
Abstract
Objective:
Inclusion of minority women in gynecologic research is vital for preventing health care inequities and disparities. This research was conducted to determine how frequently race and ethnicity data were reported in oral presentations at the Society for Gynecologic Surgeons (SGS)'s annual meeting.
Materials and Methods:
The abstracts and articles associated with SGS oral presentations between 2016 and 2020 were reviewed. Data regarding the numbers of subjects and reported races and ethnicities were extracted from each study. The proportion of studies that reported data about race and ethnicity was calculated. The racial and ethnic distributions of subjects within the studies that reported race and ethnicity were compared to distributions in the U.S. census data.
Results:
The inclusion criteria were met by 72/92 available abstracts and 28/37 available, articles. Data were reported on participants' race in 10/72 (13.9%) abstracts and 21/28 (75.0%) articles. Ethnicity was reported in 3/72 (4.2%) abstracts and 14/28 (50.0 %) articles. In the abstracts and articles that did report on race, races other than White were underrepresented, compared to the U.S. population.
Conclusions:
Most research abstracts at SGS annual meetings did not include race or ethnicity data. SGS articles were more likely to report these data but did not represent the the U.S. population diversity accurately. (J GYNECOL SURG 38:241)
Introduction
Health care disparities are preventable differences in the burden of disease, and/or lack of opportunities to achieve optimal health experienced by socially disadvantaged populations. 1 The treatment of race as a biologic concept contributes to limitations in screening, timely diagnosis, and effective treatment of disease among some racial and ethnic groups. Differences are not related to genetics or biology, but rather to those of human experience, ancestry, and racism. 2 Race is a mixture of physical, behavioral, and cultural attributes. Ethnicity recognizes differences among people mostly on the basis of language and shared culture. Race is, therefore, a social construct and not a biologic difference, and inequities in gynecologic health outcomes based on race and ethnicity are not due to biologic differences, but to racism.
Acknowledgement of disparities within women's health starts with accounting of inclusion. The National Institutes of Health (NIH) requires documented inclusion of minority populations in clinical research or, if such populations are excluded, that funded investigators make a sound argument for this exclusion. 3 Despite this, past studies have failed to meet this standard. A study among NIH-sponsored studies between 2004 and 2009 found no improvement in race reporting over this 5-year timeperiod. 4 One-fifth of the studies failed to report the racial/ethnic distribution of their participants, and when these data were reported, Black and Hispanic subjects remained underrepresented relative to the U.S. population. If transparent reporting and diverse research populations are not obtained, there is a risk of mistreating minority populations or making clinical decisions based on studies in which these populations are not represented. Research mistreatment of marginalized populations has many historical examples, including J. Marion Sims' abuse of enslaved Black women, 5 the use of Henrietta Lacks' cervical-cancer cells without her consent, 6 and untreated syphilis in the Tuskegee Syphilis study. 7
Lack of trust, opportunity costs of engaging in research, and lack of study documents in appropriate languages all represent barriers to the participation of women of color in gynecologic research. For women's health research, these barriers led to a preponderance of studies including White, non-Hispanic participants and the creation of guidelines for care based on data that were not generalizable to minority women. 8 Meeting abstracts are typically in the format that new findings are presented to the scientific community, although they may represent data not completely presented in a published article.
The Society of Gynecologic Surgeons' (SGS) Collaborative Research in Pelvic Surgery Consortium (CoRPS) analyzed the percentage of oral-presentation abstracts from the SGS Annual Scientific Meetings and articles published in the meeting issues of the American Journal of Obstetrics and Gynecology (AJOG) over a 5-year period that reported race/ethnicity. It was hypothesized that race/ethnicity are rarely reported in abstracts and are reported in articles more frequently, but, when reported, do not represent the diversity of the U.S. population accurately.
Materials and Methods
A self-selected group of the SGS CoRPS' members, who are gynecologic surgeons with expertise in scientific reviewing, analyzed the abstracts for all oral presentations at the SGS Annual scientific meetings for a 5-year timeperiod (2016–2020) that were available online in portable document formats (PDFs).* Furthermore, all articles published in the “Meeting Papers” section of the AJOG featuring outstanding articles from the annual meeting of the SGS for a 5-year period were reviewed.9–52
The New York Medical College's institutional review board (IRB) confirmed that this study did not require IRB review, as no research on was conducted directly on human subjects. All abstracts and articles were reviewed to determine eligibility for inclusion. Abstracts or articles that did not involve human subjects were excluded. Studies that utilized research databases rather than cohorts assembled by the researchers were also excluded, as research database cohorts cannot be controlled by researchers and often have racial and ethnic distributions already reported and published. Education studies were excluded when the research participants were medical trainees.
Information was abstracted from each eligible abstract or article regarding total number of participants and reported information about race and/or ethnicity (American Indian or Alaska Native, Asian, Black, Native Hawaiian or Other Pacific Islander, White, and Hispanic).
The primary outcome was the proportion of abstracts that were full oral presentations at the SGS Scientific Meetings (2016–2020) and that included reporting of participants' races. Among those abstracts and articles when data were available about participants' races and/or ethnicities, the absolute number of participants as well as the number of participants identified as each reported race and/or ethnicity were noted. The distribution of reported participants' races and/or ethnicities was compared to the most recent U.S. population census data (2016–2019). 53
Descriptive statistics included counts and percentages. χ 2 Testing was used to compare percentages of various race and ethnicity categories when reported in abstracts and articles with the percentages of the same categories in the most recent U.S. census data. Spearman correlation coefficients were calculated to compare the type of study (retrospective versus prospective) and the total number of subjects with whether race or ethnicity was reported.
Results
A total of 92 abstracts (2016-2020) and 37 articles (2016–2020) were reviewed. Twenty abstracts were excluded: 9 that analyzed existing databases; 9 that were not human subjects' research; and 2 that were withdrawn and did not have abstracts available for review. The 9 abstracts that did not qualify as human-subjects' research on gynecology patients included 2 animal studies, 1 systematic review, 1 “trend and innovation” abstract, 3 cost studies, and 2 education studies. Seventy-two abstracts remained that met the inclusion criteria (Fig. 1). Of 37 articles, 5 that analyzed existing databases and 4 that did not qualify as human subjects' research (2 systematic reviews and 2 cost studies) were excluded, leaving 28 manuscripts that met inclusion criteria (Fig. 2).
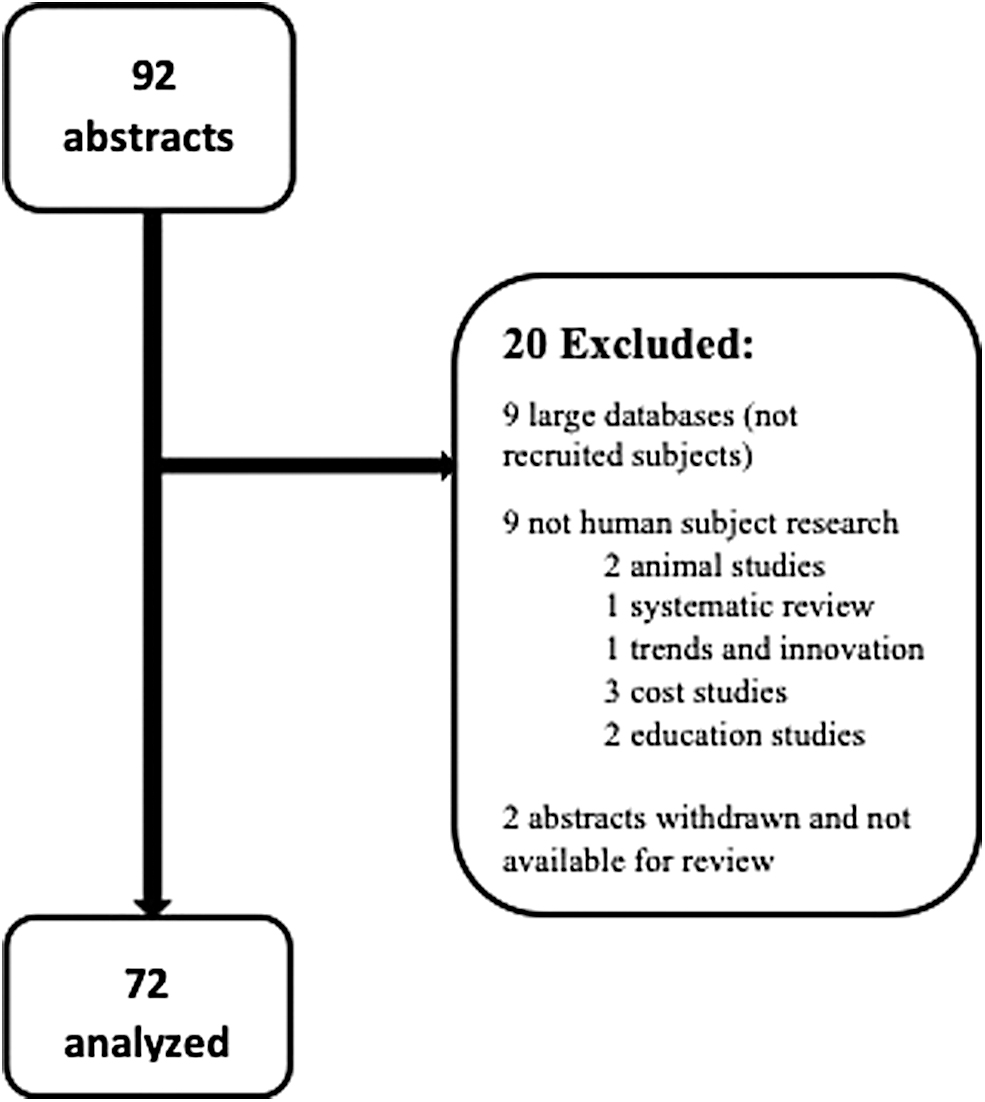
Flow diagram of included and excluded abstracts.
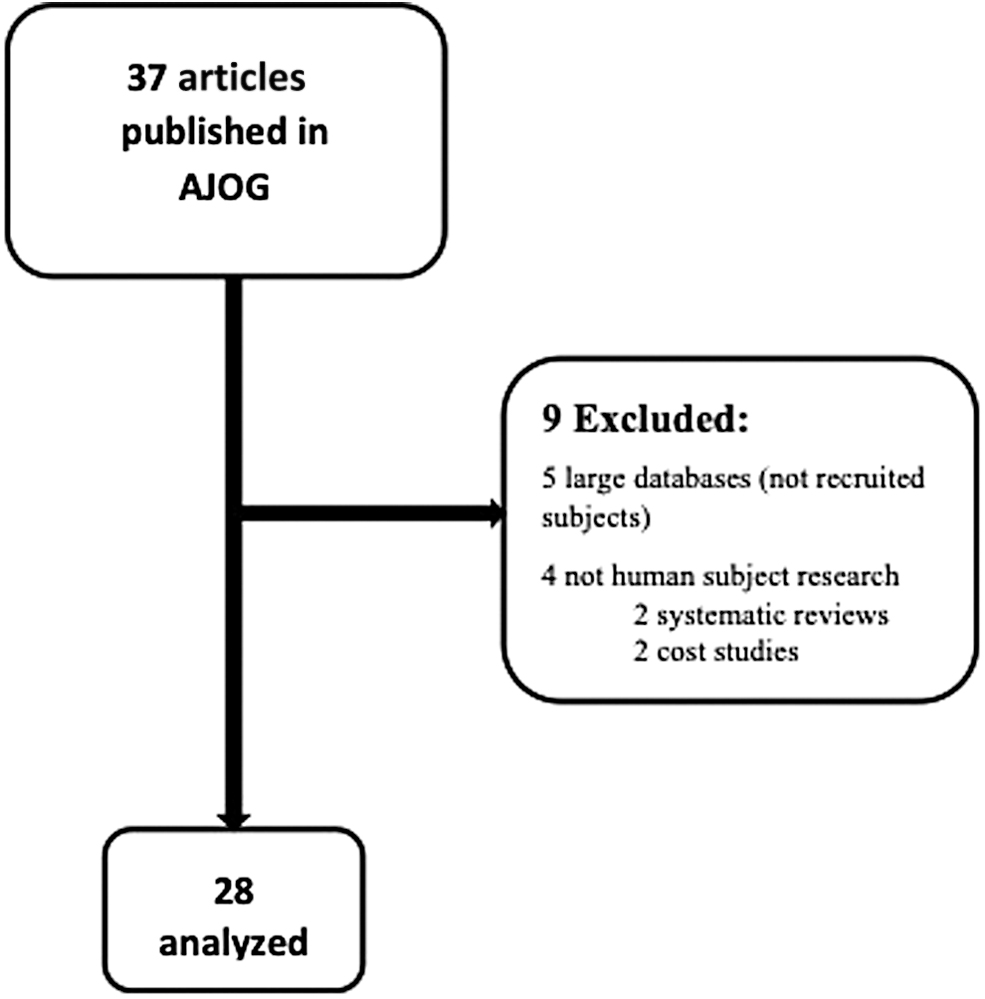
Flow diagram of included and excluded articles.
For the primary outcome, race was significantly reported less frequently in abstracts, compared to articles (10/72 (13.9%) abstracts and 21/28 (75.0%) articles (p < 0.001); likewise, ethnicity was only reported in 3/72 (4.2%) abstracts, compared to 14/28 (50.0 %) articles (p < 0.001) See Table 1.
Reporting of Race and Ethnicity Among eligible Abstracts and Articles
Yrs, years; SGS, Society of Gynecologic Surgeons; AJOG, American Journal of Obstetrics and Gynecology.
Among studies that reported race, many reported only the number of participants who identified as White and did not describe reported races for those in the “other” category. This categorization of White or non-White without further description of racial identity was common and not significantly different (p = 0.16) between abstracts (5/10, 50%) and articles (5/21, 25%). Due to this incomplete reporting of races other than White, percentages in Tables 2 and 3 do not add up to 100%.
Description of Race and Ethnicity of Participants in Abstracts for Which Race or ethnicity Data Were Available *
Often, the totals and percentages did not add up to 100, as many studies reported the race and ethnicity of only some of their participants.
N/A, not available.
Description of Race and Ethnicity of Participants in Articles in Which Race or Ethnicity Data Were Available *
Often, the totals and percentages did not add up to 100, as many studies only reported the race and ethnicity of some of their participants.
The abstracts that reported race included a total of 1677 participants cumulatively, of whom 1398/1677 (83.4%) identified as White, 74 (4.5%) identified as Black, and 3 (0.2%) identified as Asian. No information was provided about whether participants identified as Native Hawaiian/Pacific Islander, American Indian, or Alaska Native. The 3 abstracts that reported ethnicity included a total of 1012 participants cumulatively, of whom 228 (22.5%) identified as Hispanic (Table 2). Of note, 2 studies included significantly more Hispanic women, which increased the percentage of Hispanic subjects overall. One study conducted in southern California in 2017 had 54/130 (42%) Hispanic subjects, 33 while another study conducted in Texas in 2018 included 30/30 (100%) patients who were all Hispanic. 54
The 21 articles that reported information about race included a total of 17,592 participants, of whom 8358 (47.5%) identified as White, 1053 (6.0%) identified as Black, and 655 (3.7%) identified as Asian. No information was provided about whether participants identified as Native Hawaiian/Pacific Islander, American Indian, or Alaska Native (Table 3).
Two studies among these 21 articles that reported information about participants races contributed heavily to the racial distributions, particularly the percentage of patients identifying as Black. A 2018 study conducted in Cleveland enrolled 295/763 (38.7%) participants who identified as Black. 40 This study contributed 295/1053 (28.0%) of participants who identified as Black, but only 763/17,592 (4.3%) of all participants for whom data were available about race. A sensitivity analysis removing this single study from our analysis was performed, and the proportion of research participants who identified as Black decreased from 6% to 758/16,539 (4.6%).
Similarly, a large retrospective analysis conducted in southern California in 2019 included 13,404 participants, of whom 474 (3.5%) identified as Black. 46 This southern California study contributed only 45% of participants who identified as Black but 13,404/17,592 (76.2%) of research participants overall. In another sensitivity analysis removing this southern California study from the analysis, the proportion of research participants who identified as Black increased from 6% to 579/4188 (13.8%). In a third sensitivity analysis excluding both studies, the proportion of research participants who identified as Black was 8.3% (284/3,425); 80.8% (2,767/3,425) identified as White, and none identified as Asian.
The 14 articles that reported information about ethnicity included 14,524 participants cumulatively, of whom 7247 (49.9%) identified as Hispanic (Table 3). The 2019 study in southern California noted above contributed the majority (92.3%, 13,404/14,524) of participants for whom data were available regarding ethnicity and 96.1% (6961/7247) of the participants who identified as Hispanic. 46 If this single study were removed from the cumulative total, the proportion of participants who identified as Hispanic among the total number of participants for whom ethnicity was reported would become 25.5% (286/1120).
Only 2/72 (2.8%) abstracts and 1/28 (3.6%) article reported on other social determinants of health, such as socioeconomic status, level of education, or insurance status.
No significant association was seen between the temporal direction of the study (retrospective versus prospective) and whether race or ethnicity was reported in the abstracts (p = 0.09). In addition, no significant correlation between the number of participants in the studies and whether race or ethnicity was reported was found (p = 0.77). This held true for the articles as well, with no correlation between type of study (p = 0.11), or number of participants (p = 0.38) and whether race or ethnicity was reported.
In U.S. Census Bureau data between 2016 and 2019, 78.5% of American women self-reported as White, 14.6% self-reported as Black, 2.0% self-reported as American Indian and Alaskan Native, 6.8% self-reported as Asian, and 0.5% self-reported as Native Hawaiian. In the same U.S. census data, 17.7% of women self-reported having Hispanic ethnicity. Including all the reviewed articles for which data about race were available, White (47.5%), Black (6.0%), Native Hawaiian/Pacific Islander (0%), American Indian or Alaskan Native (0%) races were significantly under-represented, compared to national U.S. census data (all p < 0.001). When the 2 outlier manuscripts described above (from Cleveland and southern California) were excluded, however, White race was over-represented, while Black race remained under-represented (both p < 0.001). Hispanic ethnicity was overrepresented in this sample of articles whether or not the southern California study was included (p < 0.001).
Discussion
Most abstracts and 25% of articles featured at the SGS meetings did not report information about participants' races, and many only noted the proportion of White participants. Ethnicity was rarely reported. Black, Native Hawaiian/Pacific Islander, and American Indian/Alaskan Native races were under-represented relative to the U.S. census.
These findings have started to uncover larger issues within gynecologic research, including the lack of representative recruitment into studies, the lack of standards in reporting on study populations within articles, and the possible perception that these demographics are not essential when condensing research findings into abstract form.
However, it should be noted that lack of reporting in abstracts does not necessarily translate to authors not finding it important or collecting the information. Of note, there are often word limits to abstracts that restrict which data are included, and authors looking to save words may not find reporting of race and ethnicity vital in the abstract format but do report them in the articles. Data that support this emerged in the fact that that more articles emanating from SGS presentations in AJOG—which presumably apply higher-quality science, as they were accepted for full publication and had more space for data inclusion—reported race and ethnicity more consistently. One measure that may help this issue of reporting at the abstract level would be a requirement for reporting race/ethnicity in original studies involving human subjects in the abstracts and allowing 25–50 more words in abstracts to allow these data to be included. This small measure could help greatly with abstract inclusion of these vital data.
These issues with inadequate reporting of race and ethnicity are not unique to gynecology. The general medical community has reported disparities in recruitment into studies and inconsistency in reporting diversity. 55 NIH-sponsored trials, which “highly recommend” racial and ethnic reporting, adopt this standard incompletely. The aforementioned study among NIH-sponsored studies between 2004 and 2009 shows that reporting is not universal, and Black and Hispanic women are still under-represented even in nationally funded research. 4 While under-representation of minority populations may be an effect of biases at the institutions where the research was performed, such as less representation from non-White races in the region, this points to a systemic problem of not performing research in such a way that represents diverse populations. Another study found that, of articles included descriptions of participant races, 72% did not describe how race was ascertained (i.e. self-identification, researcher assignment, or use of language as a proxy). 55
Having broad racial and ethnic representation in research is imperative, especially in prospective studies used to establish standards of care. Without representation, the medical community cannot begin to minimize disparities in outcomes or uphold societal equity in health care. Journal reviewers and editors can play an integral role by requiring reporting race and ethnicity, an explanation of how they were assigned, or an adequate explanation for why such reporting is not appropriate. This is currently required by the Journal of the American Medical Association and Obstetrics and Gynecology. 56 57 Deliberate efforts to promote diversity among members of research study sections, journal editorial boards, and leadership positions in professional societies, is critically important.
Researchers should also promote more-comprehensive reporting of other social determinants of health. Racial health disparities are different from—and can be exacerbated by—disparities in socioeconomic status measures.58–60 Education is not an acceptable proxy for income in studies of ethnically diverse populations, and it is known that socioeconomic environmental factors affect disease care-seeking.
This collaborative work exposed current incomplete reporting of minority populations in research and the responsibility to do better. To start, this effort should include comprehensive reporting of self-identified race and ethnicity. Only when researchers are intentional and transparent can they identify health care disparities and take steps to improve health care outcomes in minority groups. It is imperative to move beyond viewing race as a biologic construct—grounded in racist and White-supremacist notions that have been engrained in gynecology historically—to reverse disparities and to achieve health equity.
Strengths of the current study included the 5-year time interval studied, the separate analysis of abstracts and articles, and distinction between race and ethnicity as different concepts. There were several limitations, including that abstract exclusion of race and ethnicity reporting did not necessarily denote lack of interest in or lack of collecting these data, but may instead be a reflection of abstract word limits or lack of requirements of reporting at the abstract level; these are barriers that would be easy to correct. It was not possible control for geographic location of study participants, as not all studies had this information stated clearly, so it was not possible to compare the representation in a study to representation of race or ethnicity within the region where the study was performed, which would have been a better comparator than the entire U.S. census distribution. In addition, individual authors were not contacted to ascertain whether additional information about race and ethnicity were collected but not reported in abstracts or articles. It also was not possible to evaluate how race and ethnicity were obtained in most studies. Funding sources were not cross referenced to see whether study funders had a policy on reporting on race and/or ethnicity.
Because the actual numbers of abstracts and manuscripts reviewed were small, a few outlier studies skewed results significantly, but sensitivity analyses were performed with and without these studies included. Also, given the small number of eligible studies in every given year, it was not possible to analyze trends from year to year in reporting. Finally, there were limitations in the way the U.S. Census data were reported, especially in categorizing certain subgroups. For example, the category of Black (race) was broad and did not delineate Caribbean–American, African, or Afro–Latinx categories further. In addition, in many studies, Hispanic ethnicity was also grouped inappropriately with race, making it difficult to discern the racial identity of Hispanic participants or determine if this was queried distinctly from racial identity.
Conclusions
Despite 1993 federal requirements that the NIH ensure members of minority groups are included in clinical research, representation of specific racial and ethnic identities in research currently does not mirror the U.S. population. The majority of abstracts selected for full oral presentation at the SGS Annual Scientific meetings did not report participants' races consistently, something that could be improved by requiring reporting race and ethnicity in abstracts and allowing higher word counts to allow for these data. Even among articles featured in AJOG from the SGS Annual Meetings in 2016–2020, half did not report participants' ethnicity and one-quarter did not report races.
The rationale for reporting both race and ethnicity in scientific publications reflects the evolved understanding of women as more than physiologic beings; they have sociocultural experiences that can influence patient-reported outcomes and lived experiences in women's health care and gynecologic surgery. This specialty has perpetuated racist ideas throughout history, and it is necessary to identify, correct, and reverse this practice.
Footnotes
Author Disclosure Statement
Dr. Grimes is the associate chair of the Collaborative Research in Pelvic Surgery Consortium, Society of Gynecologic Surgeons. Dr. Clare is on the Board of Directors of the American College of Obstetricians and Gynecologists (ACOG) and the Board of Trustees of the National Medical Association. Dr. Meriwether receives royalties for Elsevier Publishing and a travel stipend from the Society of Gynecologic Surgeons. Drs. Brown, Iglasia, and Rogers receive royalties from Wolters-Kluwer, Inc. (as an UpToDate, Inc., author) and performs expert consultations for Grand Rounds, Inc. Dr. Brennand receives grant funding from Boston Scientific. Dr. Iglesia is also on the McGraw-Hill; editorial board of OBGManagement and the executive board of the SGS, as well as being on the advisory Board and a council member of the Patty Brisben Foundation, the Healthy Women Foundation, and the Foundation for Female Health Awareness. Dr. Rogers also receives a stipend and travel reimbursement from the International Urogynecologic Association and American Board of Obstetricians and Gynecologists.
No financial conflicts of interest exist for the remaining authors.
Funding Information
All listed authors confirm that their efforts in this research were supported by an institution (SGS) that is primarily involved in education or research. However, no funding was obtained for this project.