
Abstract
Objective:
The standardized infection ratio (SIR) is “the ratio of observed number of infections (events) to the predicted number of infections (events) for a summarized time period.” Between 2019 and 2020, the SIR decreased by about 5%, according to the National Healthcare Safety Network's healthcare-associated infection progress report. Although surgical-site (SSI) infections decreased, they contribute notably to postoperative complications. Patients with SSIs are more likely to have longer hospital stays, increased morbidity, or die. Studies have explored SSI risk factors and prevention techniques; however, no studies combined known prevention techniques for perioperative management, including antibiotic prophylaxis, preoperative preparation, and postoperative irrigation. This study examined a cost-effective, systematic perioperative protocol for reducing SSIs.
Materials and Methods:
This prospective-cohort case-controlled study compared 2 perioperative management protocols between 2019 and 2020 to determine if implementation of new measures reduced the incidence rate of SSIs.
Results:
From 2019 through 2020, there was a reduced rate of SSIs. A linear-regression analysis showed an association of SSIs with malignancies and smoking. Even with the small number of SSIs that occurred, the length of hospital stay and readmission for these complications was significant while there was no mortality.
Conclusions:
The integrative novel protocol in this article should be explored by other members of the gynecologic surgical society with expanded research. (J GYNECOL SURG 38:299)
Introduction
Surgical-site infections (SSIs) are “infections at or near surgical incisions within 30 days of a procedure.” 1 SSIs not only affect patient outcomes directly, but also make an impact on hospital costs.1–4
The standardized infection ratio (SIR) is “the ratio of observed number of infections (events) to the predicted number of infections (events) for a summarized time period.” 5 Between 2019 and 2020, the SIR decreased by about 5%, according to the National Healthcare Safety Network's healthcare-associated infection progress report. 2
SSIs can be subdivided further into 3 categories: (1) superficial-incision SSIs that involve only skin or subcutaneous tissue; (2) deep-incision SSIs that occur beneath incisions in the muscles/tissues just below these areas; and (3) organ/space SSIs that can be in any area of the body except the skin/muscle/tissue surrounding the site of the surgery, including spaces between organs. 3 The current study focused on organ/space SSIs and superficial SSIs as these were the most commonly encountered SSIs during the study timeperiod. Interventions for this study were targeted to reduce infections that were in these 2 categories of SSIs.
Reducing the incidence of SSIs has been studied previously for many surgical specialties with the aim of improving outcomes. These studies have found benefit in preoperative antibiotic regimens, preparation of patients with antiseptic agents, use of sterile draping, and other commonly known measures. There has not been a study with a complete perioperative protocol specific to gynecologic surgery.
A novel perioperative protocol that improves outcomes for gynecologic patients and reduces poor outcomes for physicians and hospitals was implemented for the current study. There is significant morbidity and mortality associated with SSIs; although most of these infections can be treated with drainage of abscesses or antibiotic management, there is still a 3% mortality rate. 1
In addition, the cost of an SSI can be significant. These infections can extend hospital stays by 9.7 days and increase cost of admission by $20,842, for a total additional hospital cost exceeding $900 million. 4 It is always the goal of physicians to do best for their patients, but these financial setbacks can also be a significant issue with respect to hospital spending if they are not addressed. The measures that were applied during the current study involved minor changes taking a minimum amount of increased time spent in preparation and intraoperatively, with the potential to save hospitals large amounts of money with interventions aimed at primary prevention. There is little standardization with respect to wound irrigation at the time of surgery; thus, a “gold standard” is still missing. 6
Despite persistent efforts to reduce SSIs, this still remains an issue for surgeons. An article published in 2017 by Till et al. found that, “cefazolin plus metronidazole resulted in lower surgical site infection rates after hysterectomy compared with cefazolin or second-generation cephalosporin.” 7 This was one component of the current study's protocol change.
In addition, chlorhexidine surgical preparation involves a limited amount of antiseptic per applicator; which led to initiating the use of additional applicators according to each patient's increasing body mass index and subsequent surface area to prepare for a surgical procedure.
Irrisept,® a novel irrigation solution, was also used in this perioperative protocol. The aim was to prevent formation of SSIs by irrigation with diluted chlorhexidine (which is bacteriostatic at low concentrations). 8
Materials and Methods
This prospective-cohort, case-controlled study compared 2 perioperative management protocols between 2019 and 2020 (Fig. 1) to determine if implementation of new measures reduced the incidence rates of SSIs.
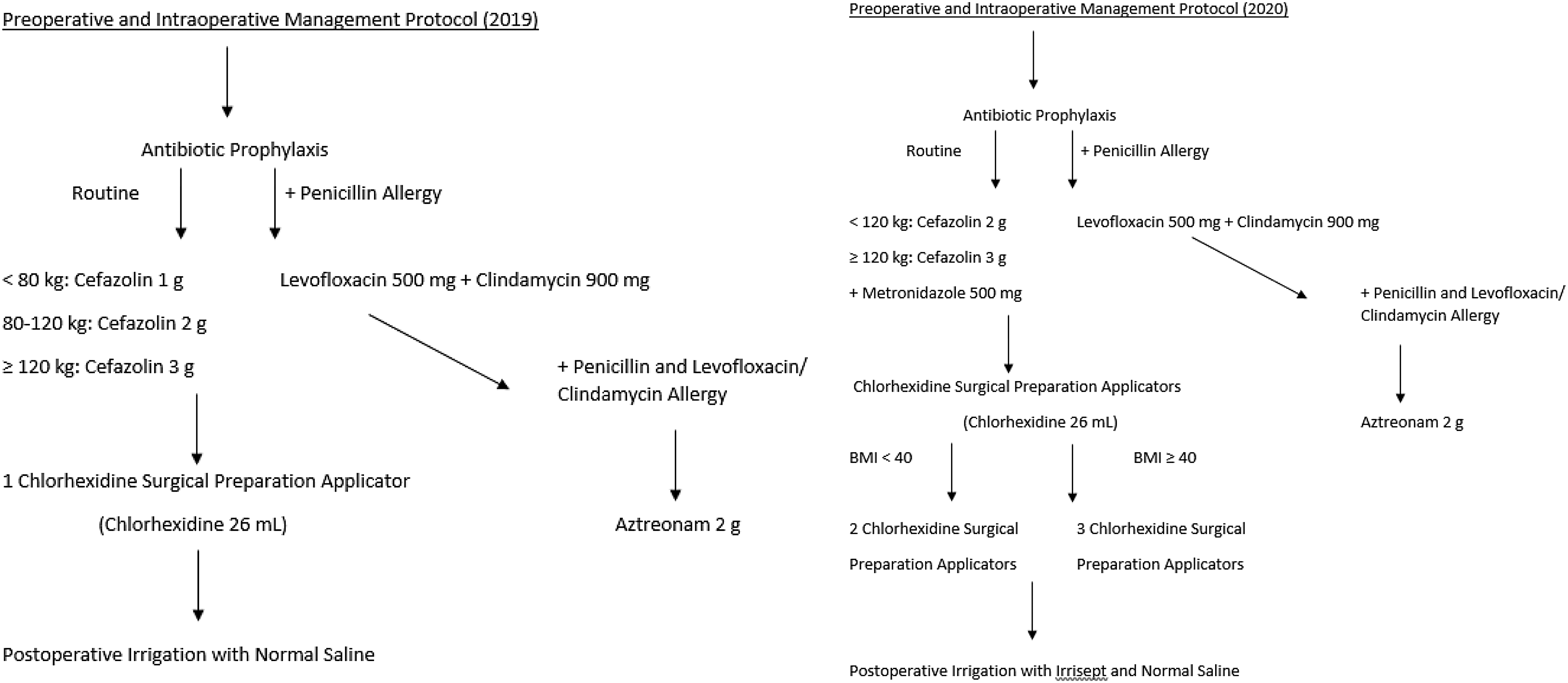
Preoperative and intraoperative management protocols for 2019 and 2020. BMI, body mass index.
New measures in the 2020 protocol included:
Expanding preoperative antibiotic coverage to include cefazolin and metronidazole (previously only cefazolin) Altering dosage of preoperative antibiotics so patients who weigh <120 kg receive 2 g of cefazolin and those who weigh >120 kg receive 3 g of cefazolin Increasing the number of preoperative chlorhexidine surgical preparation applicators so patients who are morbidly obese (body mass index [BMI] are >40 kg/m2) are cleansed with 3 applicators and all other patients are cleansed with 2 applicators Intraoperative use of Irrisept for peritoneal irrigation with normal saline upon completion of procedures.
Irrisept is chlorhexidine gluconate (CHG) 0.05% in 0.9% saline. This product is advantageous due to it being a potent antiseptic with broad-spectrum antimicrobial activity, while not inflicting damage to a patient's natural tissue. 6 The product has been approved by the U.S. Food and Drug Administration (FDA).
Finally, patients with penicillin allergy (n = 49) received levofloxacin and clindamycin or aztreonam instead of cefazolin.
The study included women who underwent a surgical procedure at the Cabell Huntington Hospital (CHH) in Huntington, WV, USA, between January 2019 and December 2020. Cohort 1 included surgical patients from January 2019 to December 2019. Cohort 2 included surgical patients from January 2020 to December 2020. All surgeries were performed by the same gynecologic oncologist and assisted by obstetrics and gynecology resident physicians, and medical students from the Joan C. Edwards School of Medicine at Marshall University, also in Huntington.
Procedures performed included robotic-assisted total hysterectomy (95%), robotic-assisted mass excision (0.003%), robotic-assisted salpingo-oophorectomy (0.0017%), robotic-assisted lymph-node dissection (0.004%), robotic-assisted colon resection (0.009%), robotic-assisted sacrocolpopexy (0.004%), diagnostic laparoscopy (0.003%), total laparoscopic hysterectomy (0.005%), laparoscopic cystectomy and salpingectomy (0.001%), laparoscopic-assisted vaginal hysterectomy (0.001%), laparoscopic salpingo-oophorectomy (0.003%). The majority of surgeries performed were the robotic-assisted total hysterectomies.
The overall SSI rate was also studied to assess associated variables that were notable risk factors. The 2 groups in this study were divided into SSI or no SSI. The following demographic information and pre/intra/postoperative variables were collected to assess the overall cause–effect relationships between the new measures and surgical site infections: age; BMI (kg/m2); smoking status (currently smoking cigarettes, electronic cigarettes, cigars or pipes); penicillin allergy status (any reported adverse reactions); total time on the surgical console (in minutes); benign or malignant diagnosis; length of hospital stay (in days); and presence and type of SSI.
The study was approved by the Marshall University institutional review board in an expedited review.
Results
Cohorts 1 and 2
Cohort 1 consisted of 402 women who underwent surgical procedures prior to implementation of the new measures to the perioperative management protocol. Cohort 2 consisted of 358 women who underwent surgical procedures after implementation of the new measures to the perioperative management protocol. Patient demographics and perioperative variables were similar for both samples, 2019 and 2020 (Tables 1–3).
Patients' Demographics and Preoperative Variables
Note: All data are presented as mean or n (%). p-Values are based on a 2-samples t-test, a Wilcoxon rank-sum test, or a Fisher's exact test.
BMI, body mass index.
Intraoperative Variables: Total Times on Console
Note: All data are presented as mean. p-Values are based on a 2-sample t-test.
min, minutes.
Postoperative Variables
Note: All data are presented as mean or n (%). p-Value is based on a Wilcoxon rank-sum test or a Fisher's exact test.
Wilcoxon rank-sum test was performed because hospital length of stay is a nonparametric variable.
SSI, surgical-site infection.
SSI versus non-SSI
A logistic regression analysis was completed to determine if a variable was associated with development of an SSI (Tables 4 and 5). Women who were diagnosed with a malignancy were 13 times more likely to develop an SSI than those with a benign diagnosis. The odds ratio (OR) was 13.02 (95% confidence interval [CI]: 1.58–107.02; p = 0.017). While smoking was not statistically significant, women who smoked were 3 times more likely to develop an SSI than those who did not smoke. The OR was 3.37 (95% CI: 0.82–13.82; p = 0.092).
Patient Demographics as Preoperative Variables
SSI, surgical site infection; yrs, years; BMI, body mass index; LOS, length of stay; d, days.
Postoperative Variables
Note: All data are presented as mean or n (%). p-Value is based on a-2 sample t-test, a Wilcoxon rank-sum test, or a Fisher's exact test.
SSI, surgical-site infection.
The overall SSI rate prior to the implementation of the new measures to the perioperative management protocol was 1.24%. After the implementation of the measures, the overall SSI rate declined to 0.84% (p = 0.729). See Table 6. This study had 8% of the needed power to detect a significant difference in SSIs between the groups. Therefore, there is a high likelihood of a Type 2 error. A difference existed, but it was not possible to detect it due to the small number of women included in the study. It was calculated that a sample size of ∼20,000 patients (with 10,097 patients in each group) would have been required to provide 80% power to detect a significant difference between the groups.
Surgical Site Infection Rates
Note: All data are presented as mean or n (%). p-Value is based on a Wilcoxon rank-sum test or a Fisher's exact test.
SSI, surgical-site infection.
There are many variables in surgery that can play a role in SSIs. There are also many different strategies used to reduce the rate of SSIs. This novel perioperative protocol was 3-tiered, focusing on (1) antibiotic prophylaxis, (2) antiseptic skin preparation, and (3) postoperative irrigation with the Irrisept solution. The final results after statistical analysis showed a reduction in the overall SSI rate from 1.24% (2019) to 0.84% (2020).
The logistic regression analysis enabled an analysis of risk factors. There was an association between malignancy and SSIs, and also between smoking status and SSIs. The OR for benign versus malignancy was 13.07 (p = 0.017), indicating that patients with malignancies were 13 times more likely to develop SSIs. The OR for SSI based on smoking status was 3.37 (p = 0.02), indicating that patients who smoked were 3.4 times more likely to develop SSIs.
Discussion
These results are important to share with the surgical community because of the reduced rate of SSIs that occurred. To the current authors' knowledge, an integrative protocol had not been studied for gynecologic procedures until the current study.
Standardization with this protocol can be shared among gynecologic surgeons for implementation. There have been studies showing that antibiotic prophylaxis with cefazolin + Flagyl® with weight-based dosing resulted in lower SSI rates after hysterectomy, and chlorhexidine has been shown to be superior in studies comparing it with another common skin antiseptic, povidone iodine. 9 Chlorhexidine has a wide array of known uses, but recent attention is on Irrisept as a routine irrigant after its FDA clearance. 6 Given what is known about these agents, the strategic combinations were used for the perioperative protocol.
Strengths
Strengths of the study included a protocol with components that have all been studied individually and shown to reduce SSIs successfully and independently. The demographics of the patients, surgeon, type of surgery, time spent intraoperatively, and benign versus malignant disease were similar between cohorts 1 and 2, as no statistically significant difference was noted. It is important that the comparative groups were similar, thus, the decreased SSI rate was not attributable to patient causes.
Limitations
The limitations of this study included its multi-intervention character. Each of these interventions have produced reductions of SSIs independently, but it was not possible determine if any one aspect of the protocol was key. This was not a significant issue, however, as these interventions did not incur significant increased costs to the hospital or procedure process. The most notable issue with this study was the small incidence rate of SSIs in the sample population. This study would have had more-powerful implications if the results had reached statistical significance. To reach this statistical significance, 20,000 datapoints would have been needed to to reach a power of 80%. The best way to study this novel protocol further would be a multisite study to incorporate more datapoints to reach this appropriate power.
Conclusions
SSIs comprise a preventable cause of morbidity and mortality in surgical patients. These infections cause increased costs of hospital stays and cause distress to both patients and physicians. There is no standardized protocol for preventing SSIs in gynecologic procedures. This protocol combined 3 known techniques to reduce SSIs to create a 3-tiered novel approach.
Although there were a limited number of SSIs in this study, it is still important to note the decrease in the rates of SSIs made between 2019 and 2020. The logistic regression confirmed what has already been documented and understood in the literature about the increased risk of postoperative complications. This knowledge can be used to counsel patients about smoking and increased risk of infection, and, thus, the benefits of smoking cessation. In addition, malignancy showed a significantly increased OR for infection, a phenomenon that may be multifactorial.
Overall, an indepth statistical analysis confirmed that a multisite study would be necessary to reach the number of datapoints needed (20,000). The cost difference between the preparation/antibiotic regimen/postoperative irrigation was minimal, while the average costs of hospital readmission, imaging, possible interventional radiology procedures, and need for reoperation can be significant.
In addition to the cost-benefit of reducing SSIs, the improved patient safety that would be provided is the ultimate goal. These preliminary data with the low number of SSIs show great promise for the novel perioperative protocol described herein. It is the authors' hope that these data can be shared with other surgical communities to expand implementation and decrease hospital costs and patient morbidity.
Footnotes
Authors' Contributions
All authors contributed to data collection, analysis, and article composition.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
This project received no funding.