
Abstract
Abstract
Endometriosis is a debilitating disease and a significant health problem for women of reproductive age. Extirpative surgery of endometriosis involves cytoreduction of visible endometriosis. Although surgical management is an important treatment option for patients with endometriosis, the complexity of the surgery confers multiple challenges to even the most experienced surgeons. A high level of training and surgical experience, as well as an excellent knowledge of pelvic anatomy, is paramount in order to maximize benefits of the procedure and minimize surgical complications for patients. This article reviews the surgical challenges associated with extirpative surgery of endometriosis and briefly discusses surgical management of bowel and urinary-tract involvement. This review is based on a search of Medline,® PubMed, and citation lists of relevant publications. Subject heading and key words used included deep infiltrating endometriosis, radical endometriosis surgery, ureteral endometriosis, and bowel endometriosis. (J GYNECOL SURG 38:7)
Introduction
Extirpative surgery of endometriosis involves cytoreduction of visible endometriosis. This is typically offered to women with debilitating symptoms of endometriosis who have completed childbearing and have had failed medical therapies and conservative surgery treatment options. 1 Laparoscopic access has become standard for treating endometriosis due to the advantage of having better views and access to lesions deep in the pelvis. The lower postoperative complication rate and morbidity, compared to laparotomy, is also a well-established benefit. However, laparoscopic dissection of endometriosis requires a high level of training and surgical experience as well as an excellent knowledge of pelvic anatomy in order to maximize benefits of the procedure and minimize surgical complications.
This article reviews the surgical challenges associated with extirpative surgery of endometriosis and briefly discusses surgical management of bowel and urinary-tract involvement.
Decision to Proceed with Ovarian Conservation
Hysterectomy with bilateral salpingo-oophorectomy was previously regarded as definitive therapy for treating endometriosis. One of the main disadvantages of bilateral oophorectomy was symptoms of surgical menopause. When deciding whether to preserve the ovaries or not during hysterectomy in patients undergoing surgical management of endometriosis, the American College of Obstetricians and Gynecologists noted that ovarian conservation can be considered in patients undergoing hysterectomy if the ovaries appear to be normal. 2 Drawbacks to ovarian conservation include higher risks of symptom recurrence and need for reoperation in the future.
The most-common sites of recurrent lesions are the large and small bowels. 3 Older studies raised concern about increased rates of recurrent symptoms with ovarian preservation. In an older retrospective study, ovarian conservation was associated with a 62% likelihood of recurrent symptoms and a 31% chance of requiring additional surgical treatment. 4
In contrast to ovarian conservation, bilateral salpingo-oophorectomy was associated with a 10% chance of recurrence of symptoms and only a 4% likelihood of additional surgery. 4 However, more-recent data show that there is no increased risk of reoperation even after ovarian conservation. A 2008 study that followed 120 patients for a total of 7 years following surgery for endometriosis found no significant difference in patients requiring reoperation when comparing patients who underwent ovarian conservation versus those who had bilateral adnexectomy at the time of hysterectomy. 5 Therefore, in patients with normal-appearing ovaries, a hysterectomy with ovarian conservation and removal of the endometriotic lesions should be considered, particularly in premenopausal patients.
Surgical Technique and Challenges
Endometriosis can invade organs in the pelvis, including the bowel, the urinary bladder and/or ureters. This type of endometriosis is called, deeply infiltrating or deeply infiltrative endometriosis (DIE) because it is found deep within the tissue or organ. Figure 1 shows an example of rectovaginal endometriosis in sagittal T2-weighted magnetic resonance imaging in a patient with DIE. Rectovaginal endometriosis is the most severe form of endometriosis. 6 It is located between the posterior wall of the vaginal mucosa and the anterior wall of the rectum, separate from the cervix.

Rectovaginal endometriosis in sagittal T2-weighted magnetic resonance image in a patient with deep infiltrating endometriosis (arrow). These are original pictures from patients the authors have been involved in their care.
When identifying lesions of deep endometriosis during surgery, important signs include evidence of fibrotic lesions (with or without characteristic dark spots), dense adhesions, reduced tissue elasticity, and hemorrhagic cystic structures. 7 Figure 2 shows an example of pelvic organs with extensive fibrosis as a result of endometriosis.
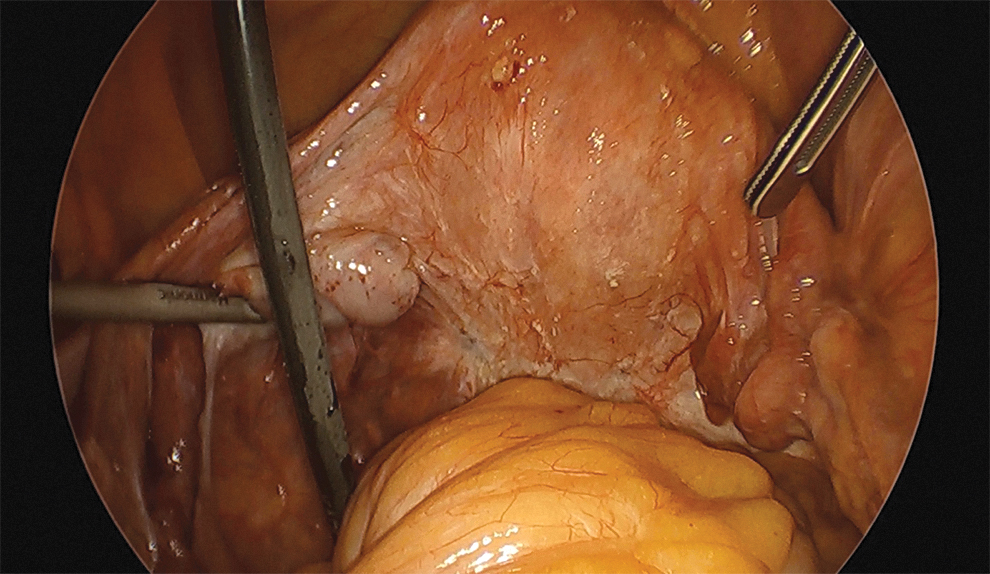
Pelvic organs with extensive fibrosis as a result of endometriosis. These are original pictures from surgeries the authors have been involved in.
The goal of extirpative surgery for patients with endometriosis is complete resection of endometriotic lesions. The lines of resection are primarily determined by the extent of disease spread. Some of the surgical challenges encountered during surgery include the extent of endometriosis, the presence of significant adhesions, and the presence of endometriosis-related fibrosis. Fibrotic changes related to endometriosis can result in retraction of surrounding structures. All of these factors distort the anatomy drastically and have to be taken into consideration during surgical planning and assessment of an optimal surgical approach (Fig. 3).
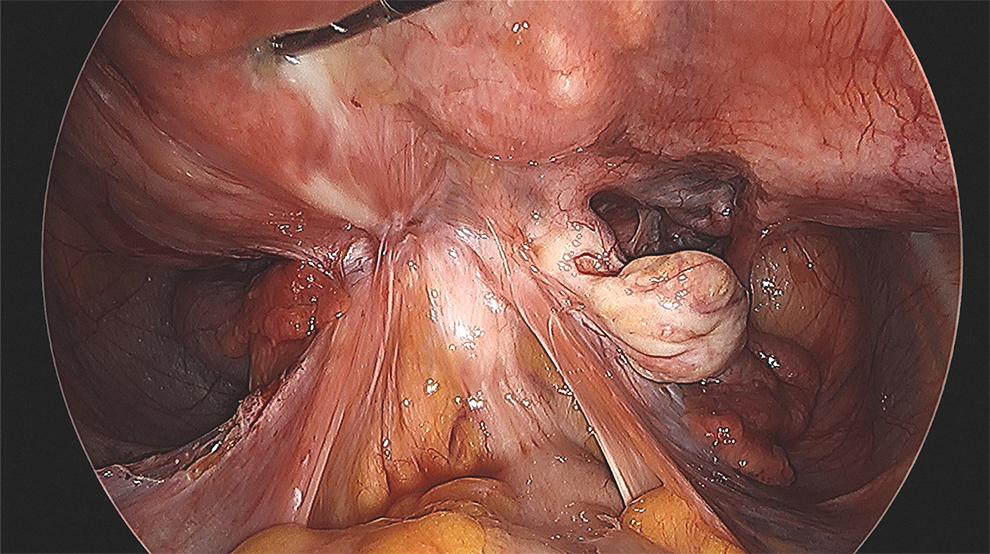
Significant anatomy distortion from deep endometriosis. These are original pictures from surgeries the authors have been involved in.
Very often, extensive dissection is necessary for reconstruction even prior to proceeding with hysterectomy and adnexectomy. In many cases, intestinal adhesiolysis and extensive ureterolysis may be required to reach the endometriotic lesion and to avoid iatrogenic injury to structures close to the margins of the endometriotic lesion. For this reason, a solid foundation and understanding of pelvic anatomy is paramount.
As previously stated, some of the surgical challenges encountered during extirpative endometriosis surgery are related to anatomical distortion. The ureter can be displaced medially due to surrounding fibrosis. Furthermore, ureteral stricture or complete obstruction may lead to hydroureter and hydronephrosis. 7 When the sigmoid and the rectum are involved, endometriotic nodules in the rectovaginal septum can result in adherence of the rectosigmoid to the lower dorsal side of the uterus, cervix, and vagina. 7 Endometriotic nodules can also be present in the vesicouterine pouch. Involvement or invasion of surrounding structures such as the underlying urinary bladder can cause displacement of the round ligaments medially and can cause challenges during development of a bladder flap during a hysterectomy.
When resecting deep endometriosis lesions, it is important to, first and foremost, identify all important anatomical structures in the pelvis, including the colon, small bowel, major vessels, nerves, adnexa, uterus, ureters, and bladder. Before being able to do so, the surgeon might need to start the dissection in areas free of disease and then divide the adhesions in order to restore the pelvic anatomy. For example, the mobilization of fixed ovaries on the pelvic sidewall improves the view of the operative field, particularly the lower structures in the cul-de-sac, which facilitates identification of the ureters.
To assist in restoring anatomy, the surgeon should have excellent knowledge of retroperitoneal anatomy to dissect the avascular retroperitoneal spaces. The surgeon can find the uterine artery as the boundary between the pararectal and paravesical space (Fig. 4). The uterine artery can then be ligated or clipped at its origin of the hypogastric artery. This will assist in preventing bleeding when dissecting an obliterated cul-de-sac. The ureter can be identified as the medial border of the pararectal space. When an oophorectomy is being performed, the pararectal space should be developed so that the ureter is mobilized and in view during infundibulopelvic ligation. 8 In some cases of recurrent endometriosis, despite repeat medical and surgical treatments, a modified radical hysterectomy can be performed to remove all endometriotic lesions, including resection of the parametria. 9
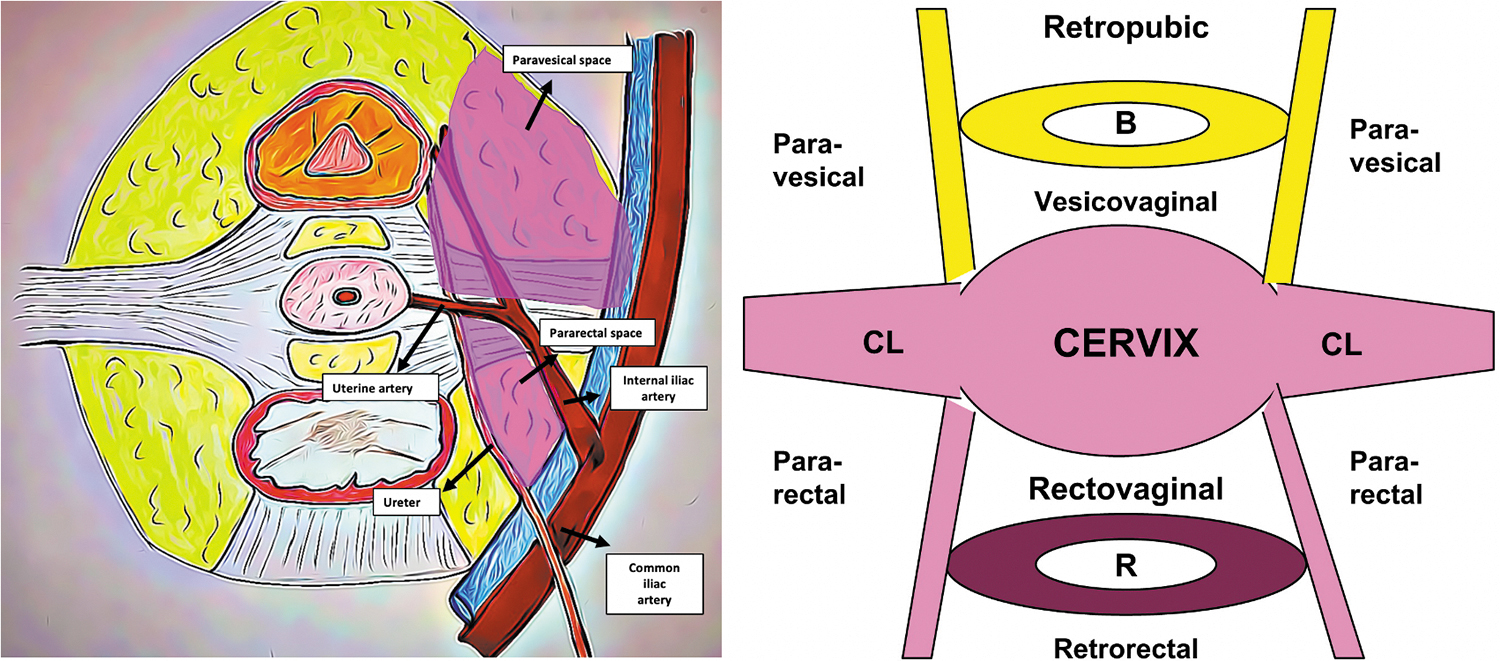
Boundaries of pararectal and paravesical space. B, bladder; CL, cardinal ligament; R, rectum.
Surgical Management of Gastrointestinal-Tract Involvement
The wall of the large intestine consists of multiple layers as illustrated in Figure 5, all of which can be invaded by endometriotic tissue. 10
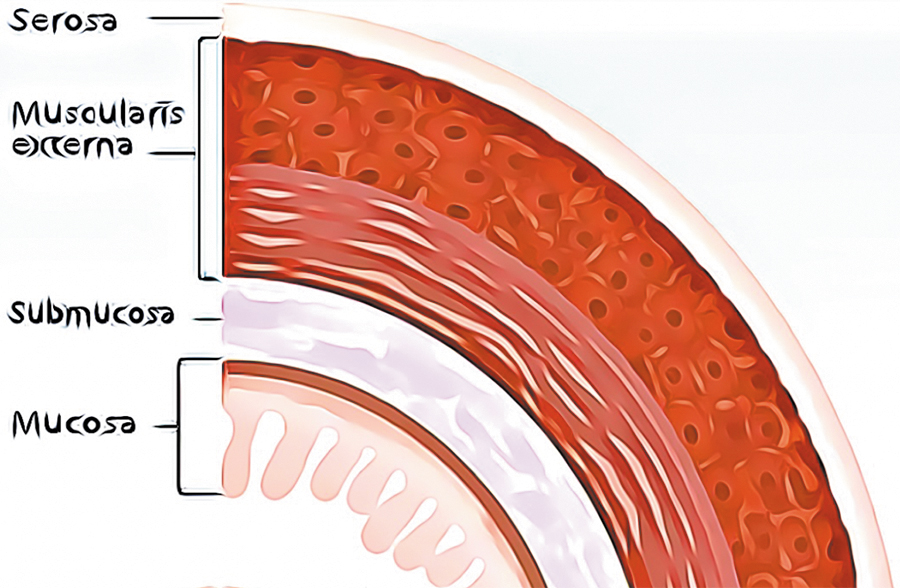
The wall of the large intestine consists of multiple layers: serosa; muscularis externa; submucosa; and mucosa.
Surgical removal of deep endometriosis is required when lesions are symptomatic, impairing bowel, urinary, sexual, and reproductive functions. Although several surgical techniques, such as laparoscopic bowel resection, disc excision, and rectal shaving have been described, there is no consensus regarding the choice of technique or the timing of surgery. 10 A randomized controlled trial involving 60 patients randomized to have either conservative surgery or radical rectal surgery showed no difference in functional outcomes when conservative surgery was compared to radical rectal surgery for DIE involving the bowel. 11
Rectal shaving consists of the separation of the endometriotic deep infiltrating nodule from the anterior part of the rectum to reach the cleavage plane. The technique for rectal shaving has been approached differently among surgeons, with some including shaving up to the rectal muscularis and others including resection of the nodule beyond the muscularis to the opening of the lumen of the digestive tract. 12 Prior to rectal shaving, it is often necessary to free lateral spaces and perform ureterolysis, as ureteral involvement has been found in 10% of cases with rectal nodules >3 cm. Shaving can be performed using a CO2 laser, cold scissors, an ultrasonic scalpel, or monopolar energy. The mean size of rectal lesions has been found to be 2–3 cm. Complications can include bowel perforation or a rectovaginal fistula. 10
Disc excision is a technique involving full-thickness rectovaginal deep endometriosis excision and is performed in 1 of 2 ways. The technique that was first introduced involved bowel lumen opening, followed by suture of the bowel. Other surgeons now prefer to use a stapler10,12 either a transanal end-to-end anastomosis (EEAtm) stapler (Ethicon Endo-Surgery, Cincinnati, OH, USA) or the Rouen technique using the Contour® Transtartm stapler (Ethicon Endo-Surgery). These techniques often use a combined laparoscopic and transanal approach.
Rectal shaving may be performed laparoscopically as a first step. If, after rectal shaving, the rectal wall is still infiltrated by deep endometriosis implants, full-thickness disc excision is then performed. An advantage to using transanal staplers is that the bowel is never opened, as both sections are stapled. The Contour Transtar stapler allows for larger disc excisions of 5–6 cm when the shaved area is located between 8 and 10 cm above the anus. In contrast, the EEA circular stapler removes discs 3 cm in diameter located in the upper rectum and rectosigmoid junction. The rate of rectovaginal fistula formation after disc excision is known to be higher than those patients managed by shaving and similar to that of segmental resection. 10
Segmental resection is utilized for advanced stages of rectovaginal deep endometriosis, when the infiltration is large. The technique for colorectal resection was described in 1992 by Nezhat et al. 13 Pararectal spaces are opened longitudinally, medially from the uterosacral ligaments and inferior hypogastric plexus, to preserve bladder, vaginal, and rectal innervation. The nodule is then detached from surrounding structures, and the rectum is sectioned with a 1–2- cm short healthy rectal margin. Colorectal anastomosis is generally carried out using transanal circular staples, and a rectal air test is used to check the quality of the colorectal suture. A diverting stoma may need to be created temporarily. 10 Two major complications include rectovaginal fistulas and bowel leakage. The lower the bowel infiltration, the higher the risk of a fistula. 10
Surgical Management of Urinary-Tract Involvement
Preoperative imaging is very important for identifying the exact location of endometriosis involving the urinary tract. For example, the presence of hydronephrosis provides information on potential involvement of the ureters and the pelvic sidewall. Intraoperatively, it is usually easy to identify endometriosis involving the bladder, as bladder endometriosis nodules are typically visible immediately.
Another sign of bladder involvement is the round ligaments being pulled medially, obliterating the ventral compartment due to fibrosis. The bladder first needs to be dissected away from both the uterus and the ventral wall of the vagina, thus opening the vesicovaginal space. Once the nodule is isolated and the bladder mobilized, the nodule is grasped with traction and excised with macroscopically free margins. 7 The bladder defect is then closed horizontally with a running absorbable suture.
If ureteral endometriosis is suspected preoperative, placement of ureteral stents is recommended by most experts. A systematic review, by Cavaco-Gomes et al., summarizes current evidence about laparoscopic management of ureteral endometriosis. The reviewers opined that ureterolysis alone was a sufficient procedure for 579 of 668 patients (86.7%), and in the remaining 89 patients, ureteral resection was necessary. 14
Ureterolysis is performed by freeing the ureter and excising the surrounding fibrotic tissue. This is typically performed when there is extrinsic ureteral endometriosis, or endometriosis that involves the periureteral tissue. Conversely, intrinsic ureteral endometriosis is characterized by endometrial tissue present in the lamina propria or tunica muscularis of the ureter. It is important to use either cold scissors or low thermal-energy sources (e.g., CO2 laser, plasma) when dissecting the ureter in order to minimize the risk of damage to its microvasculature. 7 In cases when there is a failed ureterolysis or when intrinsic ureteral lesions are far from the bladder, segmental ureteral resection with end-to-end anastomosis is necessary. Intrinsic ureteral endometriosis lesions close to the bladder that require resection will need reimplantation of the proximal end of the ureter into the bladder, a process called ureteroneocystostomy.
Conclusions
Endometriosis is a debilitating disease and a significant health problem for women of reproductive age. Because endometriosis is a chronic disease, medical treatment should be the first choice, while surgical procedures should be reserved for patients whose conditions do not respond to conservative treatments and whose symptoms greatly affect their quality of life. Extirpative surgery of endometriosis is typically offered to these patients. Although surgical management is an important treatment option for patients with endometriosis, the complexity of the surgery confers multiple challenges to even the most experienced of surgeons. A high level of training and surgical experience as well as an excellent knowledge of pelvic anatomy is paramount in order to maximize benefits of the procedure and minimize surgical complications for patients.
Footnotes
Authors' Contributions
Drs. Casas Diaz and Savoni contributed to the search of relevant publications for literature review; drafted assigned sections of the article, content; and assisted in submitting all required portions of article and supplemental documents for publication. Dr. Casas Diaz created figure and images for the article using Power Point and Photoshop. Dr. Morozov provided expertise in the field to other authors regarding relevant sections and topics to cover in the article, and reviewed and approved the final version of the article prior to submission. All 3 authors and revised the article critically for important intellectual content.
Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was provided for this project.