
Abstract

Subject
MRKH syndrome is characterized by the congenital absence of the uterus, cervix, and upper two-thirds of the vagina. This anomaly affects 1 in 5000 females and is thought to arise in-utero between the sixth and twelfth week of gestation when the paramesonephric ducts fail to develop. 1 The round ligament originates from the embryonic gubernaculum and is, therefore, intact in women with MRKH syndrome. Fibroids of the round ligament are very rare. They more commonly originate from the extraperitoneal portion of the round ligament (inguinal canal or labia majora) but can be intraperitoneal in ∼ one-third of patients. 2 This article presents a case of a symptomatic, intraperitoneal, pedunculated, round ligament fibroid in a patient with MRKH syndrome. To the current authors' knowledge, there are only 5 such patients previously reported in the literature.1–5
Case
A 40 year-old patient known to have MRKH syndrome presented to the current authors' clinic with left lower-quadrant discomfort and pelvic pressure of 1 year's duration. She had been diagnosed with Müllerian agenesis at age 21 and undergone successful vaginal reconstruction in 1999 in this institution. At that time, she was investigated thoroughly, including an unremarkable pelvic ultrasound. She was lost to follow-up until this new presentation when a large, nontender, mobile solid mass was felt in her left lower quadrant on bimanual pelvic examination. Transvaginal USG detected a 7 × 5–cm, heterogeneous, well-demarcated solid mass in her left lower quadrant, reaching the midline. The mass appeared to be separate but abutting the adjacent left ovary. No abnormality was noted in the right adnexa. This patient's serum cancer antigen (CA)–125 level was normal (6.9 U/mL). MRI was performed, revealing similar findings suggestive of a left leiomyoma, measuring 6 cm in its largest diameter (Fig. 1). She was counseled and agreed to proceed with laparoscopic myomectomy and risk-reducing bilateral salpingectomy (BS).
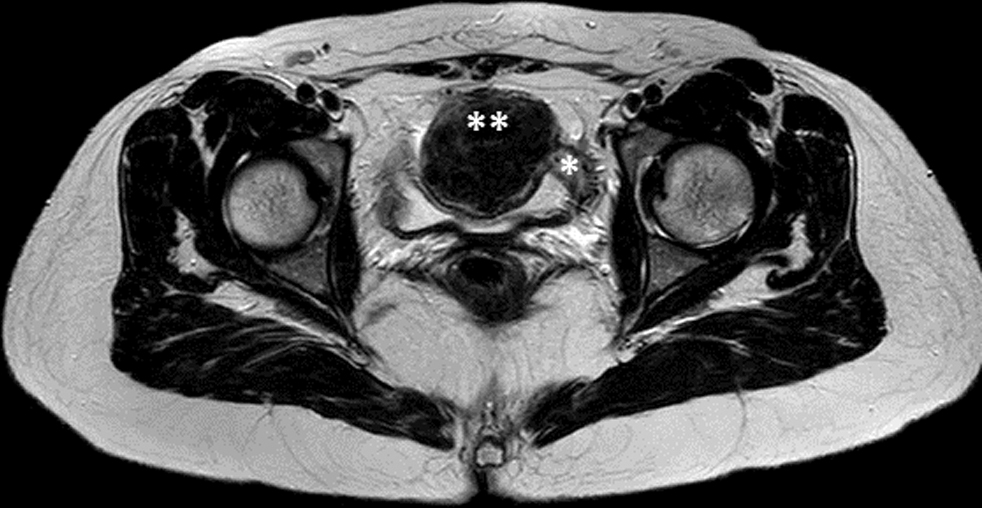
Magnetic resonance image of the leiomyoma (**) originating from the left round ligament (*) in a patient with Müllerian agenesis.
Intraoperatively, a pedunculated, solid round mass was noted arising from the left round-ligament stump. The mass was clearly distinct from the adjacent left ovary and fallopian tube (Fig. 2). Using a bipolar sealing device, the stalk of the myoma was desiccated and subsequently transected with endo-shear scissors. Using monopolar energy, the round ligament stump was then transected to prevent any future recurrences of the same mass. Risk-reducing BS was then performed. To prevent potential complications of mechanical morcellation, the specimen was morcellated into a bag, and the Alexis Contained Extraction System® (Applied Medical) was used. The surgery was completed without any complications and with minimal blood loss. The official pathology report confirmed that this patient had a leiomyoma (Fig. 3) and benign fallopian tubes. The patient tolerated this procedure well and was discharged to go home in a stable condition on postoperative day 1.

Laparoscopy showing the leiomyoma (**) originating from the left round ligament (*) with a clearly separate left ovary (arrow) in a patient with Müllerian agenesis.
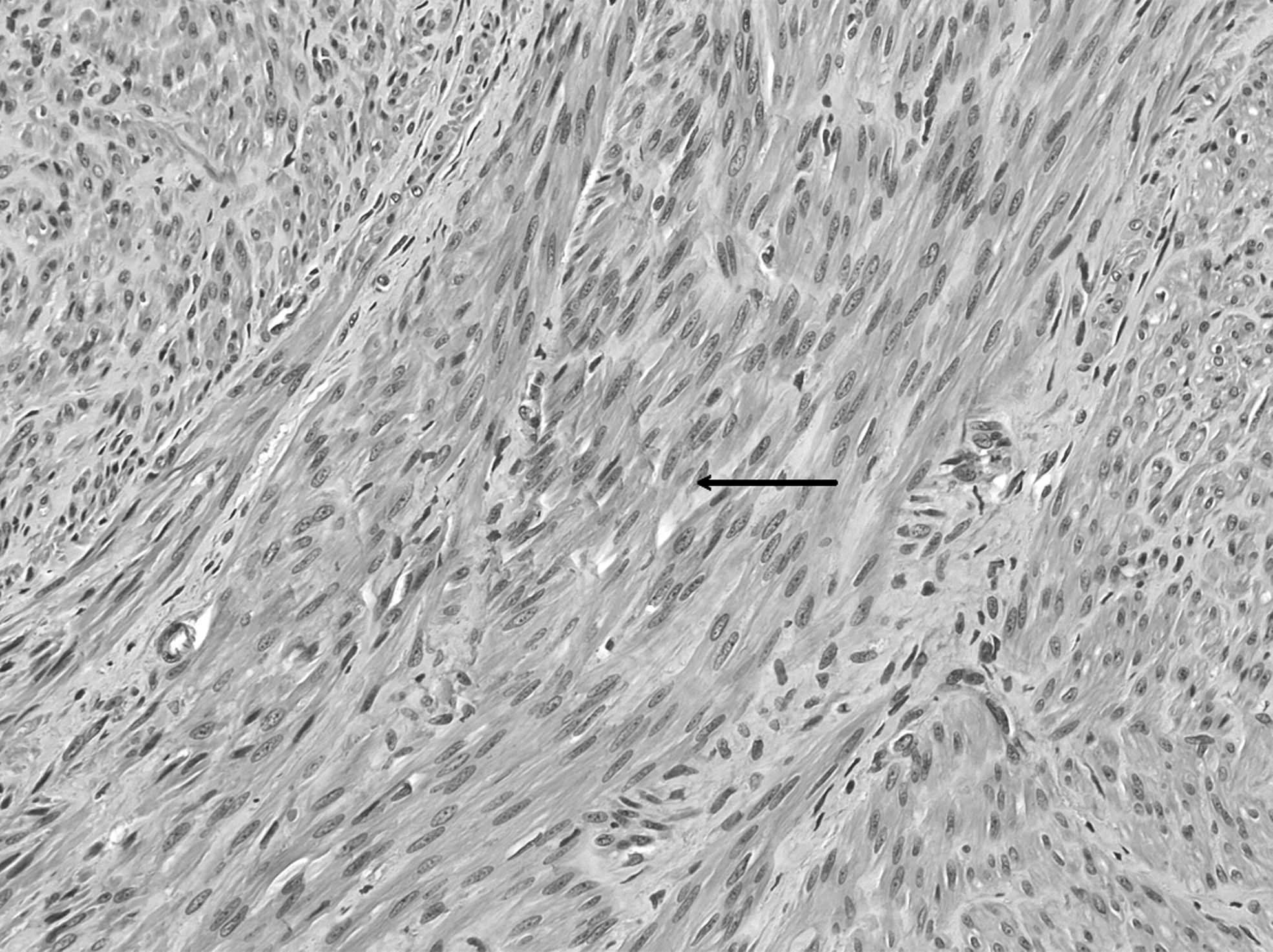
Histologic section (with hematoxylin and eosin staining) showing typical benign spindle-shaped myocytes with cigar-shaped nuclei (arrow) in a patient with Müllerian agenesis.
Review
A thorough literature review was conducted and 40 cases of leiomyomas in women with MRKH syndrome were identified (Table 1).1–37 Most of these leiomyomas originated from hypoplastic uterine remnants. Only 5 were described as originating from the round ligament stump, making the current patient the sixth to be reported in the literature.1–5 Patients with this condition can be asymptomatic and diagnosed incidentally at the time of pelvic imaging, while other patients can present with chronic pelvic pain, pressure symptoms, increased abdominal girth, or acute pain due to torsion of the leiomyoma around the ipsilateral adnexa.
Literature Review of Leiomyomas in Patients with Müllerian Agenesis
yr, year; MRKH, Mayer–Rokitansky–Küster–Hauser; BSO, bilateral salpingo-oophorectomy; GI, gastrointestinal.
Trainee's Perspective
Women with Müllerian agenesis lack uteri. Therefore, when these women present with solid pelvic masses, trainees are unlikely to consider leiomyomata in the differential diagnosis, as those are most-often uterine in origin. The trainees will first think of an adnexal mass, irrespective of the patient's clinical presentation, leading to unnecessary testing, laparotomy, and heightened patient anxiety. This can be avoided with the knowledge that women with Müllerian agenesis might have rudimentary uterine horns containing nonfunctioning myometrial tissue and, rarely, active endometrium that, therefore, could develop leiomyomas and sometimes even adenomyosis and endometriosis.34,38 Moreover, women with Müllerian agenesis have an intact round ligament that could also be the origin of leiomyomata.
Faculty's Perspective
Of the 40 published cases on leiomyomas in women with MRKH syndrome, several were misdiagnosed preoperatively as being adnexal tumors.1,4,8,10,16,17,27,30,34,35 For the current patient, the current authors did first think of a possible adnexal mass and thus requested a CA-125 level test. However, the normal-looking ovary adjacent to the pelvic mass on USG was highly suggestive of a leiomyoma. This was subsequently confirmed by pelvic MRI.
Whether the leiomyoma originates from the uterine remnant or round-ligament stump, the mass is almost often pedunculated in nature. The most-common presentation cited in the literature is that of pelvic pain. Acute torsion of the adnexa around the leiomyoma pedicle has been described in 7 patients, necessitating emergent surgery to salvage the affected ovary.10,16,26,29,31,34,35 Myxoid degeneration of a large leiomyoma has also been described in a patient with Müllerian agenesis. 36
When it comes to management, the current authors do recommend removal of the leiomyoma—especially if it is symptomatic. Considering the possibility of torsion, the current authors also advise removing large asymptomatic leiomyomata—especially in younger women in need of ovarian function. Most cases reported in the literature were managed by laparotomy. The current authors chose a laparoscopic approach to benefit the patient with the well-established advantages of minimally invasive surgery, including quick recovery, decreased postoperative pain, decreased hospital stay, and lower incidence of postoperative complications. Enclosed morcellation in a bag was performed, as this has become the standard of care ever since the U.S. Food and Drug Administration issued recommendations on the cautious use of power morcellation. 39 In fact, leiomyosarcomas, although rare, could arise from the round ligament and, therefore, extrauterine fibroids should not be presumed to be benign. 40 Following resection of the fibroid, we resected the round ligament stumps to prevent potential recurrence of the myoma in the future. Recurrence of uterine remnant fibroids has been reported, necessitating reoperation. 10
In conclusion, it is important for trainees to know that a solid pelvic mass in a woman with Müllerian agenesis is not always ovarian in origin. The mass could be a leiomyoma originating from the round ligament or from Müllerian remnants. Diagnosis can be made by pelvic USG and MRI, which are helpful for distinguishing a leiomyoma from any ovarian pathology. Laparoscopic resection is feasible and recommended to avoid potential complications, such as torsion.
Footnotes
Authors' Contributions
Dr. Hamze is the trainee who was primarily involved in the care of this patient. He drafted the article, together with Drs. Mourad and Chamsy, and conducted a thorough literature review. Dr. Mourad, another trainee, also cared for this patient. Dr. Seoud was the primary faculty member who initially evaluated the patient in a clinic and conducted the work-up. He also obtained the patient's consent to be included in this article. He contributed to the conception of the work, together with Dr. Chamsy, and reviewed the article. Dr. Chamsy operated on the patient and was involved in data acquisition. All of the authors gave final approval of the article.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this article.