the search were pregnancy rates and surgical procedures, operative or surgery or surgeries or surgic* and endometriosis and deep infiltrating or deep infiltrating endometriosis.
The search was limited to English, French, Spanish, and Italian articles published during the last 10 years. References of included articles were also reviewed, and additional studies were added if they were relevant. No funding was needed for performing this meta-analysis and it was exempt from IRB review per institutional guidelines.
An attempt was made to also include unpublished data by reviewing any relevant conference abstracts and studies quoted in other articles.
Study selection
Abstracts identified through the search criteria noted above were evaluated independently by the first 2 authors (S.B. and E.S-S.). Any discrepancies were resolved through discussion between the 2 reviewers, and by reexamining the original articles. If discrepancies were unresolved through discussion, they were discussed with a third author (J.M.). Studies were included if: (1) DIE was defined by a >5 mm peritoneal invasion; (2) excisional, not ablative, surgery was performed; (3) patients had preoperative infertility of
Data extraction and analysis
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to conduct the review. See Figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart of included studies.
The full texts of relevant articles were reviewed by both reviewers independently. For inclusion in the current review, articles had to report postoperative pregnancy rates.
All articles were reviewed, and the following data were recorded: timeperiod of enrollment; study design; DIE location; follow-up time; postoperative pregnancy rates; mode of conception; and postoperative live birth rates.
The meta-analyses were performed in R 3.4.2 14 with the Meta 15 package, using a random-effects model. A Baujat plot was used to identify studies with excessive heterogeneity and influence. 16 Studies with extreme amounts of influence and heterogeneity were excluded. This method was used instead of meta-regression because the studies lacked sufficient variation in study attributes (% of males, locations, etc.) to allow for statistical adjustments.
The random-effects model was used to pool the pregnancy rates for each analysis as the goal of this analysis was to estimate the range of the pregnancy rates seen across the pooled studies. This model was chosen due to the consideration of both within- and between-study effects, compared to fixed effects, which assumes a common effect across all studies. Heterogeneity across studies was assessed using estimates of I2 and τ 2 , which are included in each Forest plot under the results of the random-effects model. Heterogeneity of included studies was examined for each endpoint separately (overall, spontaneous, and ART pregnancy rates); thus, the number of studies included for each endpoint differed.
Given that the number of reported pregnancies was small in some studies, confidence intervals (Cis) for the pregnancy rates were calculated using the Wilson Score method with continuity correction (WSCC). 17 The WSCC CI method was chosen because it restricts the lower limit of the CI from taking on a negative value. An increment of 0.50 was added to studies that reported no pregnancies so that funnel plots could be produced and evaluated.
Assessment of risk of bias
Two reviewers (S.B and E.S-S.) used the Newcastle–Ottawa Quality Assessment Scales for observational studies to complete a quality assessment of the included articles (Supplementary Table 1).
Clinical Characteristics of the Included Studies
Yr(s), year(s); DIE, deep infiltrating endometriosis; ART, assisted reproductive technology.
Publication bias
Assessment for publication bias in the included studies for the outcome of clinical pregnancy was performed graphically using funnel plots (Supplementary Figs. 1–4).
Results
Of 162 identified articles, 14 fit the inclusion criteria, consisting of overall pregnancy rates for a total of 587 patients (2 prospective studies and 12 retrospective studies; Fig 1). Reasons for exclusion included duplicate data, patients without preoperative infertility, lack of pregnancy reporting, review articles, lack of follow-up, endometriosis not defined as DIE, lack of endometriosis excision, and analysis based on models.
Two articles excluded from the overall cohort due to heterogeneity were, however, included in the subanalysis for ART pregnancy for a total of 16 articles.
Table 1 shows the clinical characteristics of the included studies. DIE locations varied and involved the intestinal tract, genitourinary tract, and other nonvisceral locations. Follow-up times ranged from 12 to 96 months.
The pooled overall pregnancy rate in 587 patients who underwent surgical resection of DIE was 44.8% (95% CI: 39.7%–50.1%). In 12 studies with a total of 497 patients, the spontaneous pregnancy rate was 30% (95% CI: 25%–35.5%), and, in 16 studies with a total of 687 patients, the ART pregnancy rate was 22% (95% CI: 14.8–31.4%; Figs. 2–4). In 12 studies with a total of 535 patients, the live birth rate was 41.9% (95% CI: 35.2%–48.9%; Fig. 5). The mean age in the overall patient cohort was 32.41 years. Mean age was collected for each reported study but it was not possible to extrapolate the mean age of patients who achieved pregnancy and those who did not, given the heterogeneity of reporting. Given the different number of articles included in each subanalysis group, and the weighed effect of each study, spontaneous and ART pregnancy rates were not additive.

Forest plot of pregnancy rate after surgical resection of deep infiltrating endometriosis.
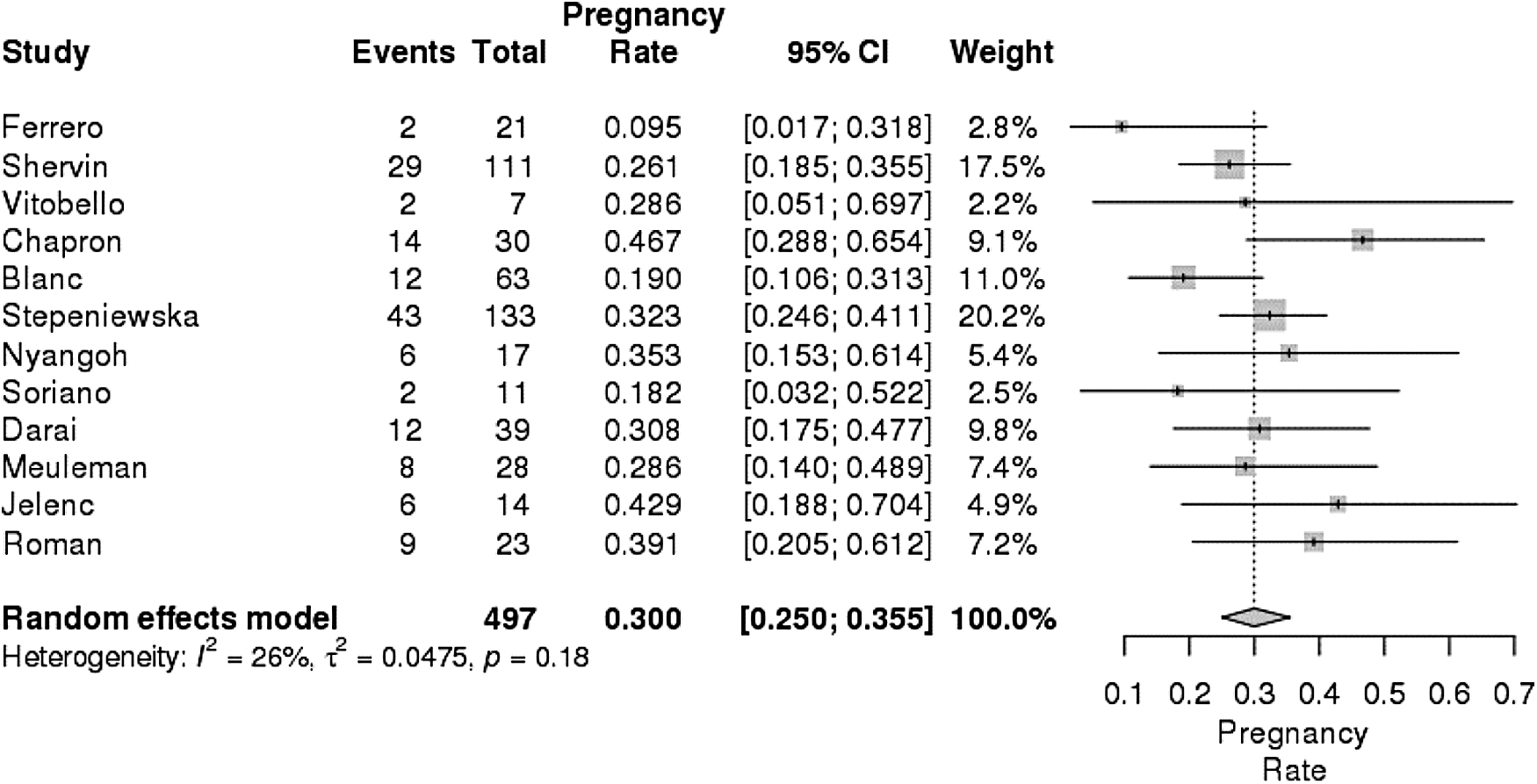
Forest plot of spontaneous pregnancy rate after surgical resection of deep infiltrating endometriosis in infertile patients.
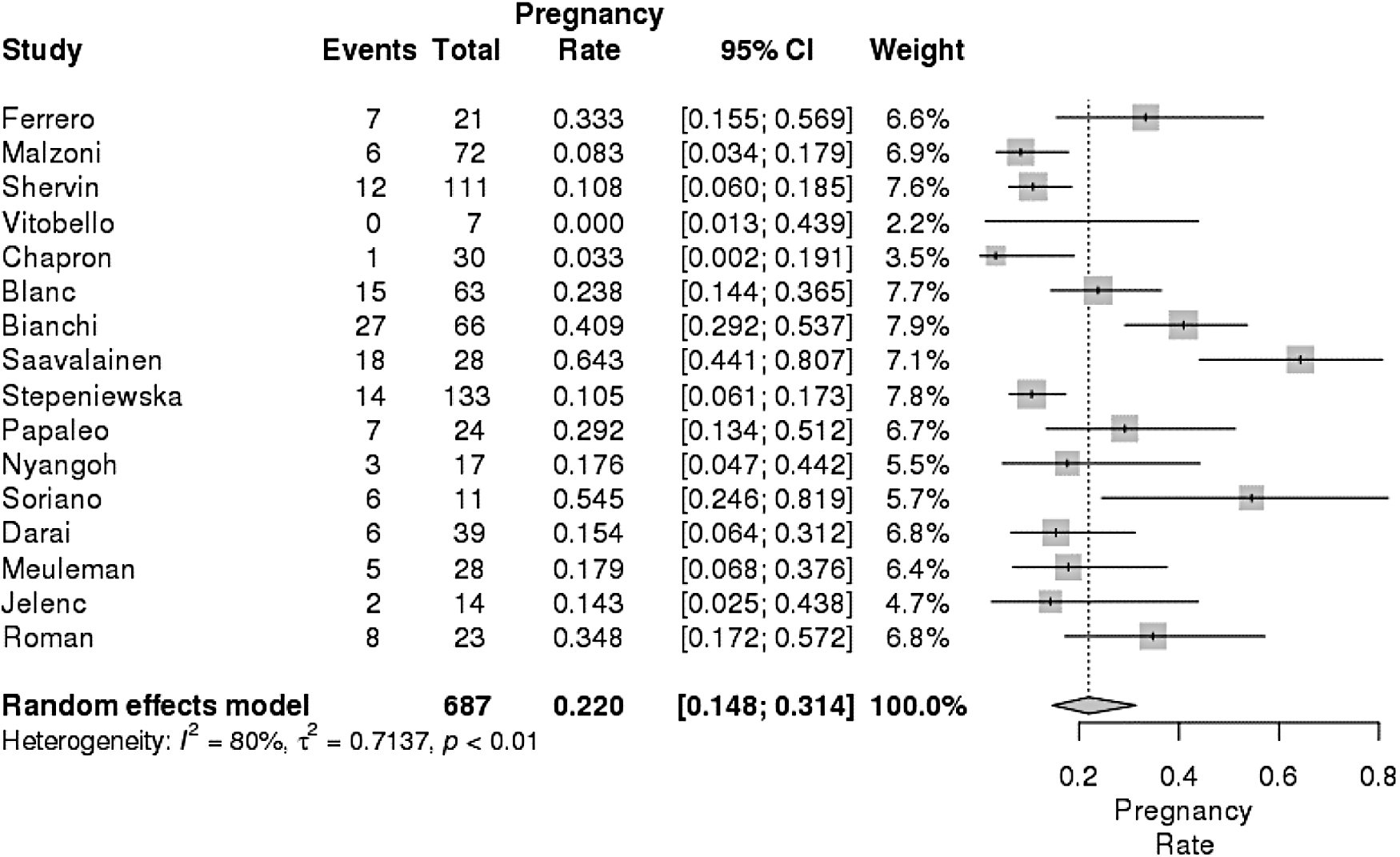
Forest plot of assisted reproductive technology pregnancy rate after surgical resection of deep infiltrating endometriosis in infertile patients.
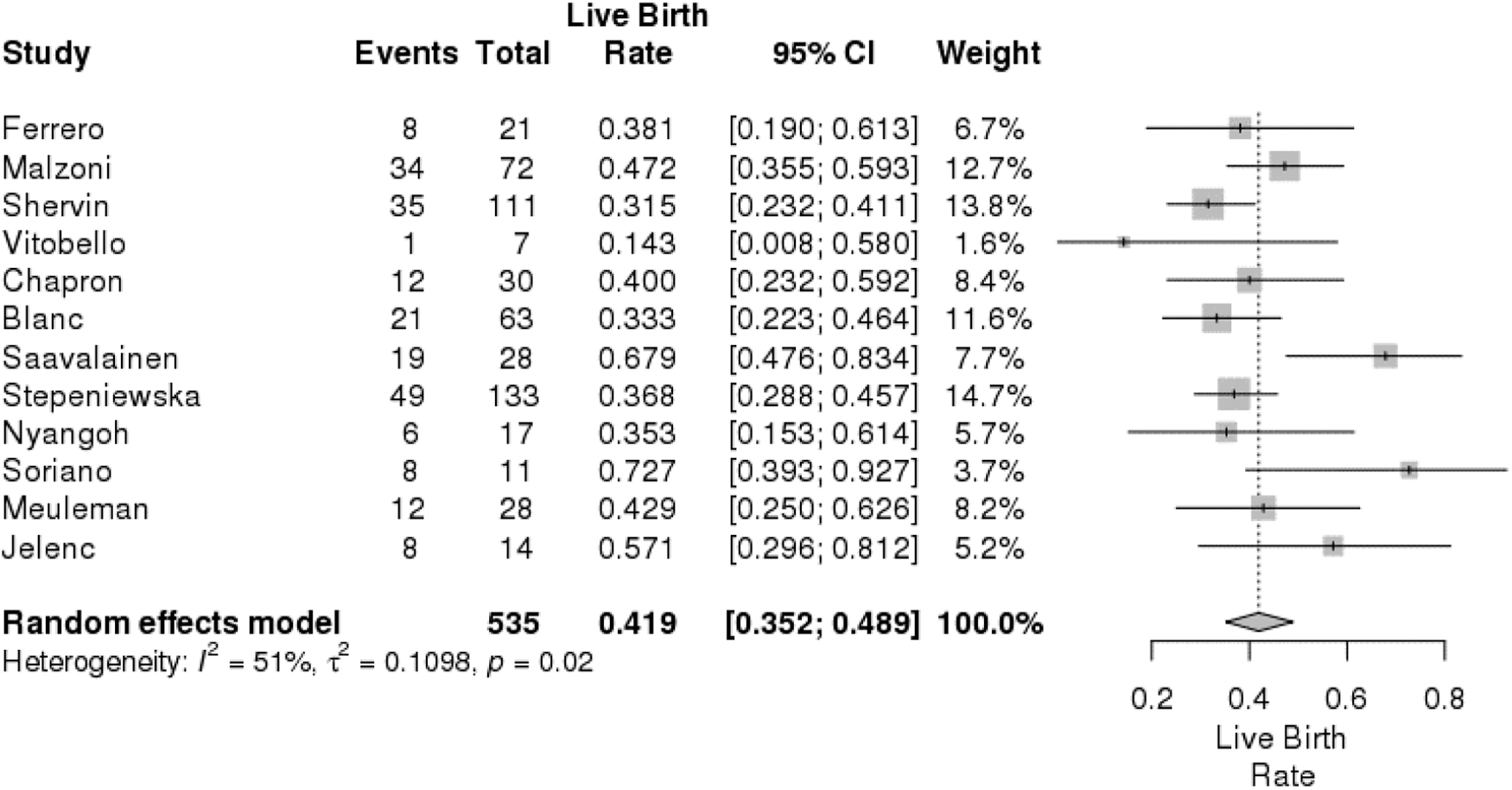
Forest plot of live birth rate after surgical resection of deep infiltrating endometriosis in infertile patients.
Discussion
The pooled pregnancy rate in this meta-analysis of 587 patients undergoing surgical resection of DIE was 44.8%. Spontaneous pregnancy was achieved in 30% of patients after surgical resection.
While it may be difficult to explain the association between DIE and infertility, it is evident that, in many studies assessing postoperative outcomes after surgical resection, a large proportion of the cohort were infertile.18–20 In a 2018 randomized controlled trial by Roman et al., resection of bowel DIE resulted in a 41% spontaneous pregnancy rate, although that study had included patients without preoperative infertility. 21 In another review, by Cohen et al., postoperative pregnancy rates after resection of bowel DIE were as high as 50%, including patients with and without preoperative infertility. 22 Similarly, pregnancy rates after resection of urinary-tract DIE in patients' who wish to conceive have ranged from 64% to 68%.23,24 These studies focused on a cohort of patients with intestinal or urologic DIE. This may be beneficial for counseling patients with isolated intestinal or urologic DIE on postoperative pregnancy rates but not with multiple organ involvements. Patients included in the current study were a comprehensive group with DIE reported in multiple locations. This allowed for better generalizability of results and patient counseling both pre- and postoperatively.
In patients undergoing surgical resection of DIE, although presenting concerns may be both infertility and pain, the incentive to perform surgery is commonly pain. 25 Patients with primarily infertility may choose to present to reproductive endocrinologists where ART, instead of surgery, might be recommended as first-line management. While not all patients undergoing surgical resection for DIE are actively trying to conceive, they are in the appropriate age group in whom future fertility may be a concern. 26 Results obtained from this meta-analysis revealed that surgical resection of DIE enhances fertility, specifically in patients who were unable to conceive preoperatively.
It must be emphasized that 44.8% of patients with infertility were able to conceive after surgical resection of DIE, and that the spontaneous pregnancy rate was 30%. This compares favorably to patients with DIE undergoing ART, with pregnancy rates reported in the range of 10%–43%.27–29 In 1 study using propensity score matching to study pregnancy rates in patients with colorectal endometriosis, cumulative pregnancy rates were found to be significantly higher in patients who underwent resection of colorectal DIE prior to in vitro fertilization (IVF), compared to those who went directly to IVF without surgical resection. 30 Based on that study, the cumulative live birth rate improved with each IVF cycle. After 3 cycles, the live birth rate was as high as 70% in the surgical-resection group.
It has been known for a long time that the presence of endometriosis affects implantation and pregnancy rate, but the mechanism remains unclear. 31 Proposed theories include distorted pelvic anatomy due to adhesions, altered peritoneal function, altered hormonal- and cell-mediated function, endocrine and ovulatory abnormalities, impaired implantation, altered oocyte and embryo quality, and abnormal uterotubal transfer.31–33 Surgical exploration, restoration of normal anatomy, and resection of endometriotic implants, therefore, may help overcome some of these factors and improve fertility. Based on the results of the current meta-analysis, spontaneous pregnancy rates in this patient cohort may be equivalent to those obtained through ART. 34
In addition to decreased fertility, endometriosis has also been linked to increased risk of miscarriage and obstetrical complications.35,36 While data are unavailable to compare live birth rates before and after endometriosis surgery, in this current meta-analysis, the pregnancy rate was 44.8% with a live birth rate of 41.9%. This miscarriage rate is similar to what would be expected in the general population. 37 Reassuring live birth rates after resection of DIE suggest that resection may play a role in reducing the associated peritoneal inflammation with an increased risk of miscarriage; however, further research is warranted before such a conclusion is made. Given that reported pregnancy rates are dependent on an individual study's follow-up time, the longer the follow-up is, the higher the cumulative pregnancy rate will be. Providing time-survival analysis may aid in pooling results collectively in future studies.
In the current meta-analysis, ART was utilized in 22% of patients, but it is unclear, based on the information provided in the studies reviewed, whether or not those patients attempted spontaneous conception first. In addition, it is possible that patients who underwent ART had other causes of infertility that may have made them poor candidates for attempting spontaneous pregnancy. Nevertheless, it is reassuring that less than one-quarter of these patients required the use of ART. The Endometriosis Fertility Index is a simple validated clinical tool that can be used to help guide patients on their chances of spontaneous conception following surgery for endometriosis and based on their staging. 26
Limitations of this study included bias inherent to the retrospective nature of the included studies, and possibly poor quality data. There were no randomized controlled trials (RCTs) available in the literature, possibly due to the challenges inherent with this type of study question. In addition, pregnancy rates may often be underreported, depending on the length of follow-up, and on accurate reporting of patients' desire to conceive. Moreover, patients desiring postoperative fertility might have gone directly to ART without attempting spontaneous conception. This may underreport spontaneous pregnancy rates. Mean age for each included study was pooled; the overall included cohort was young with a mean age of 32.4 years. Age is directly related to pregnancy rates and age is a potential confounding factor in achieving pregnancy as well as route of pregnancy. It is also unclear from the studies reviewed whether all endometriosis was completely resected or whether ovarian endometriosis and/or adenomyosis were present—both known factors that may have a negative on impact pregnancy rates. Other variables affecting pregnancy rates, such as body mass index and smoking status, were not reported consistently and could not be accounted for.
Strengths of this meta-analysis included pooling a large number of patients with DIE with infertility to provide a more-accurate assessment of the impact of DIE resection on pregnancy rate. Because only patients with preoperatively infertility were included, this was is a more-uniform cohort, compared to other published studies. Although difficult, RCTs should be considered to examine this clinical question further.
Conclusions
Surgical resection of DIE improves pregnancy rates in patients with infertility. The spontaneous pregnancy rate following surgical resection is 30%. See Table 1 for information on the included studies.18,23,24,38–50
Footnotes
Authors' Contributions
Drs. Behbehani and Suarez-Salvador were responsible for the study's design. Drs. Buras and Kosiorek were involved with its statistical analysis. Dr. Behbehani wrote the article, and together with Drs. Suarez-Salvador, Yi, and Magrina were responsible for the articles intellectual and technical content. Drs. Yi and Magrina worked on revising the article.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was obtained in connection with this research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.